


RESTORE™
A precision peptide protocol formulated for active tissue repair. Delivered sublingually via our VERISORB™ matrix, members report accelerated recovery, reduced joint discomfort, and improved systemic resilience.
$124.00
30-day supply delivered monthly.Pause or cancel anytime.
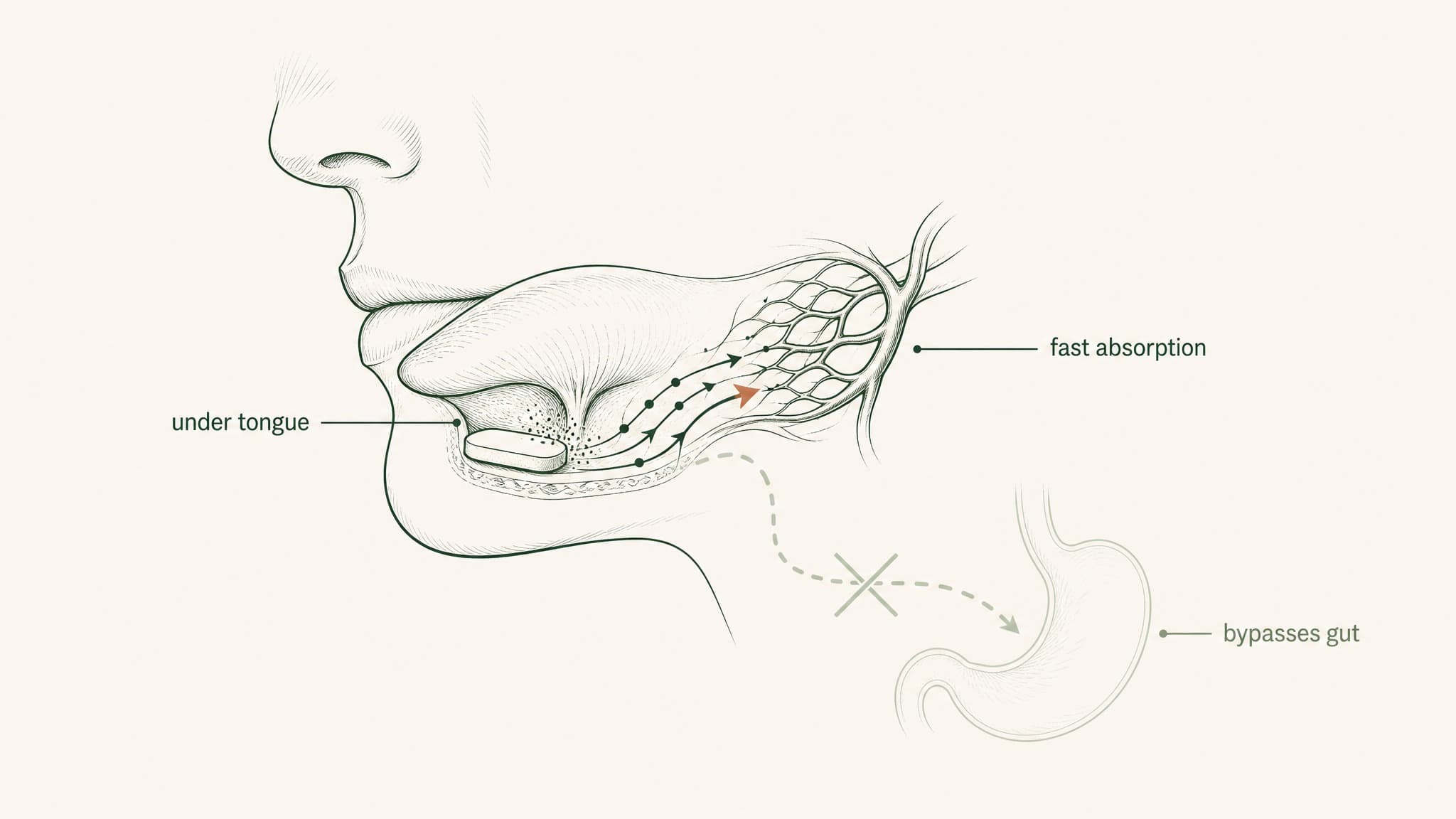
VERISORB™ vs. Standard Peptides
A swallowed peptide is mostly destroyed by your stomach before it can work. VERISORB carries it under your tongue and straight into your bloodstream, so far more of it actually does its job.
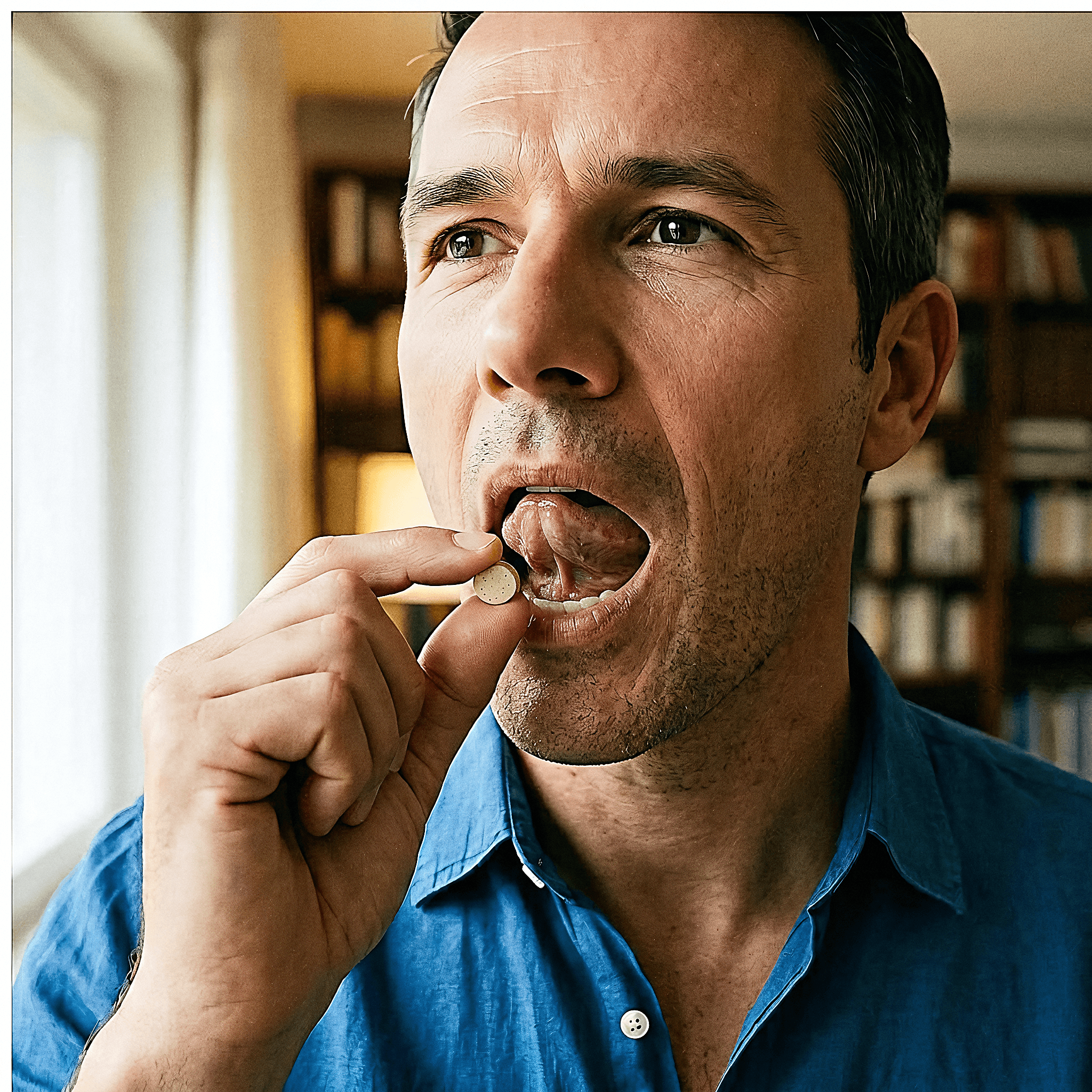
How to administer.
Prepare
Remove single tablet from climate-stable packaging.
Position
Place the rapid-dissolve tablet directly under your tongue.
Dwell
Hold for 30–60 seconds until completely dissolved. Do not chew.
Fast
Do not consume liquids or food for at least 15 minutes post-dose.

What members report.
Week 1
Initial systemic awareness. Biological baseline shifts.
Week 1
Systemic AwarenessInitial systemic awareness. Biological baseline shifts.
Week 2
Accelerated cellular response. Noticeable reduction in joint discomfort.
Week 2
Early ResponseAccelerated cellular response. Noticeable reduction in joint discomfort.
Week 4
Peak saturation phase. Significant tissue recovery timelines achieved.
Week 4
Peak SaturationPeak saturation phase. Significant tissue recovery timelines achieved.
Week 8+
Sustained systemic resilience and compound structural repair.
Week 8+
Sustained BaselineSustained systemic resilience and compound structural repair.
Uncompromising Standards.
Pharmaceutical-Grade Sourcing
Active components synthesized in GMP facilities to exact purity specifications.
Third-Party Tested
Every batch undergoes rigorous independent analysis for potency and purity.View Lab CoA
FDA Lab Validated
VERISORB™ matrix structure validated by an FDA-accredited laboratory.
Not a Research Chemical
Formulations undergo full regulatory scrutiny without "not for human consumption" loopholes.
Compounding outcomes.
Each VERO protocol works in its own way, so you can safely take them together and stack the benefits.
"89% of members add LEGACY™ to stack tissue recovery with cellular vitality."

LEGACY™
NAD+Replenishes systemic NAD+ levels and drives mitochondrial function
Explore LEGACY™ ProtocolSubscribe & Save.
Results come from taking it consistently. Lock in our best price and never run out — a fresh supply arrives at your door every month.
- One-time shipment
- Standard shipping rates apply
- Retail pricing
- Automated delivery every 30 days
- Locked-in clinical direct pricing (17% off)
- Priority allocation from fresh lab batches
30-Day Guarantee.
We stand entirely behind VERISORB. If you don't feel a difference within your first 30 days of taking it consistently, we'll refund your first order. No questions asked.
Full PolicyFrequently asked.
Ready to start?
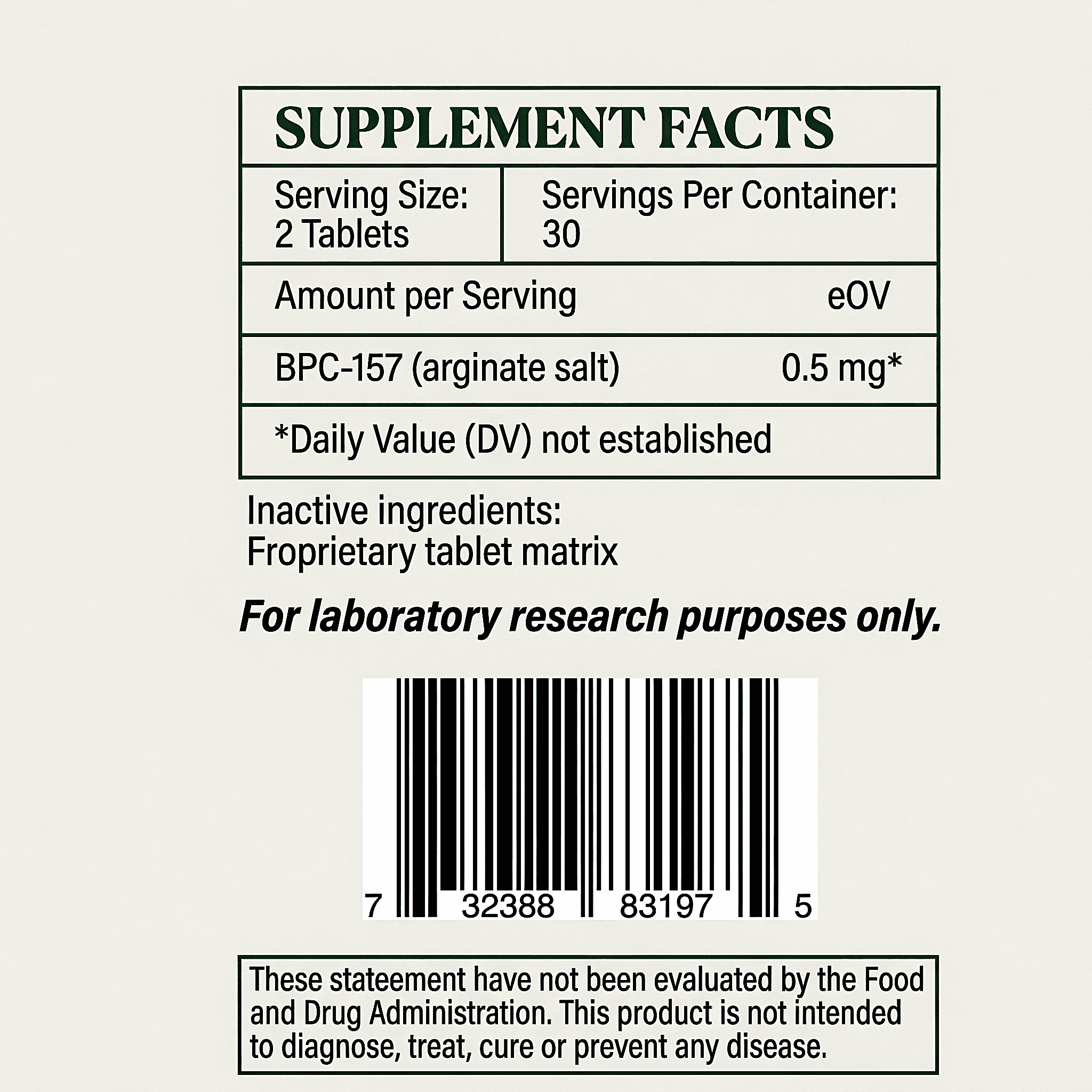
BPC-157 (arginate salt) targeted delivery protocol. Add to your configuration to lock in continuous delivery pricing.
Protocol Synergies.
Formulations operate on independent biological pathways, enabling systematic and safe stacking.
Related Research.
Verified-citation articles covering the compounds, mechanisms, and delivery science behind RESTORE™.