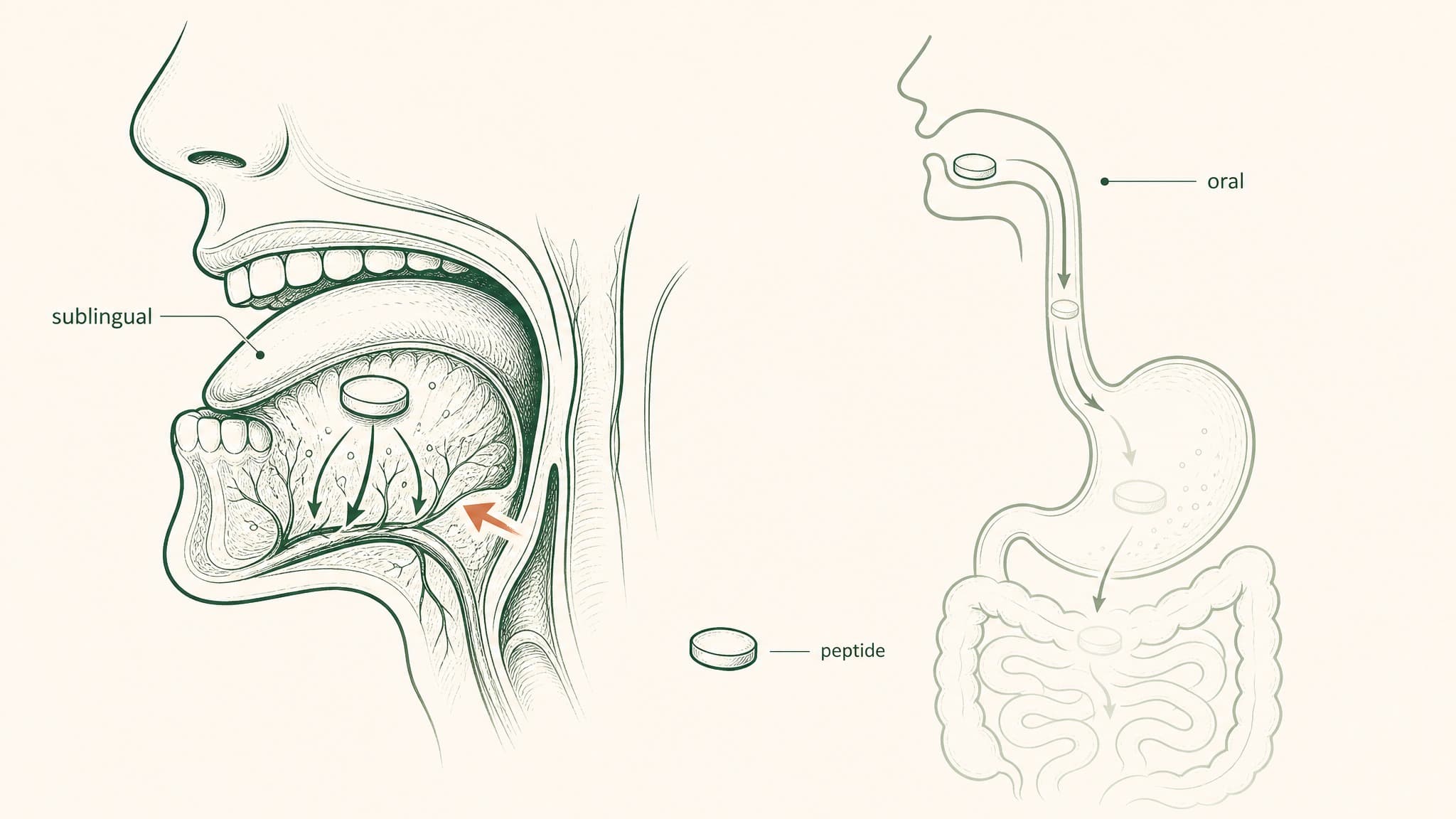
Swallowing a peptide and absorbing one are two different things. Here's what each delivery route does to a research compound before it reaches your blood.
If you're comparing sublingual and oral peptide delivery, here's the short answer: one route gets the compound into your bloodstream, and one mostly doesn't. Oral peptides face five sequential barriers in your gut that dismantle most of the compound before your blood ever sees it. Documented bioavailability sits below 2 percent for most unmodified peptides, a consistent finding across compound classes.
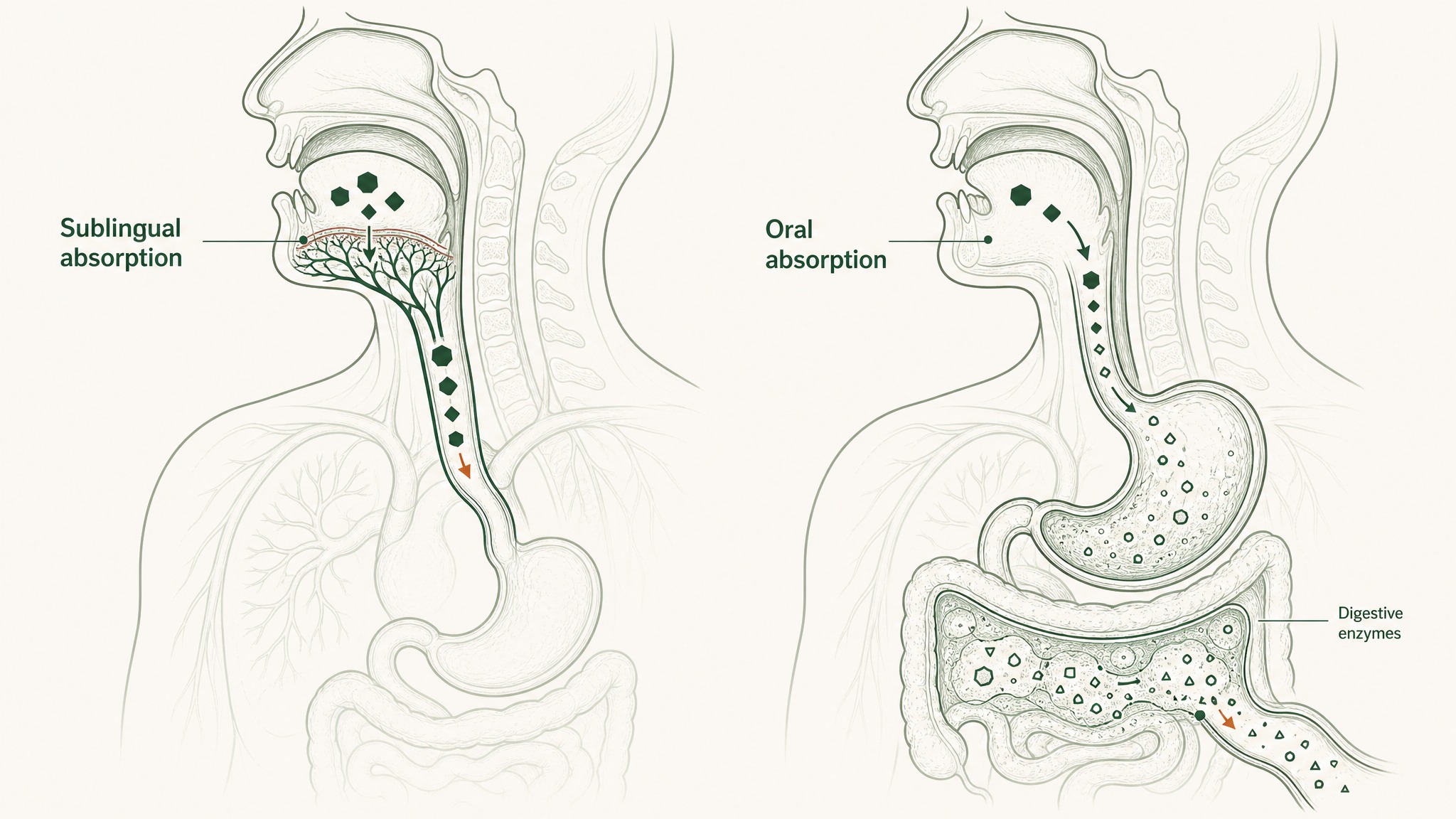
Sublingual delivery bypasses those barriers by using the tissue under your tongue as a direct entry point to systemic circulation. The route matters as much as the compound. This content is published for research purposes only.
Understanding why that happens, and why sublingual changes the equation, is what makes it possible to design a research protocol with any real precision.
What Swallowing a Peptide Actually Does to It
Think of your digestive system as five security checkpoints built specifically to dismantle anything that looks like food protein. Peptides are chains of amino acids, the same structure as food protein. Your gut doesn't distinguish between the two.
Here's what each checkpoint does to a research peptide:
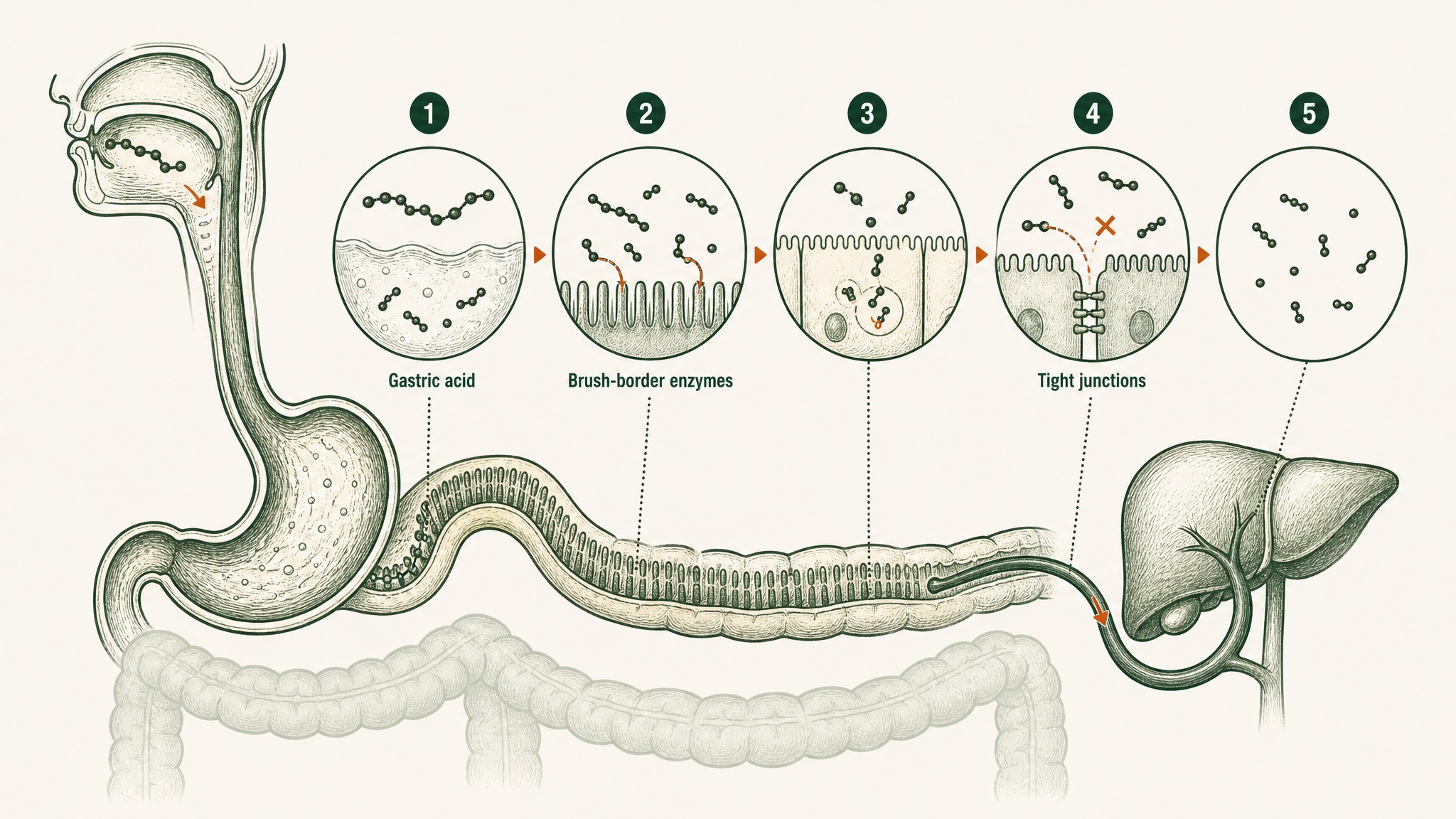
How your digestive system breaks down oral peptides into fragments before they reach your bloodstream.
- Gastric acid (pH 1.5–3.5): Creates an environment roughly as acidic as battery acid, which begins unfolding peptide structure and activates pepsin, the enzyme whose sole job is cutting the bonds that hold peptide chains together
- Brush-border peptidases: A dense enzyme layer coating the small intestine wall surface, continuing the dismantling of anything that survived the stomach
- Intestinal epithelium: A single continuous cell layer that functions as both a physical barrier and a biochemical checkpoint, containing its own intracellular enzymes that process anything attempting to cross it
- Tight junctions: The gaps between intestinal cells, sealed by protein structures that selectively allow small molecules through while blocking most of the larger compounds that make up typical research peptides
- First-pass hepatic metabolism: Everything absorbed from your gut routes to your liver before your general circulation sees it. The liver takes an additional enzymatic cut from whatever fraction survived the earlier stages.
The result of that sequence is well-established. Unmodified oral peptides typically achieve bioavailability (how much of what you swallow actually makes it to your blood intact) of less than 1 to 2 percent (Renukuntla et al. 2013, Int J Pharm, PMC3680128). Some peptide classes sit even lower.
More recent analysis places certain compound classes below 0.1 percent (Baral & Choi 2025, Pharmaceutics, PMC12030352). Out of every 100 milligrams in a capsule, 98 milligrams or more never reach your blood.
One gut mechanism does absorb intact peptides: a transporter protein called PepT1, which shuttles short two- or three-amino-acid fragments across the intestinal wall. But it exists to absorb the byproducts of food digestion, not research compounds. Most peptides are far too long for that transporter: BPC-157 is 15 amino acids, well outside the window PepT1 handles (Freeman 2015, World J Gastrointest Pharmacol Ther, PMC4419090).
Under the Tongue: A Different Path to Your Bloodstream
The sublingual route doesn't try to survive the gut. It bypasses the gut entirely.
The tissue under your tongue is one of the most permeable surfaces in your body. The sublingual mucosa (the thin membrane lining that space) is only around 100 to 200 micrometres thick, roughly the width of two human hairs. It sits directly over a dense network of blood vessels with access to systemic circulation, meaning the blood that eventually reaches your muscles, brain, and organs (Bahraminejad & Almoazen 2025, Pharmaceutics, PMC12389210).
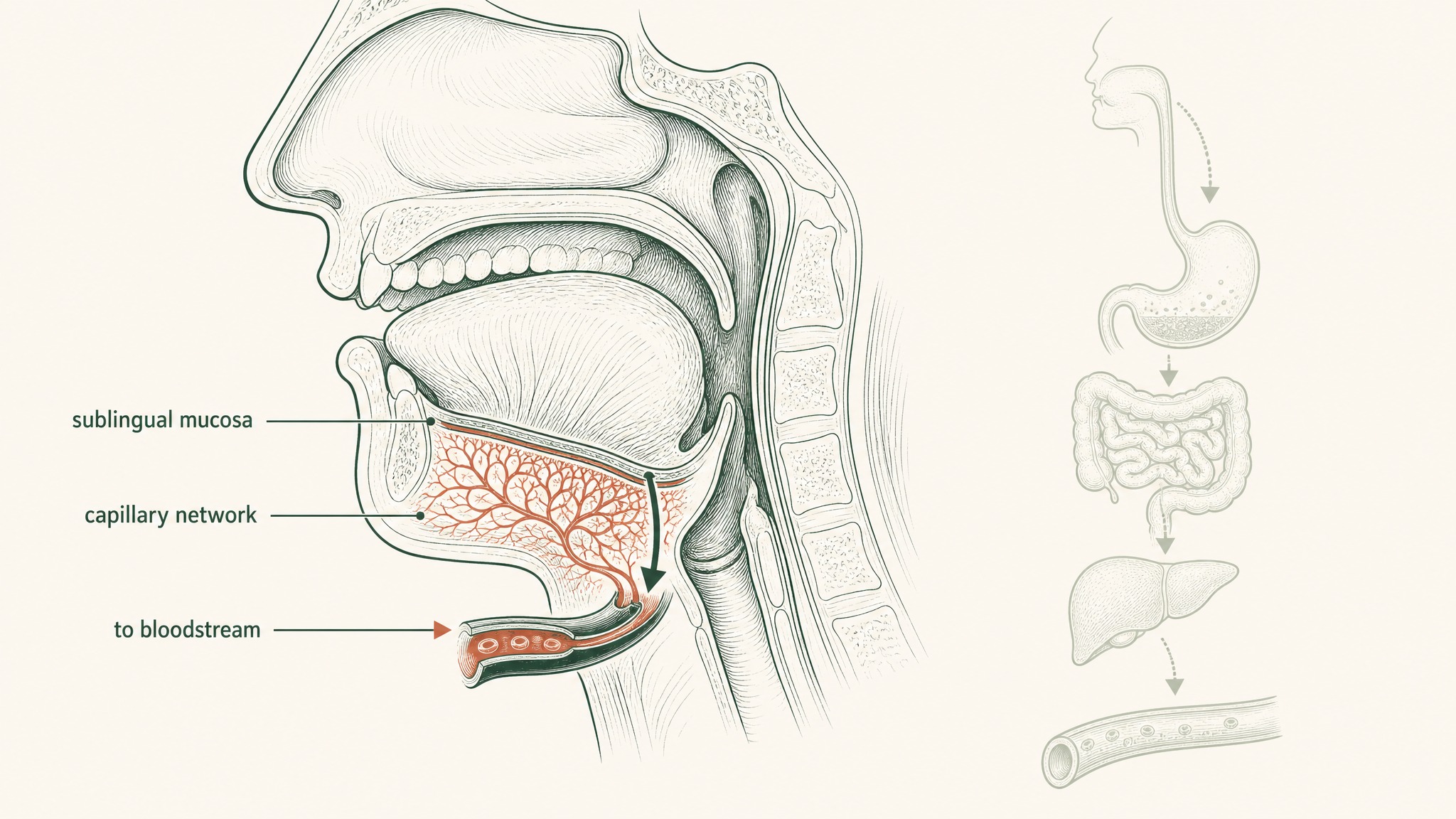
Sublingual tissue sits directly over blood vessels, bypassing the stomach and liver entirely.
A compound absorbed here doesn't go to the liver first. It goes to your blood.
The enzymatic environment is also different. There's no pepsin here and no gastric acid. Saliva contains some proteases (enzymes that break down proteins), but the profile is substantially less aggressive than your gut's compounding destruction sequence (Senel et al. 2001, Curr Pharm Biotechnol, PMID 11480421).
Think of the oral route like shipping a package through a five-stage inspection facility where each stage discards most of the contents. The sublingual route is a private entrance that skips all five checkpoints and delivers directly.
The First-Pass Bypass: What That Actually Means
Most people know the gut is harsh to peptides. Fewer realise the liver gets a second crack at whatever survives.
Everything absorbed from your gut enters the portal circulation, a direct pipeline from the intestines to your liver, before the rest of your body sees any of it. Your liver identifies compounds arriving from the gut and runs them through what researchers call first-pass hepatic metabolism. For most research peptides, that stage eliminates the majority of whatever fraction survived the intestinal gauntlet.
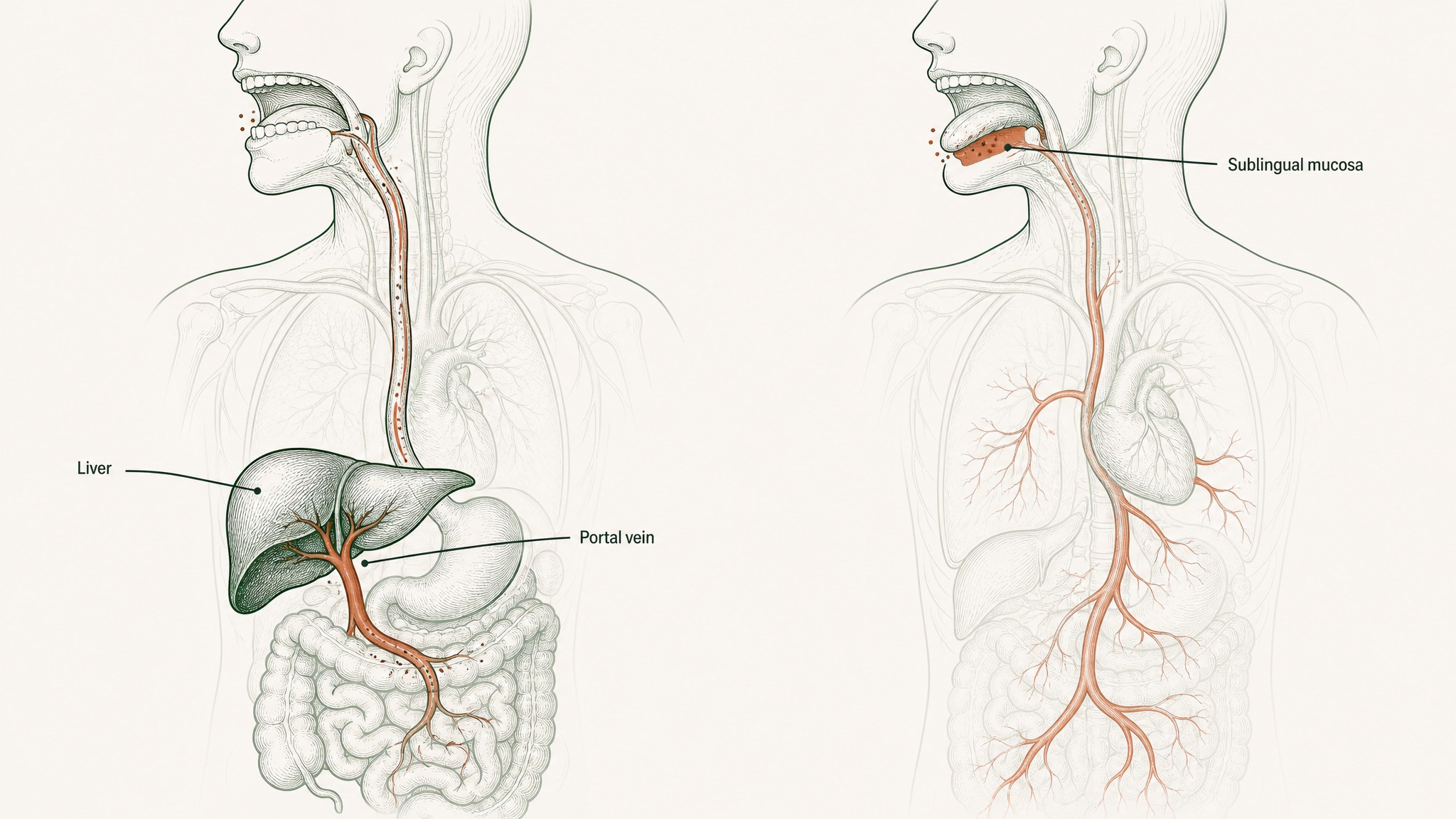
Oral peptides route through the liver first; sublingual peptides enter the bloodstream directly.
Sublingual absorption skips this entirely. Compounds absorbed through the sublingual mucosa enter systemic circulation directly, without first routing through the liver (Bahraminejad & Almoazen 2025, Pharmaceutics, PMC12389210). Your liver still processes the compound as it circulates over time. But it doesn't get the first cut, the one that eliminates the most.
That's the structural difference between the two routes. The oral route gives the liver the first opportunity to eliminate the compound; the sublingual route doesn't. It's a difference in which biological elimination processes even get access to the compound, not just a marginal difference in how much survives.
What the Research Shows About Sublingual Delivery
Quantitative human bioavailability data on research peptides via sublingual administration is limited. Human trials on investigational compounds take years and significant funding.
The mechanism, though, has been demonstrated clearly enough that pharmaceutical researchers have built delivery systems around it.
Sublingual peptides enter the bloodstream directly; oral peptides must survive stomach acid and digestive enzymes first.
Research suggests that novel peptide formulations applied sublingually can facilitate absorption of proteins ranging from 22 to 150 kilodaltons, including recombinant growth hormone, serum albumin, and immunoglobulin G, with systemic delivery profiles that researchers found comparable to subcutaneous administration (Wu et al. 2024, J Control Release, PMID 38423473). These are molecules substantially larger than most research peptides. The route's ability to move large proteins at all is the relevant finding.
Compare that to the documented ceiling for oral delivery. Rybelsus (the oral form of semaglutide) uses a proprietary absorption enhancer called SNAC to get semaglutide across the stomach wall before the small intestine's enzymes can reach it. Under strict administration conditions (30 minutes before any food, no more than 120 millilitres of water), that engineered system achieves absolute bioavailability of 0.8 percent (Overgaard et al. 2021, Clin Pharmacokinet, PMID 33969456).
Semaglutide works at that fraction because the compound is potent enough that even 0.8 percent produces a measurable effect. Most research peptides don't work the same way. The gap between sublingual and oral isn't marginal: it's the difference between a route that bypasses your biology's elimination sequence and one that tries to fight through it.
Which Compounds Absorb Best Through Sublingual Mucosa
Not every peptide absorbs equally well through the sublingual route. Several characteristics determine how effectively a compound crosses the mucosal tissue:
- Molecular weight: Smaller peptides cross the mucosal epithelium more readily than large proteins. Under 3,000 daltons is the general research threshold for meaningful passive permeation through the membrane
- Lipophilicity (fat-solubility): The mucosal membrane has a lipid bilayer component, so compounds with some fat-solubility move through it more readily than highly water-soluble molecules
- Contact time: The compound needs sustained contact with the mucosal surface to absorb. Swallowing early or rinsing the mouth defeats the route before uptake completes
- Formulation: Raw crystalline peptide doesn't adhere to mucosal tissue as effectively as a purpose-designed sublingual formulation built to resist salivary washout, maintain contact, and support permeation
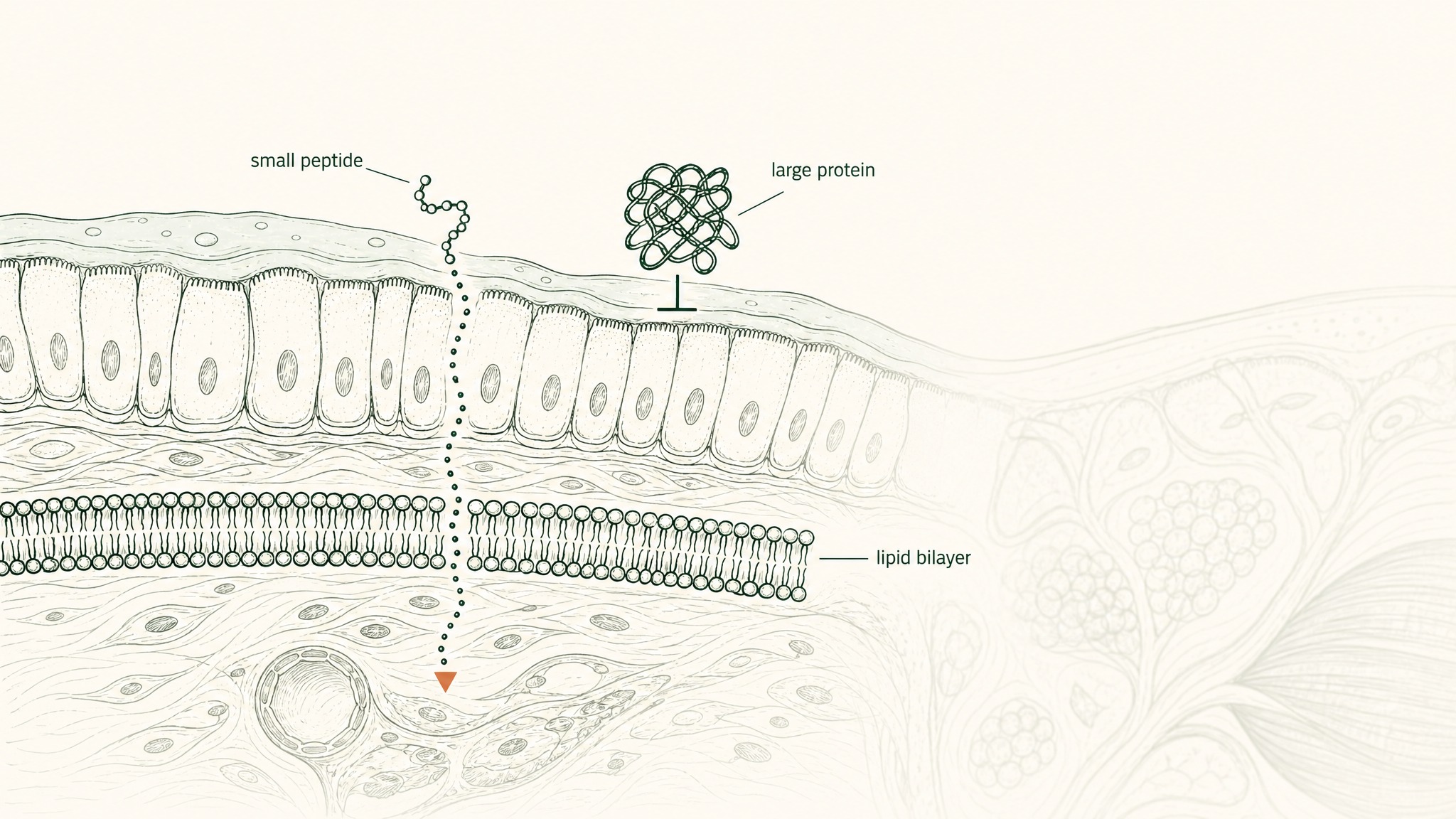
Small peptides pass through sublingual tissue more easily than large proteins because of the lipid barrier.
Members experience the most consistent results when all four factors align: right compound, right formulation, correct technique, and adequate hold time. The route advantage only fully materialises when the product is actually built for the route.
How to Get the Most from Sublingual Delivery
The technique is straightforward, but the steps most people skip are the ones that matter most:
- Start with a clean mouth: Rinse with water but don't eat before administration. Food residue dilutes contact and competes with the compound for mucosal access.
- Hold position: Place the compound under the tongue or against the inner cheek, and hold for at least 60 to 90 seconds without swallowing
- No rinsing immediately after: Allow 5 to 10 minutes before eating or drinking so any residual compound finishes absorbing rather than washing away with saliva
- Consistent timing: Same time of day, same pre-dose conditions. Mucosal hydration and saliva volume both affect absorption rates, so consistent conditions produce more consistent outcomes.
Users report that anchoring the hold time to a fixed morning routine rather than fitting it around meals is the most reliable way to stay consistent. The administration takes under two minutes. The payoff is bypassing a destruction sequence that eliminates 98 percent or more of compounds taken orally.
Why Route Choice Is a Protocol Decision
The peptide industry has a marketing problem: nearly all the attention goes to compound names, and almost none goes to delivery route. You see a product listing GHK-Cu or BPC-157, you read what the research says about it, and you buy it.
But whether those research findings are even relevant to what you're taking depends entirely on whether the compound reaches your bloodstream at all.
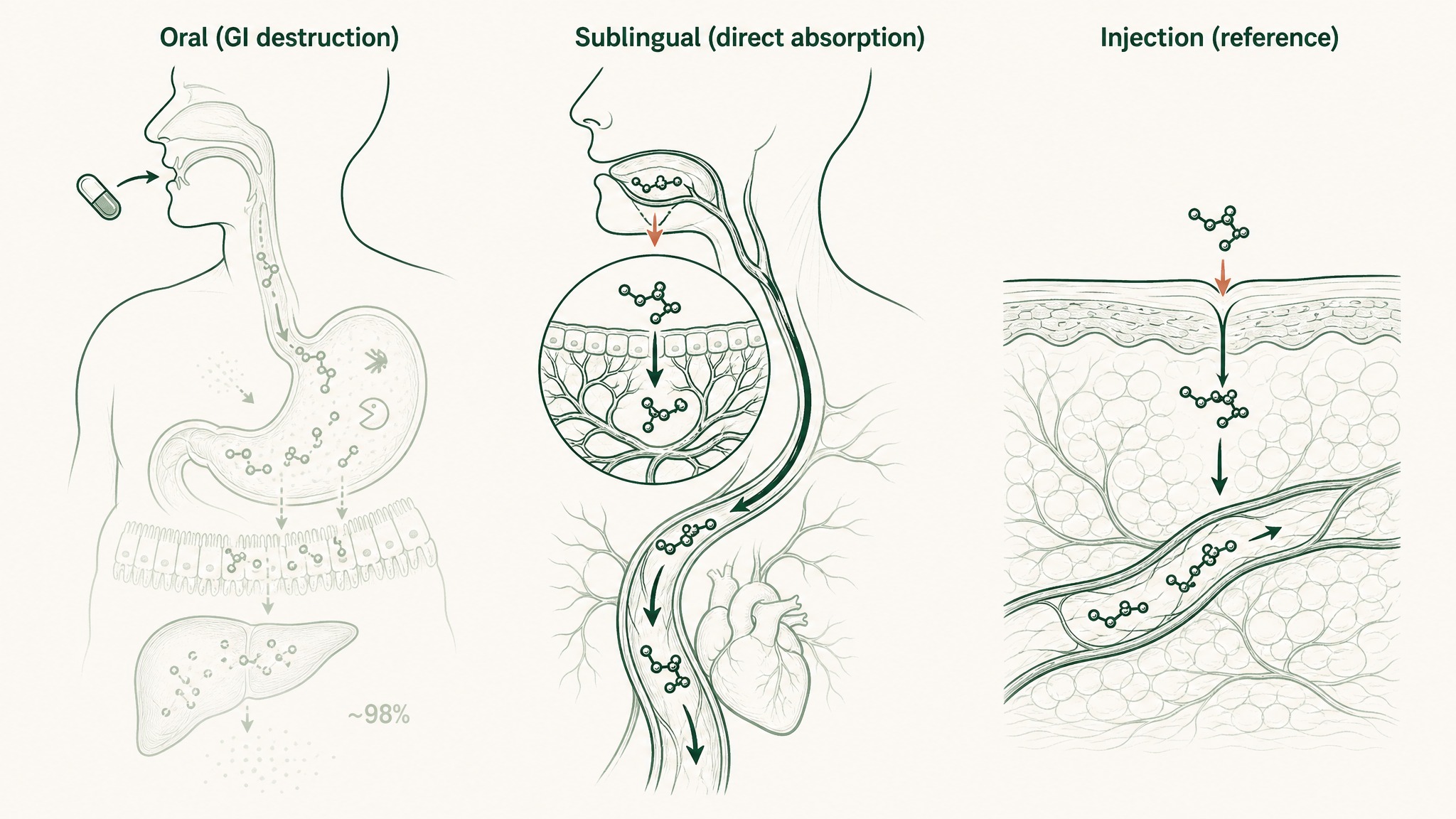
Why sublingual peptides reach your bloodstream while oral capsules are mostly destroyed before absorption.
- Oral capsules: fighting through five sequential elimination stages with a documented sub-2% exit rate
- Sublingual formulations: bypassing the GI destruction sequence and the first-pass liver cut by using the most permeable mucosal surface in your body
- Subcutaneous injection: the reference standard, bypassing the gut entirely with maximum controlled delivery
A compound with solid supporting research doesn't deliver those mechanisms if it's destroyed before it reaches circulation. Choosing the delivery route carries the same weight as choosing the compound. It's not a secondary detail.
VERO's VERISORB sublingual delivery system was built around exactly this problem. It's a formulation architecture designed to maintain mucosal contact time, support permeation through the sublingual epithelium, and get research compounds into systemic circulation rather than through the liver's first pass. The RESTORE Protocol uses VERISORB delivery because the absorption science makes the route choice the obvious one.
Frequently Asked Questions
How much of an oral peptide actually reaches the bloodstream?
Research suggests that unmodified oral peptides typically achieve bioavailability of less than 1 to 2 percent, with some compound classes sitting below 0.1 percent. Out of every 100 milligrams swallowed, 98 milligrams or more are broken down by gastric acid, intestinal enzymes, and first-pass liver metabolism before entering general circulation. This ceiling applies even when administration conditions are controlled, as the gut's dismantling sequence operates on structure rather than intent.
How long should you hold a sublingual peptide under your tongue?
Research and user reports suggest holding for at least 60 to 90 seconds to allow meaningful mucosal contact and absorption through the sublingual epithelium. Swallowing too early terminates the absorption window before the compound can cross into the blood vessels under the tongue. Waiting 5 to 10 minutes before eating or drinking after administration allows any residual compound to finish absorbing rather than washing away with saliva or food.
Why does sublingual delivery bypass first-pass liver metabolism?
Compounds absorbed through the sublingual mucosa enter systemic circulation directly via the dense vasculature under the tongue, rather than routing through the portal circulation from the gut to the liver. First-pass hepatic metabolism is triggered specifically by intestinal absorption: compounds that never enter the gut never trigger that elimination process. The liver still processes the compound as it circulates over time, but it does not receive the initial concentrated bolus that typically accounts for the largest fraction of elimination.
How does sublingual peptide delivery compare to subcutaneous injection?
Subcutaneous injection is the reference standard for peptide delivery and bypasses the gut entirely, with controlled and predictable absorption into systemic circulation. Sublingual delivery also bypasses the gut and first-pass liver metabolism, though absorption rates can vary depending on formulation quality, compound size, and hold technique. Research on novel sublingual formulations suggests systemic delivery profiles that researchers found comparable to subcutaneous administration for certain large proteins, though compound-specific human bioavailability data for the sublingual route remains limited.
Which peptides absorb most effectively via the sublingual route?
Research suggests that smaller peptides, generally under 3,000 daltons, cross the sublingual mucosa more readily through passive permeation of the lipid bilayer membrane. Compounds with some fat-solubility also move through the mucosal barrier more effectively than highly water-soluble molecules. Purpose-designed sublingual formulations that resist salivary washout and maintain sustained mucosal contact improve absorption outcomes compared to unformulated raw powder applied directly under the tongue.
Can you eat or drink immediately after taking a sublingual peptide?
Users report that eating or drinking immediately after administration washes residual compound off the mucosal surface before absorption completes. Waiting 5 to 10 minutes after the hold period allows any remaining compound to finish crossing the sublingual epithelium rather than being diluted and swallowed. The same logic applies to rinsing: even water introduced too soon can reduce the effective dose by clearing the absorption site prematurely.
Who is sublingual peptide delivery not suitable for?
Sublingual delivery requires correct technique and consistent hold time to realise its absorption advantage, so users who cannot maintain the hold position reliably may see variable results. Individuals with active oral mucosal conditions, mouth sores, or chronic dry mouth may experience altered absorption due to compromised tissue integrity or reduced mucosal hydration. As with any research administration route, sublingual delivery is not appropriate for self-treatment outside a supervised research context, and a qualified healthcare provider should be consulted before beginning any protocol.
Key Takeaways
- Oral peptides face five sequential barriers, gastric acid, pepsin, brush-border peptidases, the intestinal epithelium, and first-pass liver metabolism, that reduce most compounds to under 2% bioavailability before they reach your blood
- Sublingual delivery bypasses the entire GI destruction sequence and the first-pass liver cut by using the thin mucosal tissue under your tongue as a direct entry point to systemic circulation
- The sublingual mucosa is only 100–200 micrometres thick and sits over dense vasculature. It's one of the most permeable absorption surfaces in the body.
- Research on protein delivery via sublingual administration confirms meaningful systemic delivery even for large proteins (22–150 kDa), a ceiling oral delivery cannot approach without engineered absorption technology
- The enzymatic environment under the tongue lacks pepsin and gastric acid, making it substantially less aggressive than the compounding destruction sequence the gut and liver apply to orally administered compounds
- Correct sublingual technique (adequate hold time, timing relative to food, and a purpose-designed formulation) determines whether the route advantage is actually realised in practice
Ready to put this into a structured research protocol? Explore the VERO RESTORE Protocol, formulated for sublingual delivery and built around the absorption science. Start the RESTORE Protocol →
VERO content is published for educational purposes only and is not intended to diagnose, treat, cure or prevent any disease. Consult a qualified healthcare provider before beginning any research protocol.
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.