
GHK-Cu, MOTS-c, and Epithalon are three signalling peptides your body makes less of as you age. Here's what researchers have actually found, verified citations, no fabricated PMIDs.
Something changes in how your body maintains itself between your twenties and your forties. It's not a single dramatic event, more like a slow dimmer switch turning down across multiple systems at once. The cells that repair your skin, the mitochondria generating energy in your muscles, the enzymes maintaining your chromosomes, they all depend partly on chemical signals that your body produces in gradually smaller amounts as the years pass.
A growing area of research focuses on a specific class of those signals: peptides that are measurably more abundant in younger bodies and that appear, in controlled research settings, to influence biological maintenance in ways worth documenting. This content is published for research purposes only. What follows covers three of those molecules, GHK-Cu, MOTS-c, and Epithalon, where the published record is solid enough to map honestly.
What "Age-Supportive" Actually Means
Think of the biology here as maintenance scheduling. Your body isn't static, it's constantly repairing damaged proteins, building new connective tissue, patching errors in DNA replication, and clearing out cellular debris. That maintenance doesn't happen automatically; it happens because specific signalling molecules tell it to.
Peptides are one class of those signals. When signal volume drops, some of those tasks happen less frequently.
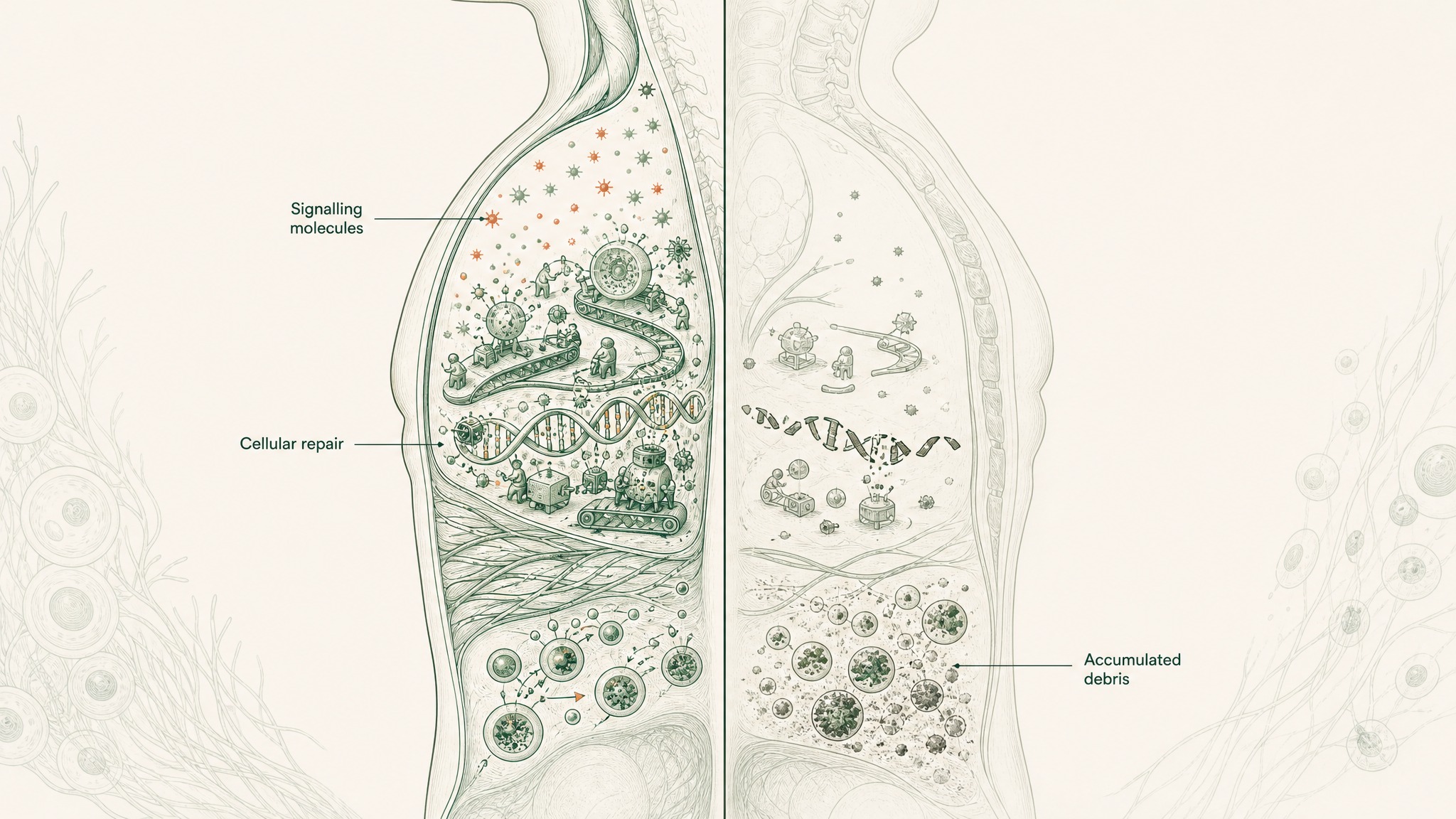
How cellular maintenance slows when signalling molecules decline with age.
The "age-supportive" label is a research frame, not a therapeutic claim. It describes peptides that share three characteristics:
- Endogenous production: your body already makes them, they're not foreign compounds
- Documented age-related decline: circulating levels are measurably lower in older versus younger individuals
- Research-documented biological effects: controlled settings show effects on cellular maintenance functions
Research suggests the decline in these specific signalling molecules is connected to changes in cellular repair efficiency, which is what makes them worth studying separately from the hundreds of other compounds that also vary with age. The three covered here are the ones where that case is currently strongest.
GHK-Cu: The Tissue Maintenance Signal
By the time you're 60, your body produces less than half the GHK-Cu it made in your twenties. That's a measured figure, not a rough estimate. Research published in the International Journal of Molecular Sciences documented circulating GHK levels at roughly 200 units per millilitre at age 20, falling to around 80 units per millilitre by age 60 (Pickart & Margolina, Int J Mol Sci 2018, PMC6073405).
That decline tracks closely with when your skin starts changing texture, when wounds take longer to close, and when tissue repair runs more slowly, because GHK-Cu is one of the primary signals your body uses to run those processes.
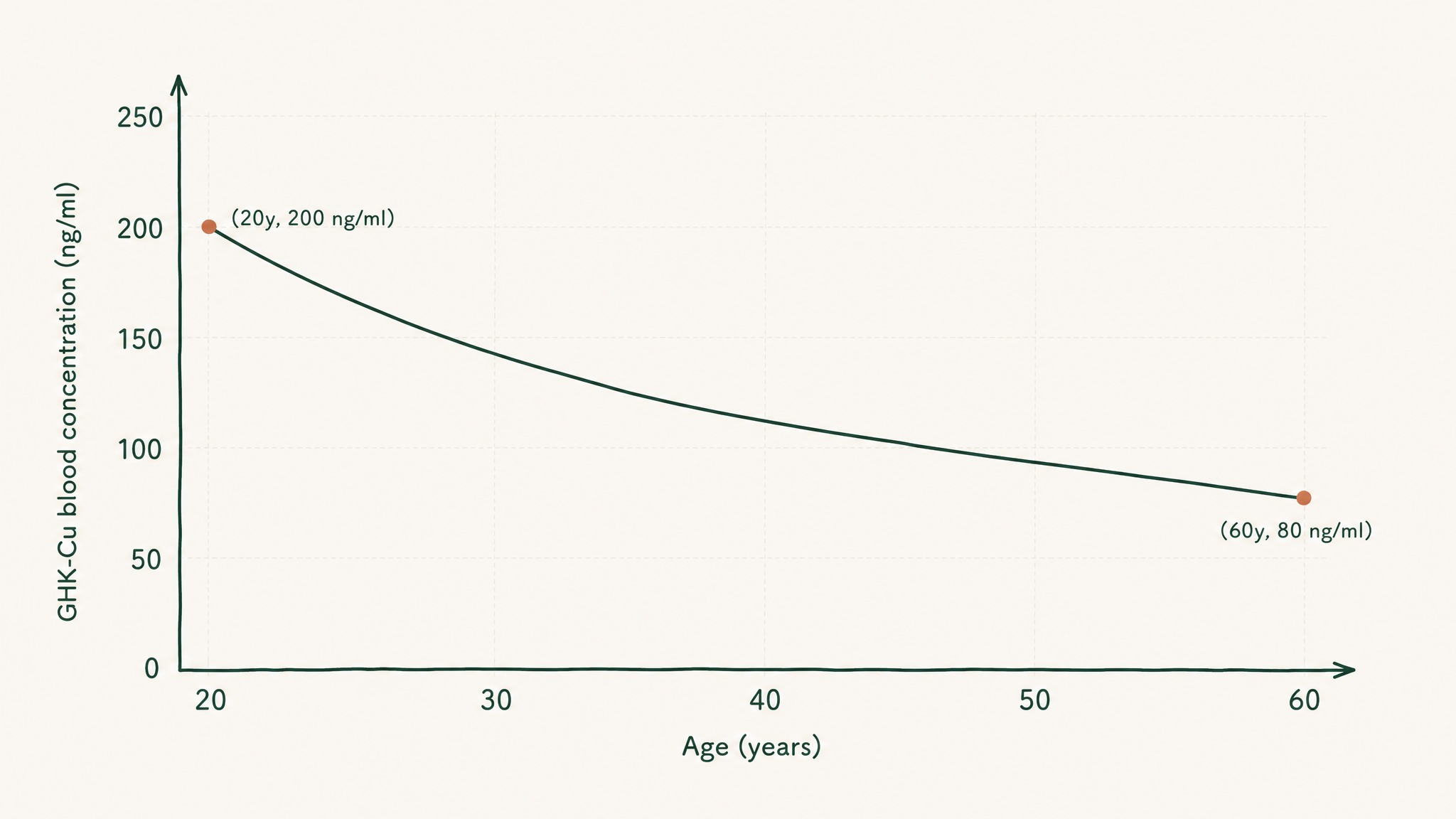
GHK-Cu levels drop from 200 units per millilitre at age 20 to 80 by age 60.
GHK-Cu is a tripeptide, three amino acids (glycine, histidine, lysine) attached to a copper ion. Your liver, skin, and plasma all produce it. Loren Pickart first isolated it from human serum in 1973 (Pickart & Thaler, Nat New Biol 1973, PMID 4349963).
What's unusual about GHK-Cu isn't the structure, it's the reach of what it influences.
A 2014 genomic analysis found that GHK changed gene expression by at least 50% in approximately a third of all human genes studied, covering tissue remodelling, antioxidant defence, inflammation signalling, and neurological maintenance (Pickart, Vasquez-Soltero & Margolina, BioMed Res Int 2014, PMC4180391). In human terms: it turns roughly a third of your genes up or down. That's an unusually wide reach for a molecule this small.
The research domains where GHK-Cu evidence is most developed:
- Wound closure and tissue remodelling after injury
- Collagen synthesis and skin matrix structural integrity
- Antioxidant gene expression, specifically the pathways that regulate SOD (superoxide dismutase) and catalase production
- Anti-inflammatory signalling in response to tissue stress
For a detailed look at GHK-Cu research and protocol considerations, the GHK-Cu copper peptide protocol guide covers it in full.
MOTS-c: The Mitochondrial Messenger
By your mid-forties, circulating MOTS-c levels are typically lower than they were during your peak years of physical activity. They track closely with how metabolically responsive your cells are to insulin, and MOTS-c isn't just a passive indicator of that. It's one of the signals driving it.
What distinguishes MOTS-c from every other signalling molecule in this article is where it comes from. Most peptides are encoded in your chromosomal DNA, the genetic blueprint inside your cell's nucleus. MOTS-c is encoded inside the separate, smaller genome inside your mitochondria, the structures that convert food into usable cellular energy.
MOTS-c travels from your mitochondria to your cell nucleus to coordinate energy and antioxidant defenses.
It's a 16-amino-acid peptide released from muscle tissue into the bloodstream. Your mitochondria, it turns out, aren't just passive energy factories. They send signals that regulate how the rest of your body runs.
The 2015 discovery paper from Changhan Lee's lab at the University of Southern California established the mechanism. MOTS-c activates AMPK, your cells' master energy-shortage sensor, by disrupting a specific internal carbon-accounting process. When AMPK switches on, cells absorb glucose more efficiently, burn fat more readily, and become more insulin-sensitive.
In the study's mouse models, that action reduced both age-related and diet-induced insulin resistance (Lee et al., Cell Metab 2015, PMID 25738459).
Three years later, the story got more complex, and more interesting:
- Under metabolic stress, MOTS-c doesn't stay in the cell's fluid. It travels to the nucleus.
- Once there, it activates NRF2, the master switch for your antioxidant gene programme.
- Both effects share the same upstream pathway (AMPK-dependent), meaning metabolic signalling and antioxidant defence are being coordinated through the same mechanism.
A 2018 Cell Metabolism paper by Kim, Son, Benayoun and Lee documented this nuclear translocation for the first time, the first described case of a mitochondrially-encoded peptide directly regulating nuclear gene expression (Kim et al., Cell Metab 2018, PMID 29983246). Two separate genetic systems, one peptide coordinating between them.
The ageing connection sharpened in 2021. A Nature Communications study administered MOTS-c to mice starting at 23.5 months, the equivalent of late life for a mouse. Even beginning at that late stage, physical capacity and muscle health improved significantly against untreated age-matched controls.
The same study documented that aerobic exercise naturally induces MOTS-c expression in human skeletal muscle (Reynolds et al., Nat Commun 2021, PMID 33473109). Members experience genuine interest in that finding, the molecule your muscles produce during cardio may be one of the mechanisms by which exercise produces its systemic benefits.
Epithalon: The Telomere Research
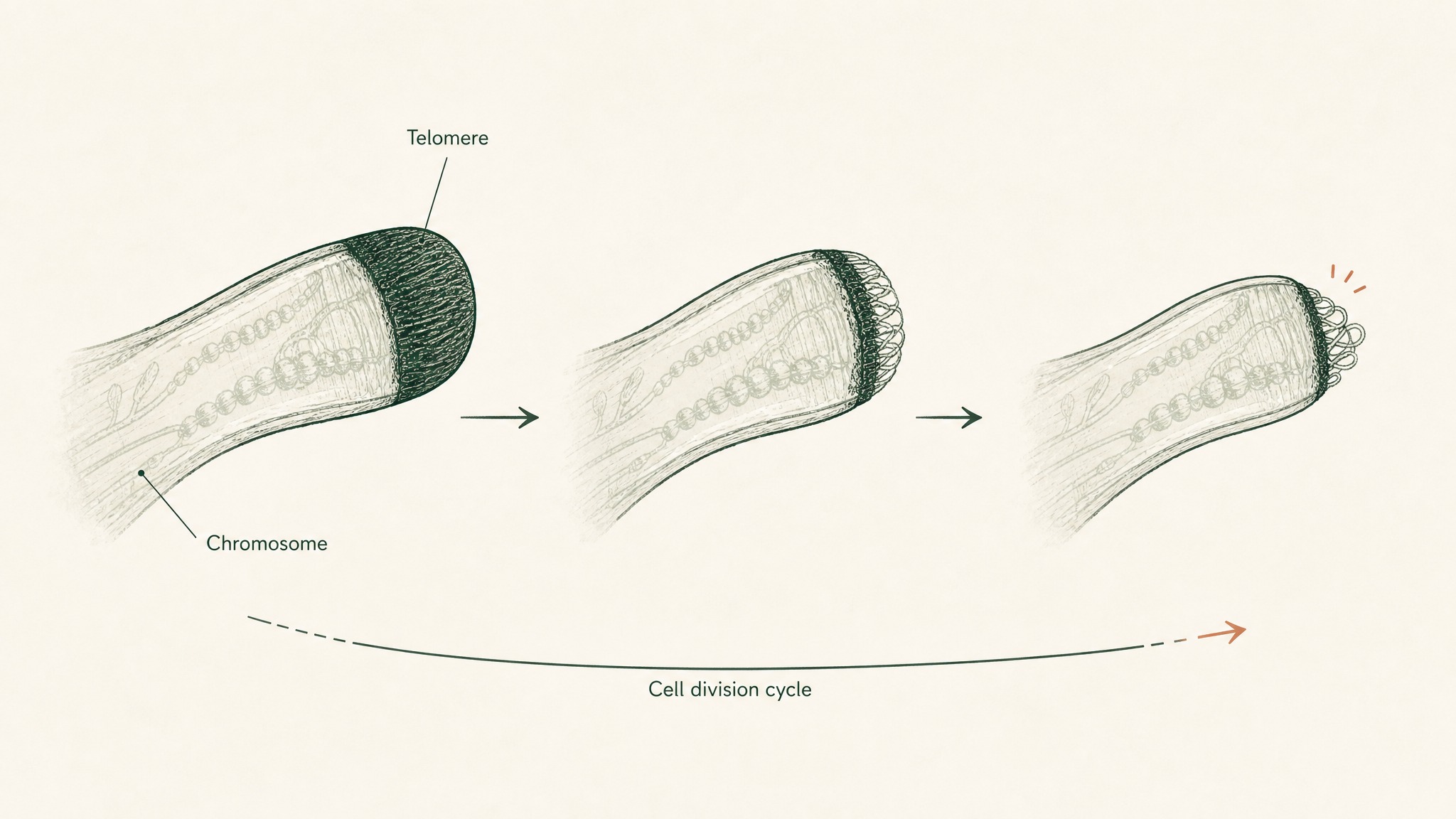
Every time one of your cells divides, the protective caps on the ends of your chromosomes get slightly shorter. Those caps are called telomeres, think of the plastic tip on a shoelace, stopping the genetic information from fraying at the ends. When they get short enough, the cell can no longer divide safely.
It either stops functioning or triggers its own controlled shutdown. Telomere shortening is one of the most studied biological ageing mechanisms in the published record.

Telomeres shorten slightly each time a cell divides, like a shoelace tip wearing down.
Epithalon is a synthetic tetrapeptide, four amino acids: alanine, glutamic acid, aspartic acid, glycine (Ala-Glu-Asp-Gly). It was developed out of Soviet-era pineal gland research in the 1970s and 1980s. Its connection to telomeres was established in a 2003 cell study.
Khavinson, Bondarev and Butyugov introduced Epithalon to human fetal fibroblast cultures that had exhausted their division capacity, cells that had shut down the enzyme telomerase, which is the machinery that normally rebuilds telomere length. The result: Epithalon reactivated telomerase activity, and the cells showed measurable telomere elongation before resuming division (Khavinson, Bondarev & Butyugov, Bull Exp Biol Med 2003, PMID 12937682). A small synthetic peptide had reactivated the cells' own telomere-maintenance machinery.
To be precise about what this finding is and isn't:
- What it is: the most direct cell-level experimental evidence in the published record of a synthetic peptide reactivating telomerase in human cells
- What it isn't: a human clinical trial, and the distance from "telomerase reactivated in a culture dish" to "healthy human lifespan extended" is large and not yet crossed
Users report strong conceptual interest in Epithalon specifically because the telomere mechanism is something you can actually measure, it's tangible in a way many ageing markers aren't. The scientific rationale behind the research interest is real. The clinical translation remains an open question.
What These Three Have in Common
Individually, GHK-Cu, MOTS-c, and Epithalon look like three separate research threads: one about skin and tissue maintenance signals, one about mitochondrial metabolism and antioxidant coordination, one about chromosomal end-cap maintenance. The shared pattern only becomes clear when you step back.
All three are endogenous, your body produces them. All three show measurable decline with age. In each case, restoring or activating them in controlled research settings produced effects in the direction of younger cellular function.
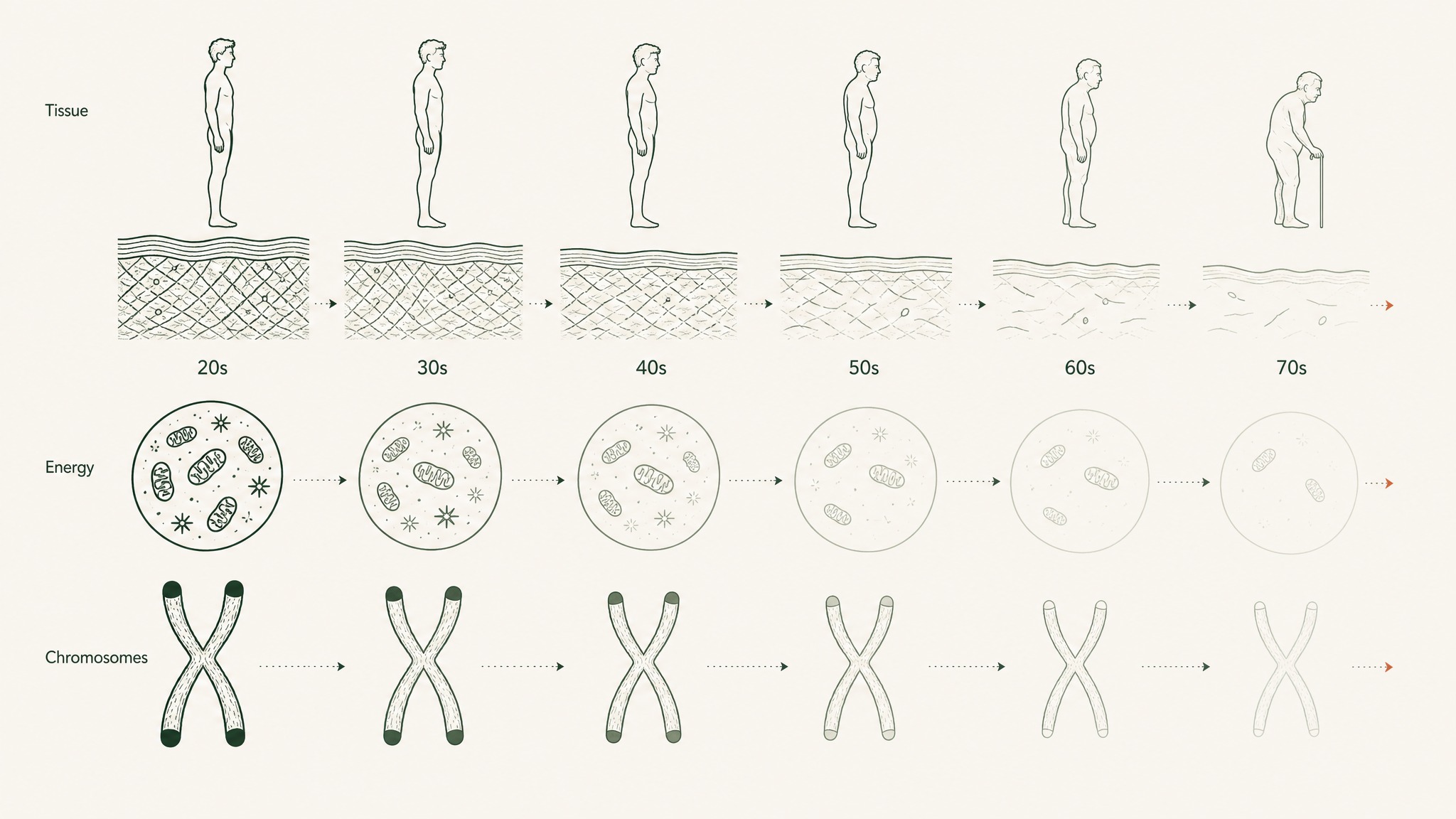
Three separate biological systems all decline together: tissue repair, mitochondrial energy, and chromosome protection.
The convergent picture looks like this:
- GHK-Cu: a circulating tissue maintenance signal that declines in the decades when skin repair, wound closure, and connective tissue maintenance visibly slow down
- MOTS-c: a mitochondrial signal linking energy production, insulin sensitivity, and antioxidant defence, declining in ways that track with age-related metabolic changes
- Epithalon: a tetrapeptide reaching toward the chromosomal level of biological timekeeping, with cell-culture evidence for telomerase reactivation
The research doesn't yet have a unified framework with full clinical backing in humans. What it has is independent mechanistic evidence from three biological systems, tissue maintenance, mitochondrial signalling, chromosomal integrity, all pointing in the same direction.
The Delivery Question
There's a practical detail that matters as much as the science itself: most peptides don't survive oral ingestion intact. Your stomach breaks down proteins and peptide chains before they can reach the bloodstream. This is why injectable delivery has historically been the research standard for compounds like GHK-Cu and MOTS-c.
Sublingual delivery, placing a compound under the tongue, bypasses that problem entirely. The tissue there is highly vascularised and connects directly to your bloodstream. Intact molecules absorb without first passing through the stomach or liver's metabolic processing.
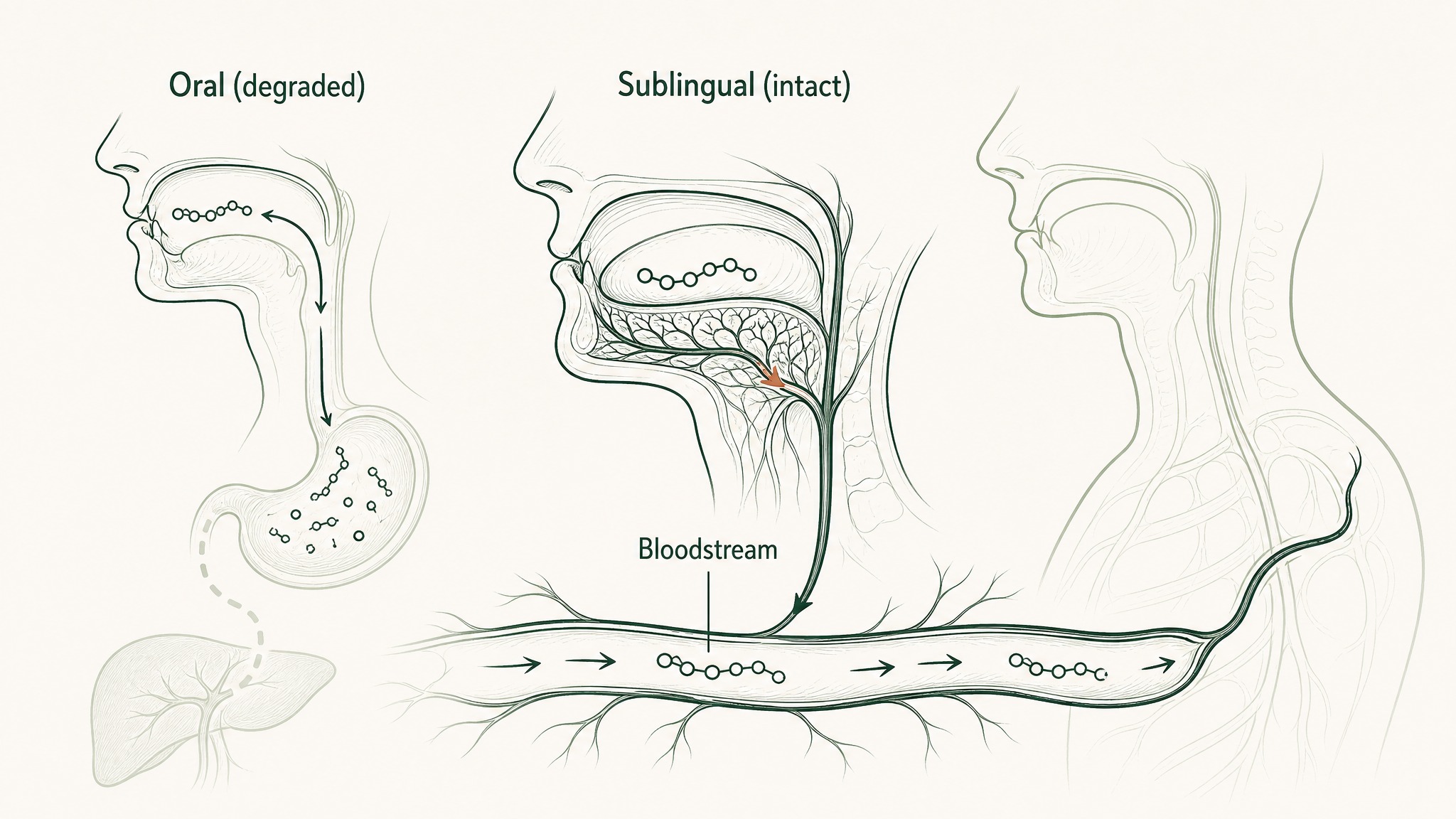
Why peptides placed under the tongue reach your blood intact, while swallowing breaks them down first.
For small peptides like GHK-Cu, sublingual delivery makes absorption possible in a way oral ingestion simply doesn't.
VERO's VERISORB system is built on this principle. The VERISORB delivery guide covers the bioavailability science behind sublingual peptide delivery in full, including what "bypassing first-pass metabolism" actually means for how these molecules reach your system.
Frequently Asked Questions
What is GHK-Cu and how does it support cellular maintenance?
GHK-Cu is a tripeptide consisting of glycine, histidine, and lysine bound to a copper ion, produced naturally by your liver, skin, and plasma. Circulating levels fall from roughly 200 ng/mL at age 20 to around 80 ng/mL by age 60, a measured decline that correlates with slower tissue repair. Research suggests GHK-Cu influences gene expression across tissue remodelling, antioxidant defence, and anti-inflammatory pathways, with a 2014 genomic analysis finding it changed expression by at least 50% in approximately a third of human genes studied.
How does MOTS-c affect metabolism and energy regulation?
MOTS-c is a 16-amino-acid peptide encoded in mitochondrial DNA and released from skeletal muscle into the bloodstream. Research suggests it activates AMPK, the cellular master energy sensor, which improves glucose uptake, fat utilisation, and insulin sensitivity. Under metabolic stress, MOTS-c also translocates to the cell nucleus and activates NRF2, the master switch for antioxidant gene expression, meaning a single peptide coordinates both energy regulation and cellular defence through the same upstream pathway.
What does the Epithalon research actually demonstrate?
A 2003 cell study introduced Epithalon to human fibroblast cultures that had stopped dividing and found it reactivated telomerase activity, producing measurable telomere elongation. This is the most direct published evidence of a synthetic peptide reactivating telomere-maintenance machinery in human cells. The research is cell-culture only: no human interventional trial data is currently published, and the distance from a culture dish finding to clinical application remains an open scientific question.
Does aerobic exercise have a documented relationship with MOTS-c levels?
Research suggests aerobic exercise naturally induces MOTS-c expression in human skeletal muscle, a finding documented in a 2021 Nature Communications study. The same study showed MOTS-c treatment improved physical performance in aged mice even when begun late in life, against untreated age-matched controls. The finding implies that cardio-induced MOTS-c release may be one mechanism by which exercise produces systemic benefits beyond the muscle tissue itself.
Why does delivery method matter for these research peptides?
Most peptides break down in the stomach before reaching the bloodstream, which limits the relevance of oral ingestion for research purposes. Injectable delivery has historically been the standard for compounds like GHK-Cu and MOTS-c because it bypasses digestive breakdown entirely. Sublingual delivery works on the same principle: the tissue under the tongue is highly vascularised and connects directly to the bloodstream, allowing intact molecules to absorb without passing through the stomach or liver's first-pass metabolic processing.
Who is the research on age-supportive peptides most relevant for?
The published research focuses on age-related declines in endogenous signalling molecules, making it most relevant for adults in their thirties and older when measurable reductions in GHK-Cu, MOTS-c, and similar compounds typically begin. Users report interest in these compounds as part of a broader approach to cellular health rather than as standalone interventions. These are research peptides, not approved medical treatments, and they are not substitutes for clinical care of any diagnosed condition.
How do GHK-Cu, MOTS-c, and Epithalon differ from each other?
The three peptides operate across distinct biological systems: GHK-Cu works primarily on tissue remodelling and antioxidant gene signalling, MOTS-c coordinates mitochondrial energy output with nuclear antioxidant defence, and Epithalon has published cell-culture evidence for telomerase reactivation at the chromosomal level. Research suggests all three are endogenous, all three decline measurably with age, and all three show effects in the direction of younger cellular function in controlled settings. The convergence across three independent biological systems is what distinguishes this group from single-mechanism compounds.
Key Takeaways
- GHK-Cu plasma levels fall roughly 60% between age 20 and age 60, from ~200 ng/mL to ~80 ng/mL, a documented, measurable decline that correlates with reduced tissue repair capacity (PMC6073405)
- GHK-Cu changes gene expression by at least 50% in approximately a third of human genes, influencing tissue remodelling, antioxidant defence, and anti-inflammatory signalling pathways (PMC4180391)
- MOTS-c is a 16-amino-acid peptide encoded in mitochondrial DNA; its 2015 discovery paper showed it activates AMPK in skeletal muscle, reducing age-related and diet-induced insulin resistance in mouse models (PMID 25738459)
- Under metabolic stress, MOTS-c travels to the cell nucleus and activates antioxidant genes via NRF2, a bidirectional communication between two separate genetic systems (PMID 29983246)
- In aged mice, MOTS-c treatment initiated in late life improved physical performance; exercise data confirms aerobic training naturally induces MOTS-c expression in human skeletal muscle (PMID 33473109)
- Epithalon reactivated telomerase and produced measurable telomere elongation in human fibroblast cell cultures, the most direct cell-level evidence of a synthetic peptide reactivating telomere-maintenance machinery in the published record (PMID 12937682). Cell culture findings only; no human interventional trial data is currently published.
- All three peptides are endogenous, measurably decline with age, and show effects in the direction of younger cellular function in controlled research settings
Ready to explore protocols built around compounds with the strongest delivery science behind them? View protocols →
References
Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMC6073405
Pickart L, Vasquez-Soltero JM, Margolina A. GHK and DNA: Resetting the Human Genome to Health. BioMed Res Int. 2014. PMC4180391
Pickart L, Thaler MM. Tripeptide in human serum which prolongs survival of normal liver cells and stimulates growth in neoplastic liver. Nat New Biol. 1973;243(124):85-7. PMID 4349963
Lee C, Zeng J, Drew BG, et al. The mitochondrial-derived peptide MOTS-c promotes metabolic homeostasis and reduces obesity and insulin resistance. Cell Metab. 2015;21(3):443-54. PMID 25738459
Kim KH, Son JM, Benayoun BA, Lee C. The Mitochondrial-Encoded Peptide MOTS-c Translocates to the Nucleus to Regulate Nuclear Gene Expression in Response to Metabolic Stress. Cell Metab. 2018;28(4):516-524.e7. PMID 29983246
Reynolds JC, Lai RW, Woodhead JST, et al. MOTS-c is an exercise-induced mitochondrial-encoded regulator of age-dependent physical decline and muscle homeostasis. Nat Commun. 2021;12(1):470. PMID 33473109
Khavinson VKh, Bondarev IE, Butyugov AA. Epithalon peptide induces telomerase activity and telomere elongation in human somatic cells. Bull Exp Biol Med. 2003;135(6):590-2. PMID 12937682
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.