Most peptide pills are destroyed in your gut before they work. Here's what the research shows, and what makes a legitimate peptide product different.
Here's the direct answer most peptide brands won't give you: the majority of oral peptide pills on the market don't deliver working peptides into your bloodstream. VERO's own peptide pills sidestep the problem by dissolving under the tongue instead. The exception is peptides built around an absorption-engineered delivery format, and telling that apart from the rest is the point of this piece. This isn't a fringe critique: unmodified oral peptides typically achieve bioavailability (how much of what you swallow actually makes it into your blood) of less than 1 to 2 percent (Renukuntla et al. 2013, Int J Pharm, PMC3680128). This content is published for research purposes only.
Not because the peptides are necessarily fake. Because your gut is a precision dismantling machine, and peptides look identical to food protein to every part of it.
"Scam" deserves more precision than a blanket yes or no. Some products misrepresent their ingredients entirely; others contain exactly what the label says but use a format that can't get the compound into your blood; and a small category uses delivery engineering that genuinely bypasses the problem. Knowing which is which is the whole point of this piece.
Key Takeaways
- Most oral peptide pills don't effectively deliver peptides into your bloodstream. Research documents bioavailability below 1 to 2 percent for unmodified oral compounds, the gut's multi-stage destruction sequence eliminates them before they can absorb (Renukuntla et al. 2013, PMC3680128).
- The best oral peptide bioavailability pharmaceutical science has produced is 0.8 percent, for a single purpose-engineered drug under strict controlled conditions (Overgaard et al. 2021, PMID 33969456). Standard supplement capsules are well below this ceiling.
- Most peptide supplement products aren't fraudulent in terms of ingredients. The problem is they use a delivery format that can't reliably put the compound into your bloodstream, and they rarely disclose this.
- Subcutaneous injection and properly formulated sublingual delivery are the two routes that genuinely bypass the gut's destruction sequence.
- Red flags: no delivery mechanism explanation, no bioavailability discussion, outcomes borrowed from injection research, prices inconsistent with synthesis costs, no certificate of analysis.
- Legitimate peptide research brands use research-oriented framing, acknowledge where evidence is preliminary, and are transparent about how their delivery technology actually works.
Want to see what bypass-the-gut delivery looks like in practice? Explore the RESTORE Protocol →
Why Oral Pills Can't Deliver Peptides Effectively
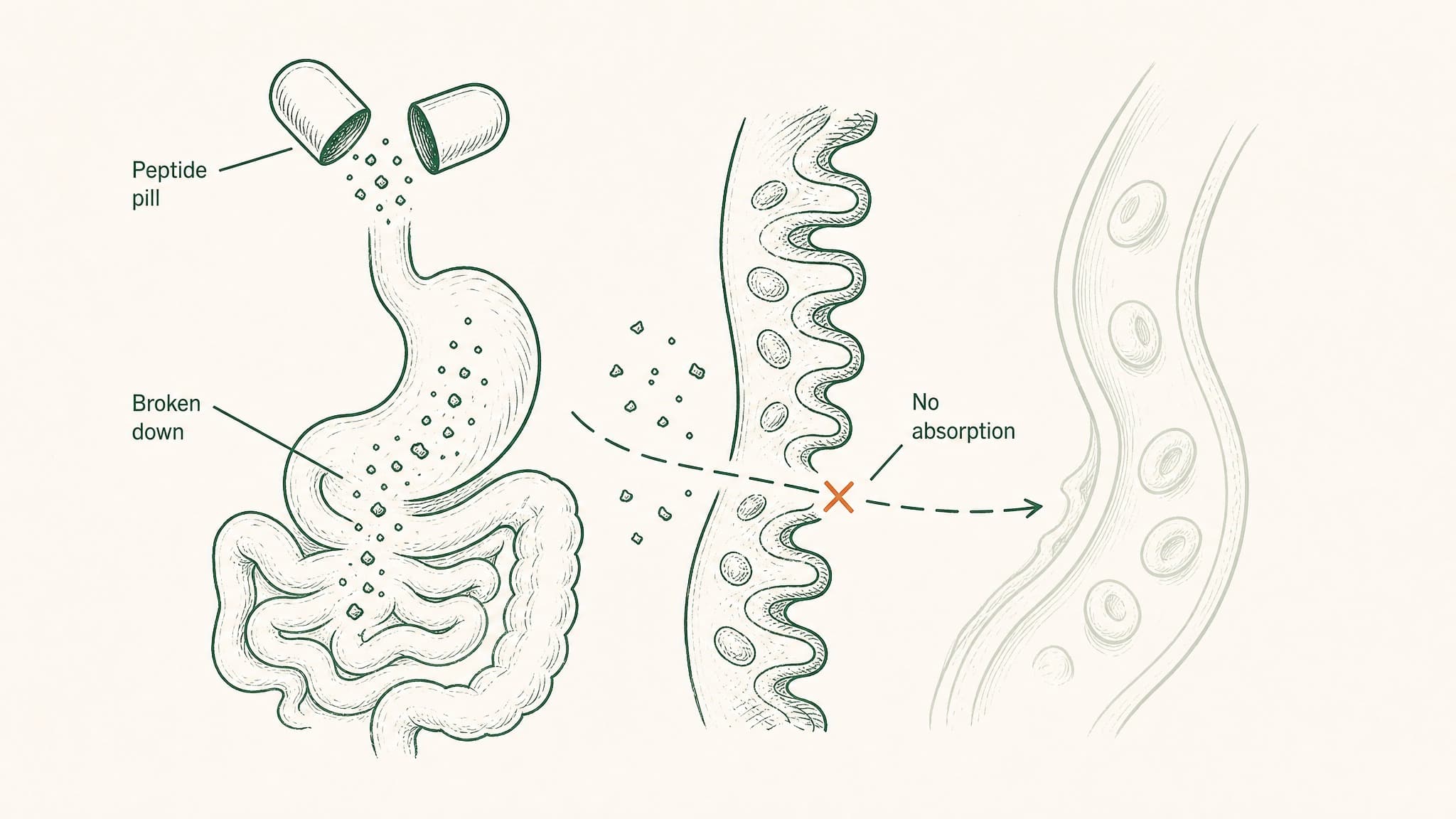
Your digestive system functions as a multi-stage checkpoint built to dismantle any protein structure that enters it. It wasn't built to block peptide supplements specifically, it was built to process food. Peptides are chains of amino acids, just like food protein, and the checkpoint runs both through exactly the same sequence.
Here's the destruction sequence:
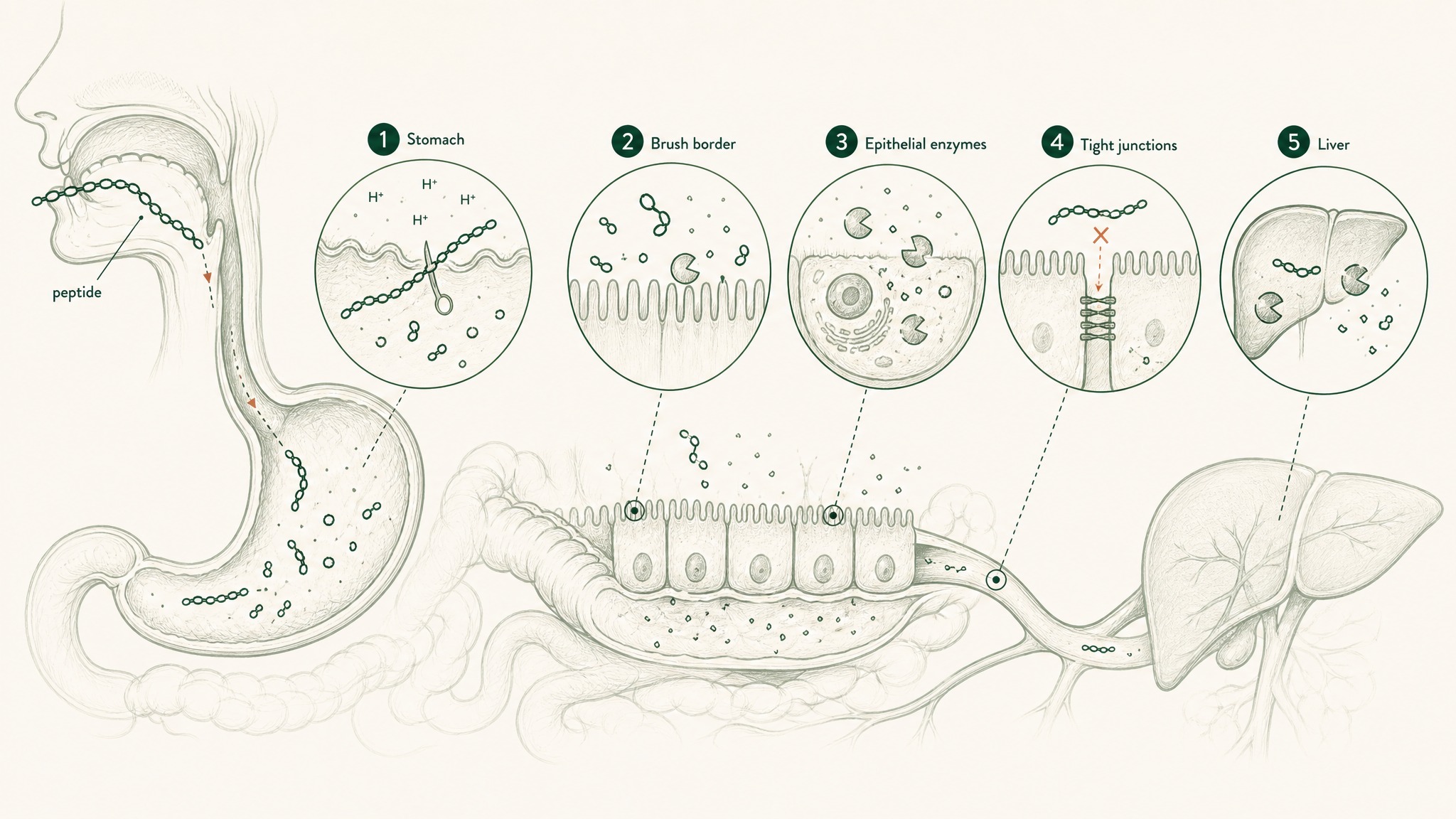
How your digestive system destroys peptide pills before they reach your bloodstream.
- Stomach (pH 1.5 to 3.5, roughly battery acid territory): produces pepsin, an enzyme whose entire function is cutting the chemical bonds that hold peptide chains together. The acidic environment alone begins to unfold and disrupt molecular structure.
- Small intestine brush-border: the intestinal lining is coated with enzymes called peptidases that continue dismantling anything that survived the stomach.
- Epithelial barrier: a continuous cell layer functioning as both a physical wall and a biochemical checkpoint, including enzymes inside the cells themselves that process anything attempting to cross.
- Tight junctions: protein structures sealing the gaps between intestinal cells. They block most larger molecules (including most research peptides) from slipping through.
- Hepatic first pass: everything absorbed from your gut enters the portal circulation, routed to your liver before it reaches the rest of your body. Hepatic proteases take a final cut.
Each stage works on whatever the previous stage left behind. Oral peptide delivery faces enzymatic degradation, poor cellular membrane permeability, and hepatic first-pass metabolism as sequential obstacles (Verma et al. 2021, Drug Dev Res, PMID 33988872). Multiply those reductions together and you arrive at sub-2-percent bioavailability, that's not a pessimistic estimate; it's the documented outcome.
There is one active transport mechanism in the gut that accepts intact peptides: a transporter protein called PepT1. The problem is PepT1 only transports di-peptides and tri-peptides, chains of exactly two or three amino acids (Freeman 2015, PMC4419090). Most research peptides are far longer than that.
BPC-157 is 15 amino acids long. The transporter that could theoretically help absorb intact peptides was designed for the output of the gut's own dismantling process, not for the compounds researchers are trying to get through.
Out of every 100 milligrams in a capsule, 98 or more are destroyed before they reach your blood. That's not a rounding error. That's the structure of the format.
What the Best Pharmaceutical Engineering Has Achieved
Here's a benchmark worth understanding. Drug companies have spent hundreds of millions of dollars trying to solve the oral peptide delivery problem, for compounds worth billions in revenue if they could be put in a pill.
The best result on record is oral semaglutide, marketed as Rybelsus for type 2 diabetes. Novo Nordisk engineered a proprietary absorption enhancer called SNAC, which creates a localized pH rise in the stomach that allows semaglutide to absorb across the stomach wall before the enzymatic environment of the small intestine becomes involved. Dosing conditions are strict: take it alone, 30 minutes before any food, with no more than 120 ml of water.
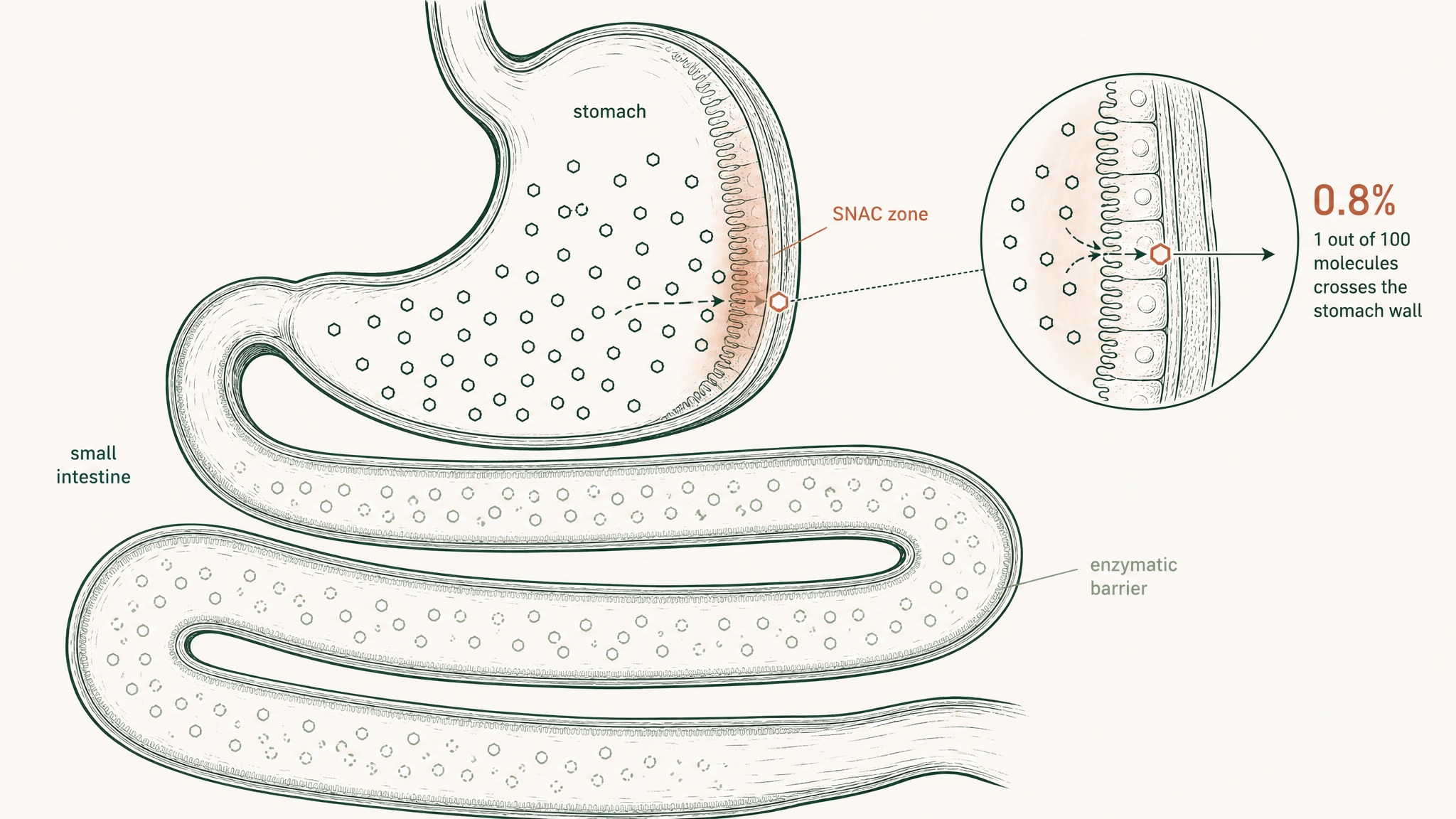
How semaglutide's absorption enhancer helps just 0.8% of the dose cross the stomach before enzymes destroy it.
Under those controlled conditions, absolute bioavailability: 0.8 percent (Overgaard et al. 2021, Clin Pharmacokinet, PMID 33969456).
That's the pharmaceutical ceiling. A decade of engineering targeting one specific peptide, one proprietary absorption technology, strict dosing protocols, and the outcome is 0.8%. Rybelsus works despite that number because semaglutide is extraordinarily potent at very low concentrations. Most research peptides don't have that pharmacological headroom.
No standard peptide supplement capsule uses SNAC technology. No supplement capsule was developed the way Rybelsus was. If the highest pharmaceutical engineering has reached for a single purpose-built compound under controlled conditions is 0.8%, a standard capsule ordered online is working with considerably less.
What the Supplement Industry Doesn't Tell You
The peptide supplement market grew quickly alongside broader consumer interest in longevity, recovery, and performance. That growth created an incentive structure where "peptide capsule" became a marketing category before the underlying delivery problem was resolved.
Most oral peptide supplement products aren't scams in the sense of containing unlisted or counterfeit ingredients. The problem is subtler:
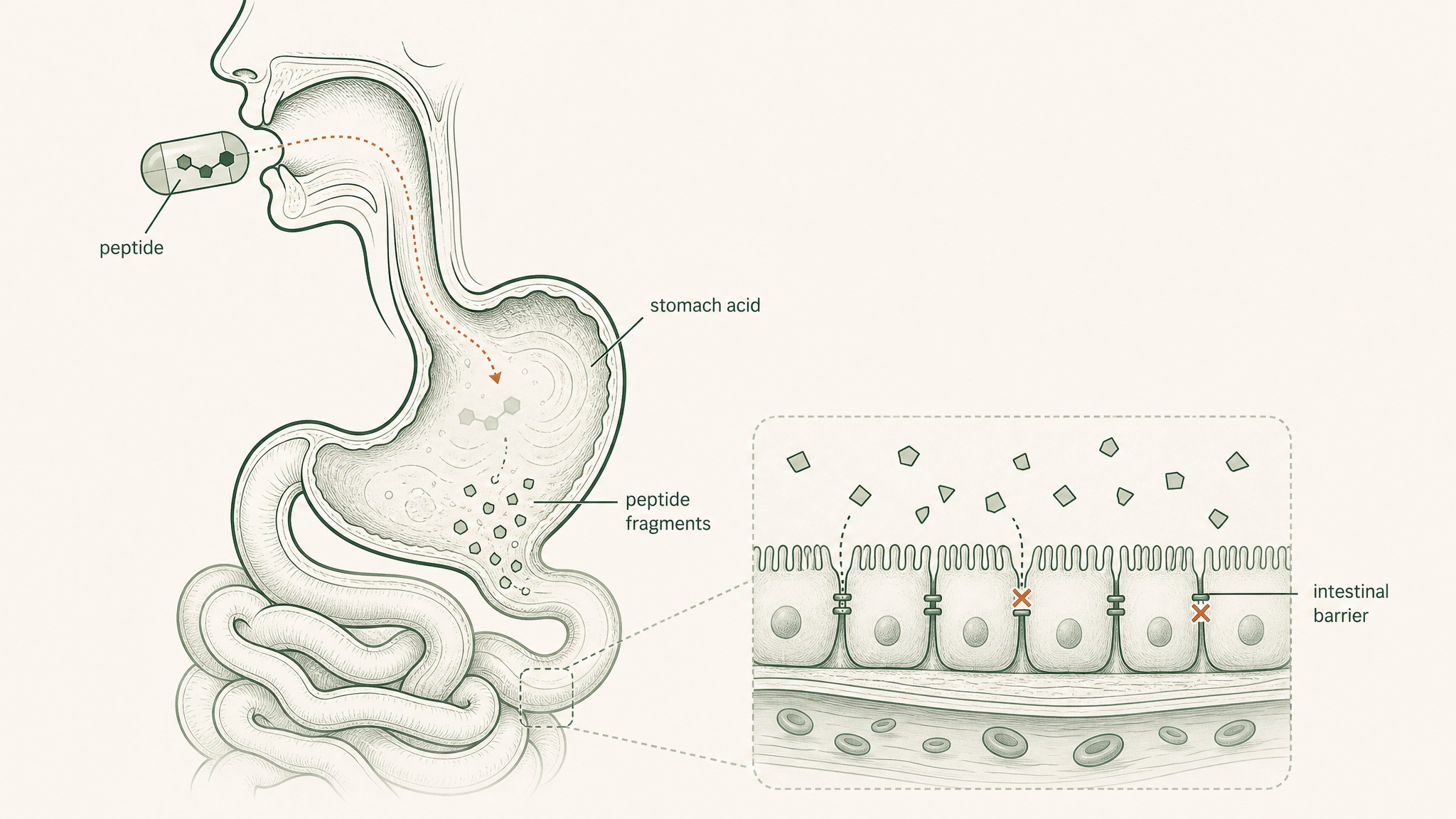
Why peptides swallowed as pills break down in stomach acid before reaching your blood.
- The milligram count on the label may be accurate for what's physically inside the capsule.
- The label won't disclose what happens to those milligrams between your mouth and your bloodstream.
- Marketing language borrows outcomes from injectable research (animal models, in vitro cell studies, subcutaneous injection trials) and implies equivalent results from a swallowed capsule.
Users report a significant experience gap when switching from oral peptide formats to delivery systems that bypass the gut. That gap isn't surprising: it's exactly what the pharmacokinetics would predict. What's notable is how rarely oral supplement brands address this in their own marketing.
Research suggests that outcome claims for oral peptide products frequently don't disclose the delivery mechanism limitations that would qualify those claims. This isn't a fringe critique. It's the documented pharmacological reality of the format.
None of this requires assuming bad intent from every manufacturer. Some brands simply haven't engaged with the delivery science at all. The result is the same either way: a product that can't reliably put the compound you paid for into your bloodstream.
Red Flags: How to Spot a Peptide Pill That Won't Deliver
Not every peptide supplement is actively deceptive. But certain patterns consistently appear in products that can't work as marketed.
- Outcome claims without delivery explanation: a capsule that claims to "support growth hormone release" or "promote collagen synthesis" without explaining how the compound reaches systemic circulation is skipping the most important question.
- No discussion of bioavailability: brands that have engaged with the delivery science address the absorption problem directly. Silence on bioavailability is a meaningful signal.
- Outcomes borrowed from injection research: citing results from studies that used subcutaneous injection or intravenous administration, then implying the same outcomes from an oral capsule, is a direct mismatch between evidence and product format.
- Prices that don't match synthesis costs: pharmaceutical-grade peptide synthesis is expensive. Products priced far below market often contain low-purity material, underdosed amounts, or compounds that haven't passed independent quality testing.
- No certificate of analysis: legitimate research compounds come with third-party documentation showing purity, identity, and absence of contaminants for that specific batch. If you can't find it, you don't know what's in the capsule.
The harder question isn't "is this company fraudulent?" It's simpler: "does this product have any plausible mechanism for delivering what I'm paying for?" With unformulated oral peptide capsules, the pharmacokinetics make that question difficult to answer in the affirmative (regardless of the brand's intentions).
Sublingual Delivery: The Route That Bypasses the Gut
Two delivery routes genuinely sidestep the gut's destruction sequence.
The first is subcutaneous injection, which deposits the compound directly into the vascularized tissue just beneath your skin, bypassing the gastrointestinal tract entirely. It's the reference standard for peptide research because the dose-to-exposure relationship is predictable and consistent.
How sublingual absorption bypasses your stomach, intestines, and liver entirely.
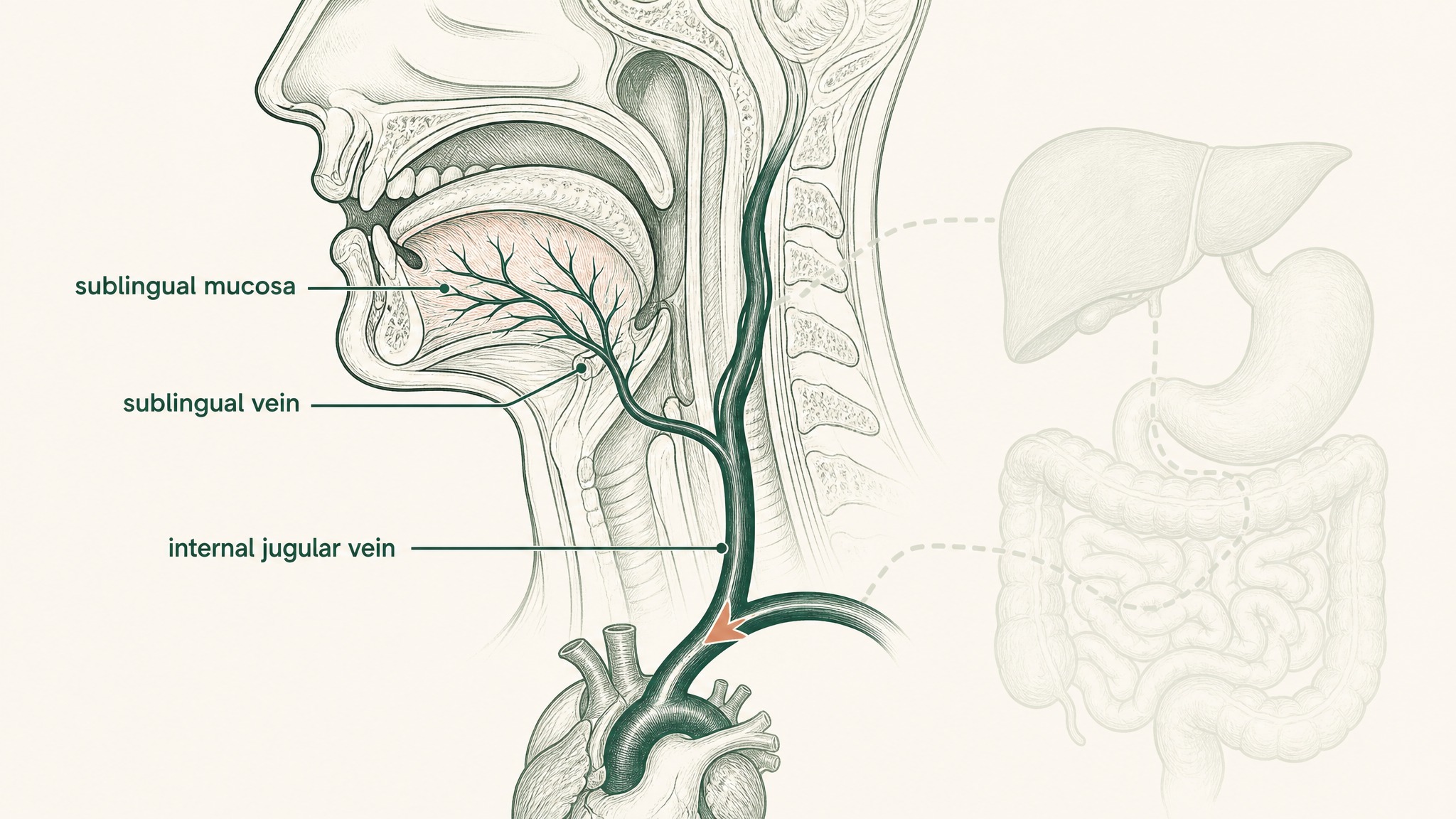
The second is sublingual delivery, absorbing through the mucosal tissue on the underside of your tongue.
The anatomy is what makes it different. The underside of your tongue is lined with thin, non-keratinized epithelium, far more permeable and far less enzymatically aggressive than anything in your digestive tract. Compounds absorbed there drain into the sublingual and lingual veins, entering systemic circulation via the internal jugular and superior vena cava (Zhang, Zhang & Streisand 2002, Clin Pharmacokinet, PMID 12126458). Your stomach, your intestinal enzymes, and your liver's first-pass filter are all out of the picture.
That's five barriers removed, not one.
Members experience significant variation between sublingual peptide products, because the mucosal barrier still exists. It's one barrier instead of five, but it's still a barrier. An unformulated peptide dropped under the tongue doesn't automatically absorb across the sublingual mucosa any more than a peptide in a capsule crosses the intestinal wall.
What makes sublingual delivery actually work is formulation engineering: mucoadhesive polymers that hold the compound against the mucosal surface long enough to absorb, permeation enhancers matched to the peptide's molecular characteristics, and vehicle chemistry designed specifically for the sublingual route. That's the engineering VERO's VERISORB platform is built around. The route creates the opportunity; the formulation is what captures it.
What a Legitimate Peptide Research Product Looks Like
The peptide research product market spans an enormous quality range. Here's what distinguishes the credible end from the rest.
Transparent delivery mechanism: the brand explains specifically how the compound reaches your bloodstream. Not "advanced delivery" as marketing shorthand: an actual mechanism you can evaluate against the pharmacological literature.
Third-party batch testing: independent certificates of analysis, specific to the product batch, from real labs. Not self-reported purity claims. A real document you can verify.
Research-consistent framing: claims stay within what the existing evidence actually supports (often animal models, cell studies, and early human data) rather than extrapolating to therapeutic outcomes that haven't been demonstrated in human trials.
Honest acknowledgment of limits: the brands worth trusting are explicit about what isn't known, where research is at an early stage, and what conditions the evidence applies to.
"Research purposes only" isn't a disclaimer companies add to dodge liability. It's an accurate description of where most peptide compounds sit in the scientific hierarchy: compounds with real and interesting preliminary research behind them, but without the completed human clinical trial data that qualifies a compound for medical use. Saying so clearly is what honesty looks like in this space.
Frequently Asked Questions
Are all peptide pills a scam?
Not in the technical sense of containing counterfeit ingredients. Most oral peptide capsules contain what the label says, but research suggests the format itself delivers less than 1 to 2 percent of the compound into systemic circulation. The deception, where it exists, is usually in marketing outcome claims that the delivery mechanism cannot plausibly produce.
Why can't peptides survive being swallowed?
Peptides are chains of amino acids structurally identical to food protein, and your digestive system is built to dismantle protein. Stomach acid and pepsin begin the breakdown, intestinal peptidases continue it, the epithelial barrier blocks most larger molecules, and hepatic first-pass metabolism takes a final cut. Each stage works sequentially on what survived the previous one.
How is sublingual delivery different from swallowing a pill?
Sublingual absorption occurs through the thin, non-keratinized mucosa under the tongue, which drains directly into systemic circulation via the sublingual and lingual veins. This bypasses the stomach, intestinal enzymes, and hepatic first-pass filter entirely. Research suggests the absorption profile is fundamentally different from oral capsules because five major degradation barriers are removed.
Does enteric coating make oral peptides work?
Enteric coating only protects the capsule from stomach acid. It does not address intestinal peptidases, the epithelial barrier, tight junctions, or hepatic first-pass metabolism. Research suggests enteric coating alone cannot meaningfully raise bioavailability for unmodified peptides because four of the five destruction stages still apply.
What should I look for on a peptide product label?
Look for a transparent delivery mechanism explanation, a batch-specific third-party certificate of analysis, research-consistent claims that match the existing evidence base, and explicit acknowledgment of what is not yet established. Silence on bioavailability or absorption pathway is a meaningful signal that the brand has not engaged with the delivery science.
Is injection the only delivery route that actually works?
Subcutaneous injection is the reference standard because the dose-to-exposure relationship is predictable. Properly formulated sublingual delivery is the other route that bypasses the gut's destruction sequence. Research suggests both routes can deliver intact peptides into circulation, while unformulated oral capsules cannot reliably do so regardless of dose.
Who should avoid oral peptide capsules?
Anyone expecting their results to match the outcomes reported in injectable peptide research should not assume an oral capsule will produce a comparable effect. Research suggests the pharmacokinetic gap between routes is substantial. This content is published for research purposes only and is not medical advice.
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.