BPC-157 isn't FDA-approved, but its regulatory story just moved. Here's what the July 2026 compounding vote, the human trial gap, and the research actually show.
If you've looked into BPC-157 at all, you've probably hit the same wall: vague answers, forum arguments, and a regulatory picture that seems designed to confuse. It's one of the first things people ask about when they start looking at a structured recovery protocol, which makes the confusion especially frustrating.
The compound isn't banned. It isn't approved. And as of this month, its status just moved for the first time in years.
This is a plain walkthrough of where BPC-157 actually stands with the FDA right now, what changed on July 23, 2026, and what the underlying research looks like once you separate it from the noise.
Key Takeaways
- BPC-157 is not FDA-approved for any use in humans. No completed Phase 1, 2, or 3 human trials exist for it.
- On July 23, 2026, an FDA advisory committee voted 8-6 (with one abstention) to recommend BPC-157 be added to the list of substances compounding pharmacies can legally prepare, for a specific ulcerative colitis use case. That vote is not a decision, it's a recommendation the FDA can still reject.
- FDA staff themselves argued against the recommendation, citing insufficient human safety and effectiveness data.
- BPC-157 is not a scheduled controlled substance in the US. It's legally purchasable as a research chemical, separate from the compounding question above.
- Animal research on tendon, gut, and connective tissue repair is extensive and consistent. Human evidence is limited to one small retrospective review.
Exploring a research protocol built around recovery and cellular resilience? The RESTORE Protocol is where VERO members start. Explore RESTORE →
What BPC-157 Actually Is
Picture a long strand of pearls: that's a protein, hundreds of amino acids clipped together. Now snip out just fifteen of those pearls in a row, the exact sequence found in a much larger protein in human gastric juice. That fifteen-pearl fragment is BPC-157, a synthetic peptide researchers isolated and now manufacture in a lab.
Three things worth knowing before the regulatory story makes sense:
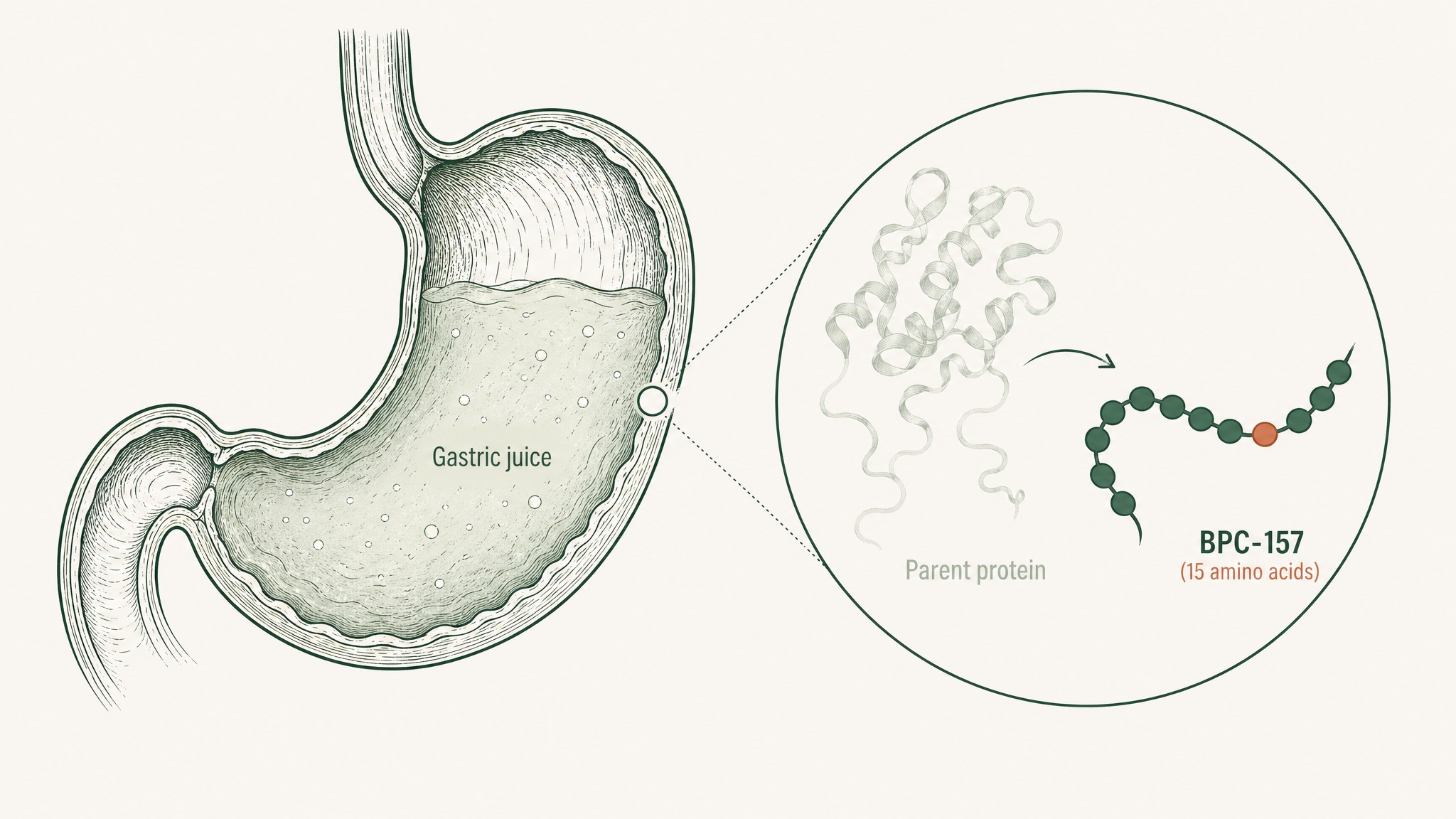
BPC-157 is a 15-amino-acid fragment isolated from a much larger protein found in stomach acid.
- It's a 15-amino-acid fragment, not a full protein.
- It's made in a lab today, not extracted from gastric tissue.
- Its natural origin is exactly why it's hard to patent, which turns out to be the whole story below.
The gastric-juice origin matters for two reasons. It's part of why researchers first got curious about gut protection and tissue repair. And, less obviously, it's the reason BPC-157 hasn't made it through FDA trials, more on that below.
BPC-157 isn't extracted from animals or plants, and it isn't a natural supplement in the herbal sense. What researchers work with today is a precisely manufactured, chemically defined molecule made in a lab.
What "FDA Approval" Actually Requires
Before getting into BPC-157 specifically, it's worth being precise about what "FDA approval" means, because the term gets thrown around loosely.
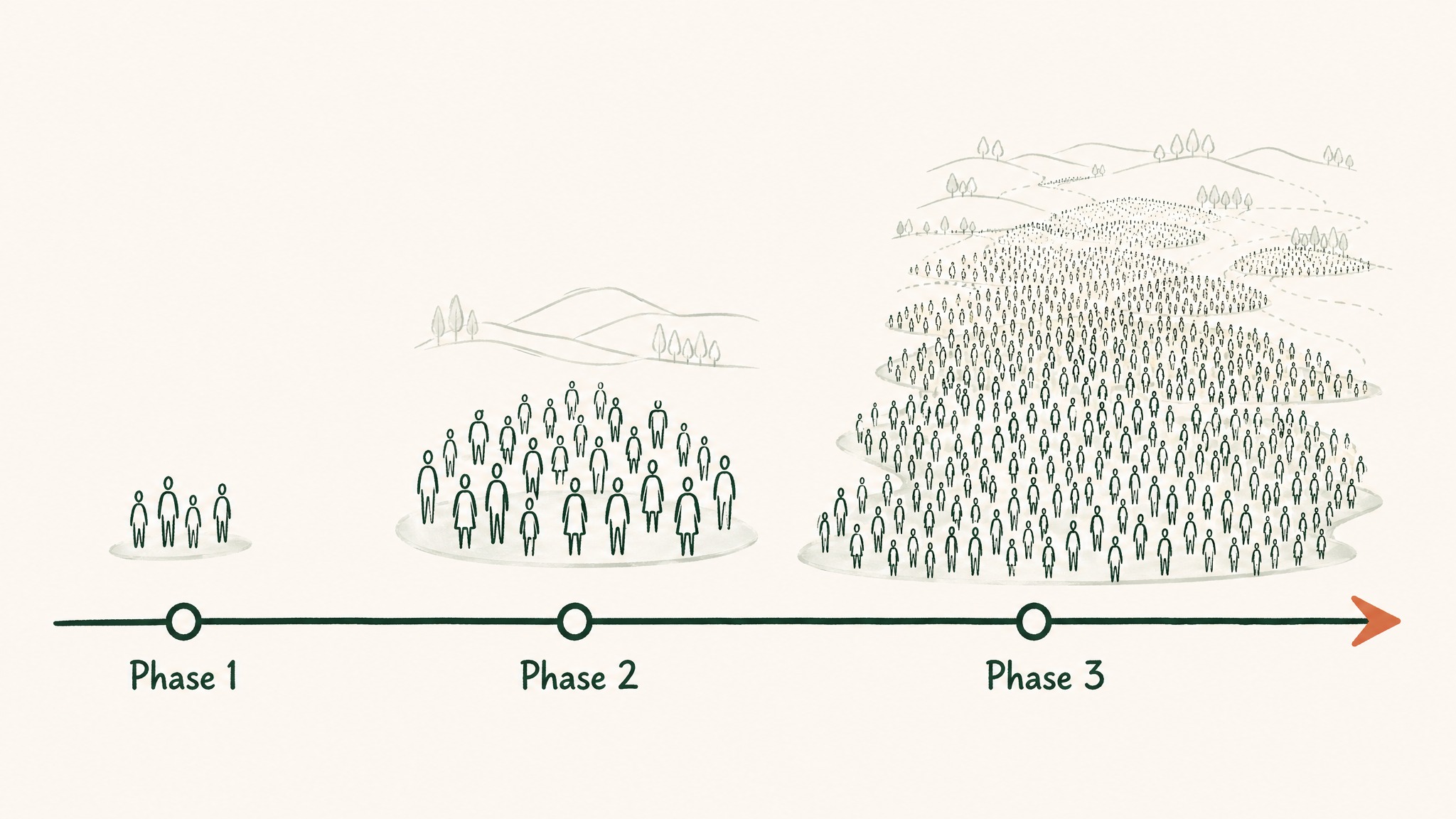
Getting a drug approved means clearing three phases of human trials, each one bigger and slower than the last:
- Phase 1 — a small group of people, checking whether the compound is safe at all.
- Phase 2 — a larger group, checking whether it actually works.
- Phase 3 — thousands of people across multiple sites, confirming it works and watching closely for side effects.
None of these three phases has ever been completed for BPC-157.
That full pipeline is not cheap. A 2020 JAMA analysis of 63 approved drugs put the median research and development cost at roughly $985 million, with the average pulled up to $1.3 billion by expensive categories like cancer drugs, some of which ran past $2.8 billion (Wouters et al. 2020, JAMA, PMID 32125404). BPC-157 has never entered that pipeline in the US.
That's a statement about where the evidence sits, not a verdict that the compound is dangerous. FDA approval requires human trial data. BPC-157 doesn't have it.
Why the Human Trials Haven't Happened
Here's where the story gets structurally interesting, and where blaming "regulatory obstruction" misses the actual reason.
Drug companies fund billion-dollar trials when they can lock in exclusive sales rights afterward through a patent. That patent is how they earn the investment back.
BPC-157 is a fragment of a naturally occurring human protein, which makes it very hard to patent in a way that gives any one company exclusive rights. Without that exclusivity, no pharmaceutical company has the financial incentive to spend a billion dollars proving it works. The compound isn't secret or unusually risky, it's commercially unattractive to the only entities with the resources to run the trials.
This pattern isn't unique to BPC-157. It shows up across naturally occurring compounds with promising research behind them: the biology looks interesting, but the business case for trials never closes, so the compound stays in a research grey zone. Curious readers are left with preclinical data and a real human-evidence gap rather than a clean approved-or-not answer.
The Compounding Pharmacy Track — And What Just Happened
There's a separate regulatory lane that matters here: compounding pharmacies, which prepare custom drug formulations for individual patients rather than mass-producing a product. They operate under Section 503A of the Food, Drug, and Cosmetic Act, and the FDA maintains a list of "bulk drug substances" these pharmacies are permitted or barred from using.
This is where the real news is. For roughly the past few years, BPC-157 sat in the FDA's Category 2 — a designation for substances the agency says raise "significant safety risks," which effectively blocks compounding pharmacies from touching it. Then, in a Federal Register notice published April 16, 2026, the FDA pulled BPC-157 (along with eleven other peptides, including TB-500 and Semax) out of Category 2 entirely and moved it into formal review by the Pharmacy Compounding Advisory Committee.
That committee met on July 23-24, 2026. Here's what happened:
- The panel voted 8-6, with one abstention, to recommend adding BPC-157 to the approved 503A compounding list — specifically for a defined ulcerative colitis use case, not for general use.
- FDA staff themselves argued against it. Their briefing documents cited a lack of evidence supporting BPC-157's effectiveness for that indication, plus gaps in substance-specific quality data.
- Committee votes like this are advisory. The FDA is not bound by them and will make its own final call.
Worth flagging: reporting from STAT News on the same vote noted that a majority of the panelists who voted in favor had ties to the peptide industry, a detail worth knowing as you weigh how much signal to take from an 8-6 split.
So where does that leave things? Out of Category 2, no longer treated as a flagged safety risk pending review, but not yet cleared either. "Recommended by committee" is a real step forward from "prohibited," and a long way from "approved."
What the Animal Research Actually Shows
While the human clinical record is thin, the preclinical picture, studies in animal models and cell cultures, is substantial and has held up across independent labs for over a decade.
A 2019 review in Cell and Tissue Research (Gwyer, Wragg & Wilson 2019, PMID 30915550) looked across tendon, ligament, and skeletal muscle studies and found consistently positive healing outcomes, while being upfront that the work has mostly been done in small rodent models and that human efficacy remains unconfirmed.
BPC-157 activates fibroblasts to migrate toward and repair damaged tendon tissue.
Research suggests the underlying mechanism runs through more than one pathway.
A 2011 study in the Journal of Applied Physiology (Chang et al. 2011, PMID 21030672) zoomed into tendon fibroblasts, the cells responsible for building and repairing tendon tissue, and found that in these rat-tissue and cell-culture experiments, BPC-157 dose-dependently activated what's called the FAK-paxillin pathway. In plain terms, that's a signalling chain that tells fibroblast cells to divide and move toward damaged tissue. In that same rat-and-cell-culture research, BPC-157 accelerated tendon-explant outgrowth and fibroblast migration.
On the gut side, a 2020 review in Current Pharmaceutical Design (Park et al. 2020, PMID 32445447) documented what researchers call BPC-157's cytoprotective effects, its apparent ability to help preserve the stomach lining against damage from NSAIDs like ibuprofen and aspirin, in animal models. Given that BPC-157 originates from gastric juice, researchers find that connection mechanistically coherent.
A few other things researchers keep coming back to, per a 2021 review in Frontiers in Pharmacology (Seiwerth et al. 2021, PMID 34267654) covering wound-healing research across skin, muscle, tendon, and connective tissue in animal models:
- BPC-157 was previously administered to humans in clinical trials for ulcerative colitis and multiple sclerosis, with no toxicity reported at the doses used.
- In separate animal safety testing, researchers never reached the "LD1" threshold, the dose at which 1% of test subjects die, even at high experimental doses.
- The compound's research footprint spans an unusually wide range of tissue types for a single molecule.
None of that is a substitute for controlled human trials. It's the reason researchers keep circling back to the compound.
The Human Evidence Gap — And What Actually Exists
It would be dishonest to write this without being direct: the human data on BPC-157 is thin. The animal research is genuinely interesting. It's still animal research.
The most-cited piece of human data is a 2021 retrospective chart review published in Alternative Therapies in Health and Medicine (Lee 2021, PMID 34324435). Researchers at a private clinic reviewed 16 patients who'd received intra-articular BPC-157 injections, meaning injected directly into the knee joint, for various types of knee pain between 2019 and 2020.
Among the 12 patients who received BPC-157 alone, 91.6% reported significant improvement. Across the full group of 16 (some of whom also received a second peptide), 87.5% reported relief.
Users report meaningful experiences in research contexts like this one, but the study's own authors were careful to frame it correctly: this was a retrospective chart review, not a randomized controlled trial, and they called for exactly the kind of larger study that hasn't happened yet.
A chart review is a data point. It isn't a conclusion.
The ulcerative colitis and multiple sclerosis trials mentioned above tell you BPC-157 has been given to humans before without raising safety red flags. But safety observations from early-phase work are a long way from the efficacy evidence the FDA requires for approval, or apparently, even for a compounding recommendation, based on what FDA staff argued in July.
The WADA Situation
One thread that comes up constantly: the World Anti-Doping Agency added BPC-157 to its Prohibited List in 2022 (Józwiak et al. 2025, Pharmaceuticals, PMID 40005999), under the categories covering non-approved substances and peptide hormones/growth factors. As of the Prohibited List currently in force for 2026, anti-doping resources continue to list it there, banned at all times, in and out of competition.
A doping ban and an FDA approval answer two completely different questions.
That's worth separating from the FDA story entirely. WADA prohibits substances based on suspected performance-relevant effects and a lack of approved medical status, a different bar than either FDA approval or a compounding recommendation. Its inclusion doesn't tell you anything new about safety or efficacy, only that anti-doping bodies are watching a compound they can't yet fully characterize.
What the Regulatory Picture Means for Researchers
The honest summary of where BPC-157 sits in 2026, at a glance:
- DEA: not a scheduled controlled substance. Legal to purchase as a research chemical.
- FDA drug approval: not approved. No completed human trials of any phase.
- FDA compounding (503A): out of the restrictive Category 2 as of April 2026; an advisory committee recommended it for a narrow ulcerative colitis use case in July, over FDA staff's own objections. Final decision still pending.
- WADA: prohibited since 2022, still listed on the current list.
None of that adds up to "approved" or "banned." It adds up to a compound that just cleared its first real regulatory hurdle in years, a non-binding recommendation, over the FDA's own staff objections, with the agency's final call still pending.
Members experience ongoing interest in this compound across multiple research domains, and the preclinical work has held up across independent groups for more than a decade. The clinical gap is real, though, and shouldn't be smoothed over.
Any engagement with BPC-157 by researchers today is for research purposes only. That's not boilerplate, it's an accurate description of where the compound sits in the evidence hierarchy right now.
The more interesting question isn't whether BPC-157 is "approved" or "banned." It's whether the FDA follows its own staff's objections or its advisory committee's recommendation, and what that decision does to compounding access from here.
That decision is worth watching.
Curious how VERO approaches BPC-157 research responsibly, within the current regulatory picture? See the RESTORE Protocol →
Frequently Asked Questions
Is BPC-157 legal to buy in the United States?
BPC-157 is not a scheduled controlled substance under US federal law, so it's legal to purchase as a research chemical. It cannot legally be sold or marketed for human therapeutic use, since it hasn't received FDA approval for any indication. Its status for compounding pharmacy use is a separate track that's still being decided.
What happened with BPC-157 and the FDA in July 2026?
On July 23, 2026, the FDA's Pharmacy Compounding Advisory Committee voted 8-6, with one abstention, to recommend BPC-157 be added to the list of substances 503A compounding pharmacies can legally use, specifically for an ulcerative colitis use case. FDA staff had recommended against this, citing gaps in effectiveness and safety data. The vote is advisory only, the FDA makes the final call and isn't bound by it.
Why hasn't BPC-157 been FDA approved if the animal research looks promising?
FDA approval requires completed Phase 1, 2, and 3 human clinical trials, a process that a 2020 JAMA analysis put at a median cost of roughly $985 million per drug. Because BPC-157 is derived from a naturally occurring human protein, it's very difficult to patent exclusively, which removes the financial incentive for a pharmaceutical company to fund those trials. This is a funding and patent structure problem, not a regulatory block based on known safety concerns.
What does the human research on BPC-157 actually show?
Human data is limited. The most-cited study is a 2021 retrospective chart review of 16 patients who received intra-articular BPC-157 injections for knee pain, in which 87.5% reported significant improvement. BPC-157 was also given to humans in earlier trials for ulcerative colitis and multiple sclerosis without reported toxicity, though those trials weren't designed to prove efficacy.
Researchers consistently note that larger randomized controlled trials are the missing piece.
How does BPC-157 work in animal research?
Research suggests BPC-157 acts through more than one pathway. In tendon tissue, studies in animal models and cell cultures show it activates the FAK-paxillin pathway, which prompts fibroblast cells to divide and migrate toward damaged tissue. In gastrointestinal tissue, animal studies point to cytoprotective effects that help preserve the stomach lining, consistent with the compound's origin in gastric juice.
Has BPC-157 shown any safety concerns in research settings?
Preclinical safety data is consistently reassuring across animal studies; a 2021 review in Frontiers in Pharmacology noted the LD1 threshold, the dose at which 1% of test subjects die, was never reached even at high experimental doses. Early human trials for ulcerative colitis and multiple sclerosis reported no toxicity. As with any compound lacking completed human trials, its long-term safety profile in people hasn't been formally established.
Can a compounding pharmacy legally prepare BPC-157 right now?
Not yet, formally. As of July 2026, an FDA advisory committee recommended BPC-157 be added to the approved 503A compounding list for a specific ulcerative colitis use case, but the FDA hasn't issued a final decision, and its own staff argued against the recommendation. Until the FDA rules, compounding access remains in a transitional, pharmacy-dependent grey zone.
Is BPC-157 banned by WADA for athletes?
Yes. The World Anti-Doping Agency added BPC-157 to its Prohibited List in 2022, and it remains listed under the current Prohibited List in force for 2026, banned at all times, in and out of competition. That's a separate question from FDA status, WADA's bar for prohibiting a substance isn't the same as FDA approval or compounding eligibility.
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.