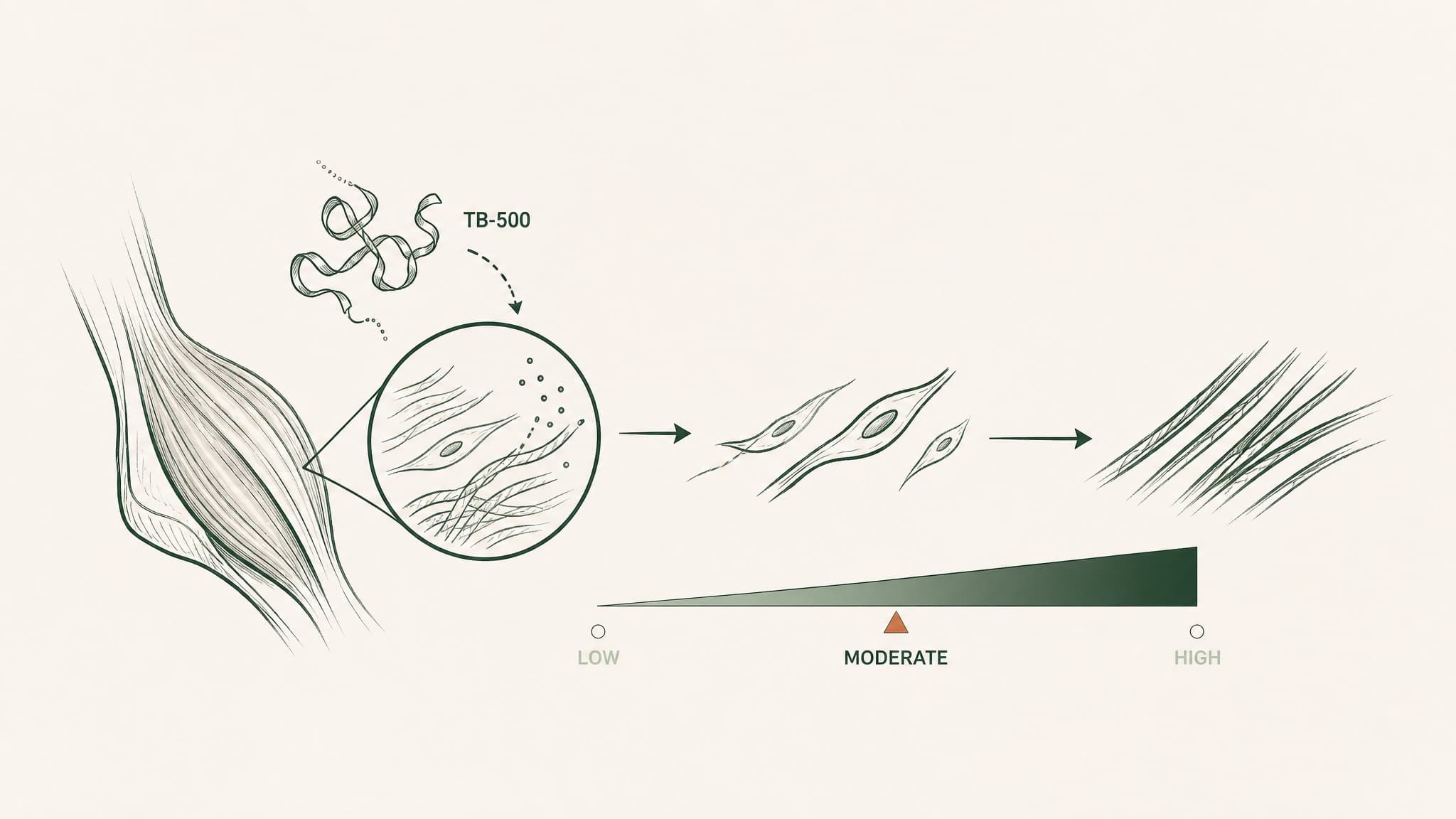
Two researchers can run the same TB-500 protocol and land on different doses. Here are the six variables that shift the standard range. For research only.
Two researchers can run TB-500 at the same milligram-per-week target and watch their cycles play out completely differently. The cause usually isn't the number on the label. It's everything that sits around the number: what they're studying, how they deliver it, where the compound came from, and a handful of biological context variables nobody bothered to write on the protocol sheet.
This guide is about those variables. If you want the standard mg-per-week range, the TB-500 dosage guide covers it. The single-dose calculation framework handles the unit math, and the TB-500 dosing strategy covers the weekly schedule.
This piece covers a different question: given the same range, what shifts a researcher's actual dose decision? Published for research purposes only.
Why do two researchers run the same TB-500 protocol at different doses?
The standard range every researcher anchors to (roughly 5 to 10 mg of TB-500 per week, split across two subcutaneous injections) is real. It's also broad on purpose. That range is a band, not a target, because the right number inside it depends on what the researcher is actually trying to observe.
Six variables consistently shift where a researcher lands inside (or outside) the standard band:
- Research goal and timeline. Acute injury windows look different from sustained recovery research.
- Delivery route. Same number on the label, different number in your bloodstream.
- Source compound variance. What the vial says and what the vial contains aren't always identical.
- Body weight. Less impact than you'd expect inside the 65 to 95 kg band; more outside it.
- Age-related signalling baseline. Endogenous thymosin beta-4 levels shift with age.
- Cycle-to-cycle adjustment. Observed response feeds the next cycle's number.
None of these is a clinical recommendation. There's no FDA-approved human TB-500 dose, so every number below is research convention, not medical guidance. The next six sections walk through each variable, what shifts because of it, and where the published evidence actually lands.
Variable 1: What's the research goal and timeline?
The single biggest input into a TB-500 dose decision is what the research is trying to observe. Acute tissue-injury research and sustained-recovery research use the same compound at very different rhythms.
Here's the basic split:
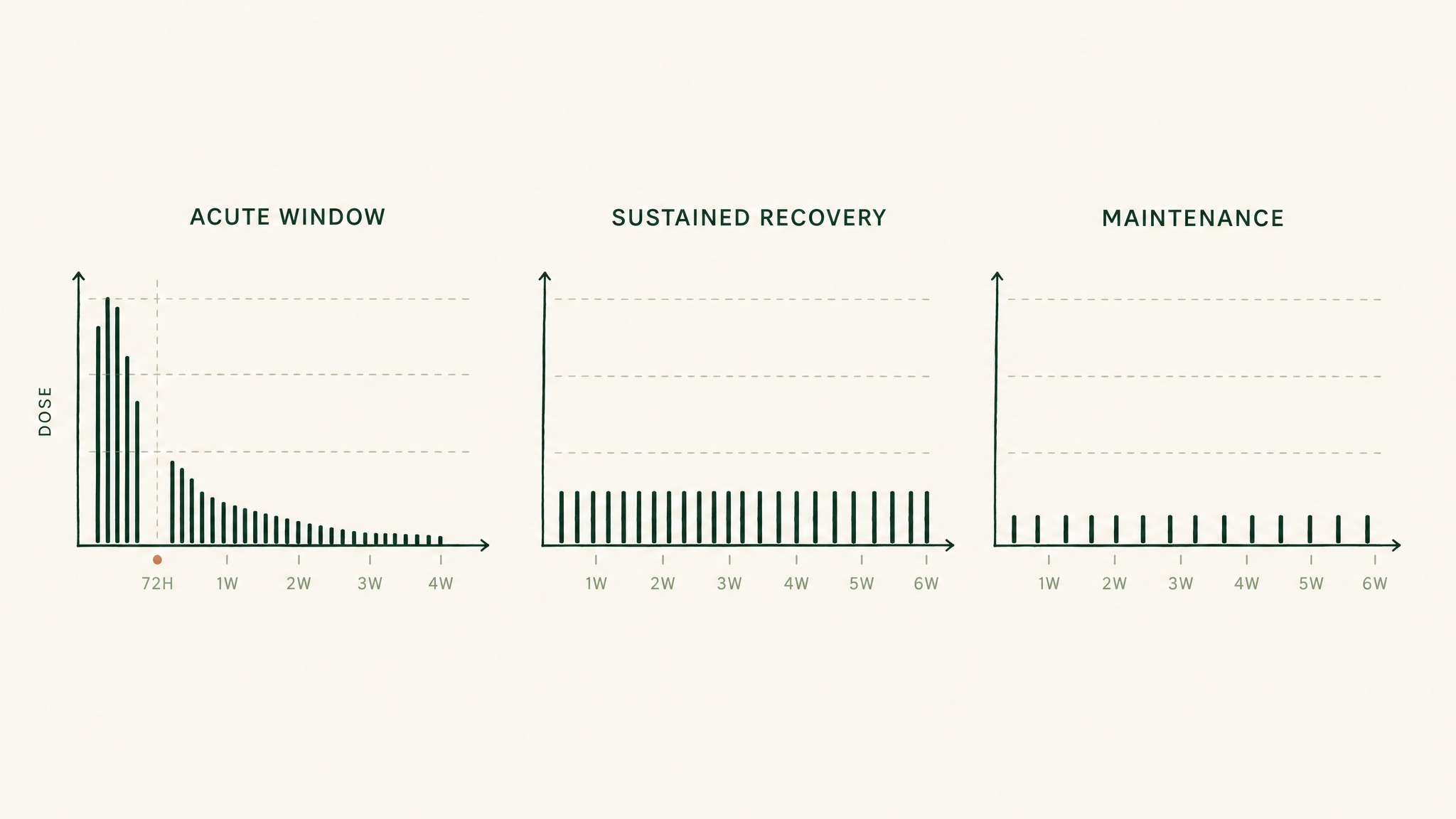
Three dosing schedules for TB-500: acute injury front-loads then tapers, sustained recovery stays steady, maintenance stays low.
- Acute window research (rapid tissue insult, like post-surgical recovery models): higher daily frequency at the start, then taper.
- Sustained recovery research (lower-intensity, weeks-long protocols): twice-weekly steady-state across the cycle.
- Maintenance windows (post-loading observation periods): once-weekly or once every five days at the lower end of the range.
The closest human anchor for the acute pattern is the RGN-352 acute myocardial infarction trial protocol (NCT01311518), which registered three consecutive daily IV bolus doses followed by weekly dosing for four more weeks. The trial was withdrawn before enrollment, but the registered protocol design is the only acute-window human regimen for any thymosin β4 molecule on record.
The rodent acute models agree on the front-loading pattern. In a rat traumatic brain injury model, thymosin β4 was administered intraperitoneally for three consecutive days starting six hours after injury. In a rat embolic stroke model, researchers used every-three-days IP dosing across a longer window.
In both, acute-onset signalling appears to matter more than steady-state exposure.
In the research cycles we've run at Peak Human Labs, the most consistent observation is that researchers studying acute repair windows front-load the first 72 hours and then back off; researchers studying sustained recovery hold steady-state for the full 4 to 6 weeks. The goal sets the rhythm, and the rhythm sets the dose.
For most non-acute research scenarios, twice-weekly inside the standard range is what published protocols converge on.
Variable 2: How does delivery route reshape the absorbed dose?
The same number written on the protocol sheet can deliver very different amounts to your bloodstream depending on how it gets there. Route reshapes the absorbed dose, sometimes by more than an order of magnitude.
Think of it like a delivery van trying to get to your house. The street it takes matters more than the size of the package:
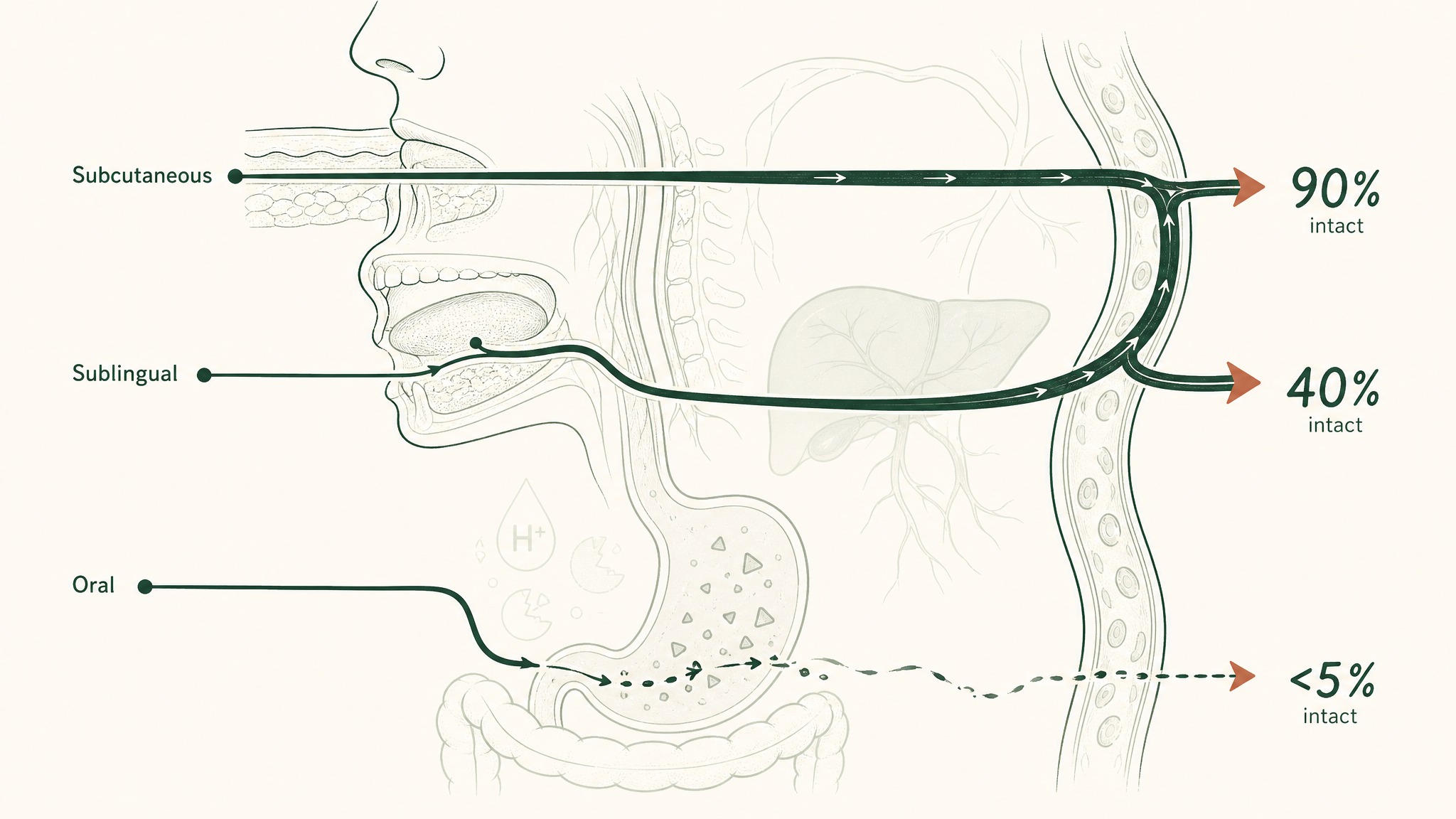
How subcutaneous, sublingual, and oral routes deliver different amounts of peptide to your bloodstream.
- Subcutaneous injection: the van takes the highway. Almost all the package arrives.
- Sublingual mucosal delivery: the van takes a service road that skips the toll bridge (your liver's first-pass metabolism). Most of the package arrives, depending on formulation.
- Standard oral capsule: the van drives through a demolition site (your stomach acid). Almost nothing useful arrives.
Sub-Q (under the skin) injection is the route every standard TB-500 protocol uses, and bioavailability (how much of what you administer reaches your bloodstream) is high. A 2 mg sub-Q dose delivers close to 2 mg of absorbed peptide.
Oral capsules sit at the other end. Peptides are essentially fragile protein chains, and your digestive tract is designed to dismantle protein chains. Most published peptide research treats unprotected oral delivery as not viable for systemic effect.
Sublingual delivery sits in the middle, but the spread is wide. Standard sublingual lozenges or sprays without absorption enhancement often deliver low single-digit percentages. Formulations engineered for mucosal uptake (such as VERO's VERISORB system, used in RESTORE) report bioavailability comparable to subcutaneous administration, which is why the per-dose number tracks the injection range rather than the inflated oral range.
The practical implication: if you change routes mid-cycle without recalculating the absorbed dose, you're effectively running a different protocol.
Variable 3: Does the source compound match what the label claims?
The number on the vial isn't always the number in the vial. Source variance is one of the least-discussed dose decisions and one of the more consequential.
Three sources of variance show up consistently in community-sourced research:
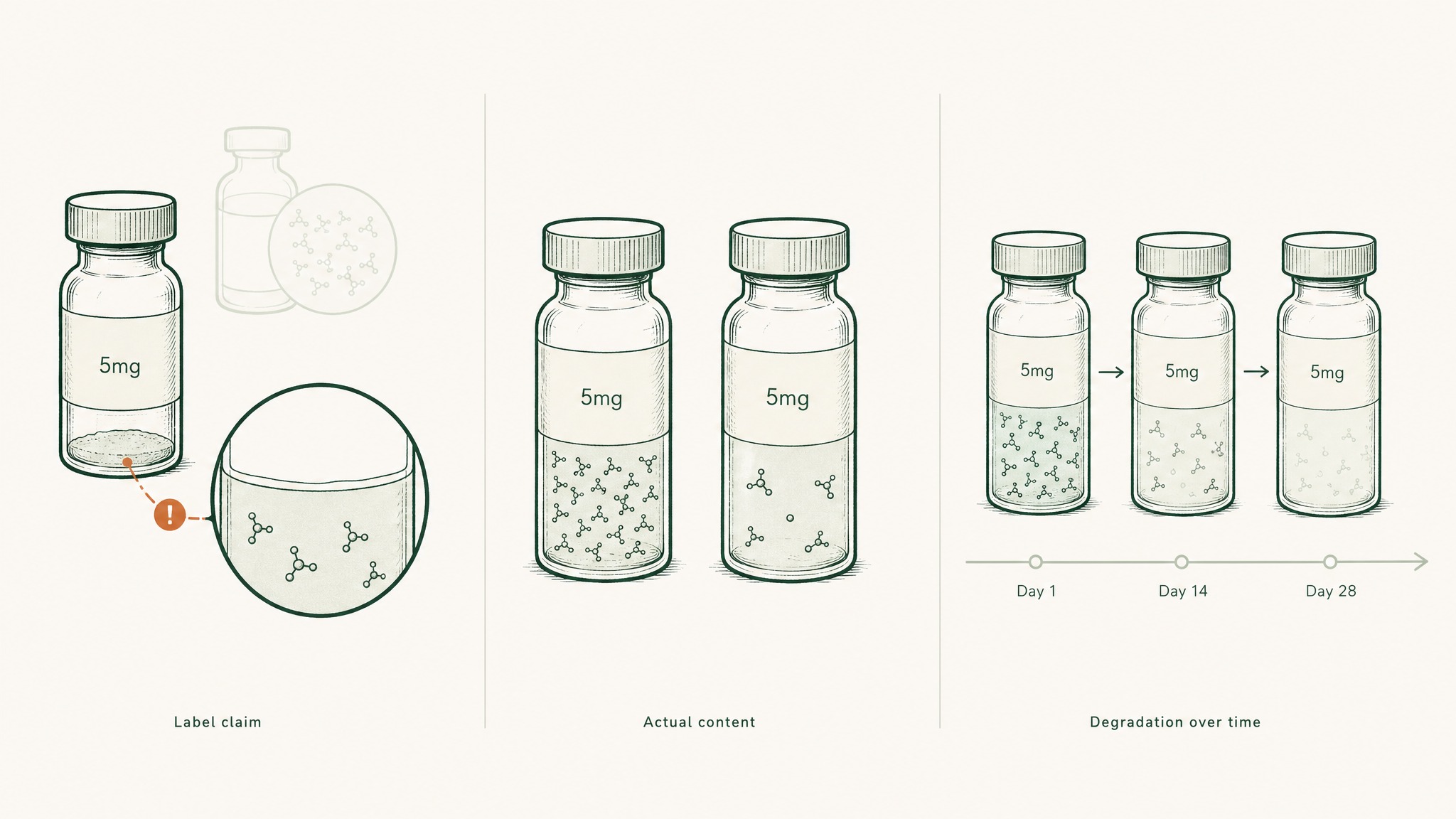
Why the milligrams printed on a peptide vial often don't match what's actually inside.
- Lab-to-lab purity differences. The TB-500 fragment (the seven-amino-acid sequence at positions 17 to 23 of thymosin β4) is short enough that synthesis is straightforward, but purity and correct fragment identity vary across suppliers.
- Batch-to-batch peptide content. Two vials from the same supplier can differ in actual peptide mass, depending on lyophilisation consistency and the supplier's quality control.
- Storage-related degradation. Reconstituted peptides degrade over time. Storage temperature, exposure to light, and time since reconstitution all shift what's actually in the syringe.
Anti-doping researchers characterised the TB-500 fragment structure in 2012 (the seven-amino-acid N-terminally acetylated sequence from positions 17 to 23 of thymosin β4), confirming what the active molecule actually is. Users report wide differences in observed response between vendors, which is consistent with potency variance at the supplier level rather than biological inconsistency.
The conservative defaults that show up in most published protocols:
- Reconstitute fresh each cycle. Don't try to stretch a vial across months.
- Refrigerate (2 to 8°C, never freeze).
- Use within 28 days of reconstitution.
- Source from suppliers that publish third-party HPLC purity reports if you can.
Source variance doesn't change the published dose range. It changes how much faith you should put in any specific milligram label.
Variable 4: How much does body weight actually shift the number?
The honest answer is: less than you'd expect inside the normal adult range, more than you'd expect outside it.
Most published TB-500 protocols use flat dosing. A 70 kg researcher and a 90 kg researcher both run roughly 5 mg sub-Q twice a week, and that's not because the math is sloppy. It's because TB-500's signalling cascade is a switch more than a dial inside a wide concentration band.
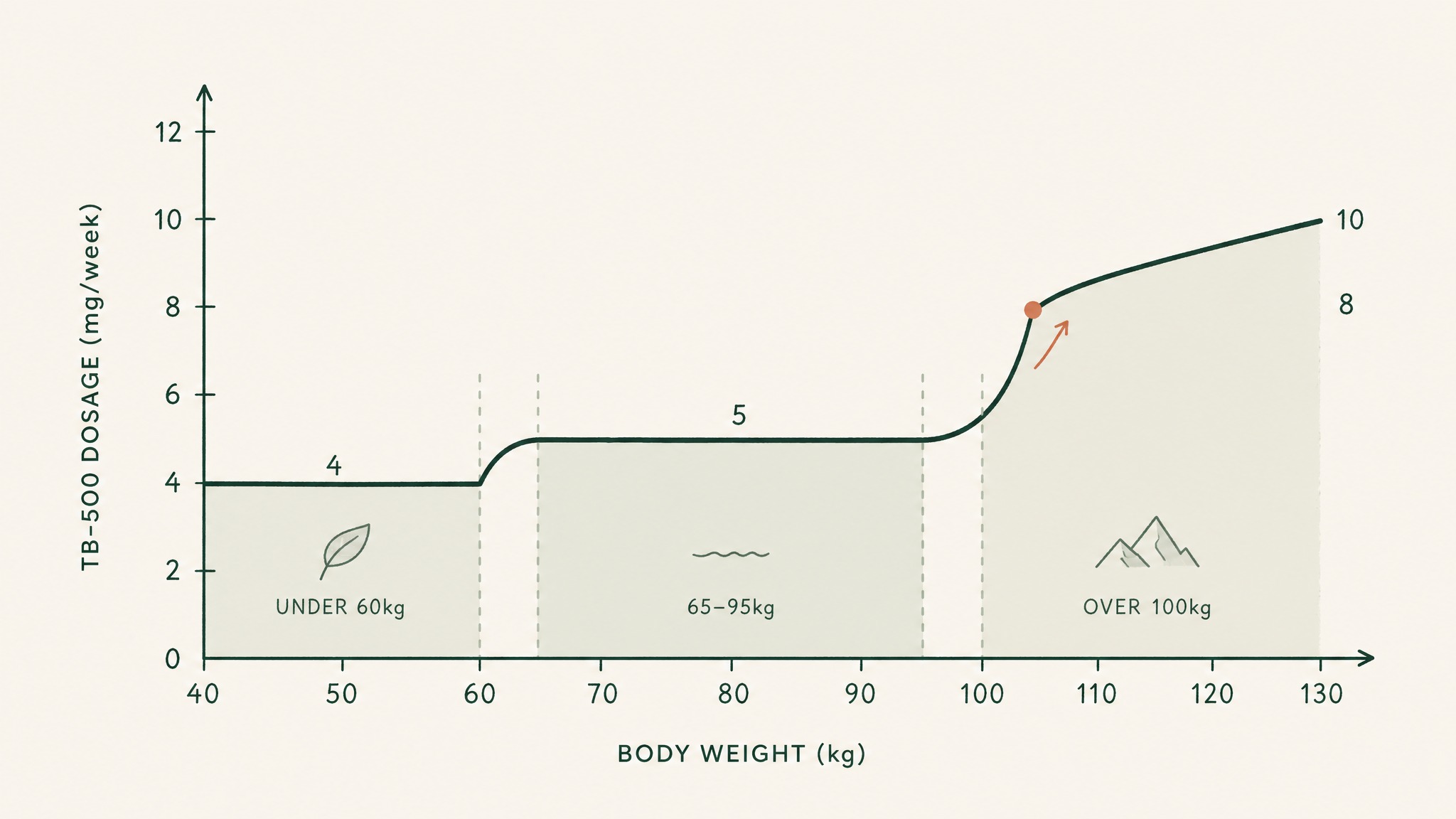
TB-500 dosing stays flat across most adult weights, then rises slightly at extremes.
Below or above that band, the picture shifts:
- Under 60 kg. Standard adult doses sit at the upper end of what's been extrapolated from rodent scaling. Researchers commonly drop to roughly 4 mg twice a week.
- 65 to 95 kg. Inside this band, flat dosing tracks the published protocols closely enough that no scaling is conventional.
- Over 100 kg. Researchers commonly run at the upper end of the standard range, around 8 to 10 mg per week, but the FDA's interspecies scaling guidance flattens above roughly 90 kg human body surface area.
The interspecies scaling method most researchers use (FDA 2005 Human Equivalent Dose guidance, reinforced by Reagan-Shaw et al. 2008 in FASEB Journal) is based on body surface area, not body weight. Body surface area scales sub-linearly with weight, which is why a heavier researcher doesn't need a proportionally heavier dose.
The practical guidance: only scale by body weight if you're at the extremes of the adult range. Inside it, flat dosing is the convention.
Variable 5: What's your age-related signalling baseline?
Your body produces thymosin beta-4 endogenously, and the broader regenerative-signalling environment downshifts with age. That changes the signalling baseline TB-500 administration is layering on top of, which is why the same dose can land differently for a 30-year-old and a 55-year-old researcher.
Endogenous thymosin β4 (the parent molecule TB-500 is a fragment of) is one of the most abundant intracellular peptides in your body, with substantial pools in platelets, white blood cells, and various tissue stores. Research suggests TB-4-driven signalling tracks the broader age-related decline in regenerative biology, although a precise human age curve hasn't been published.
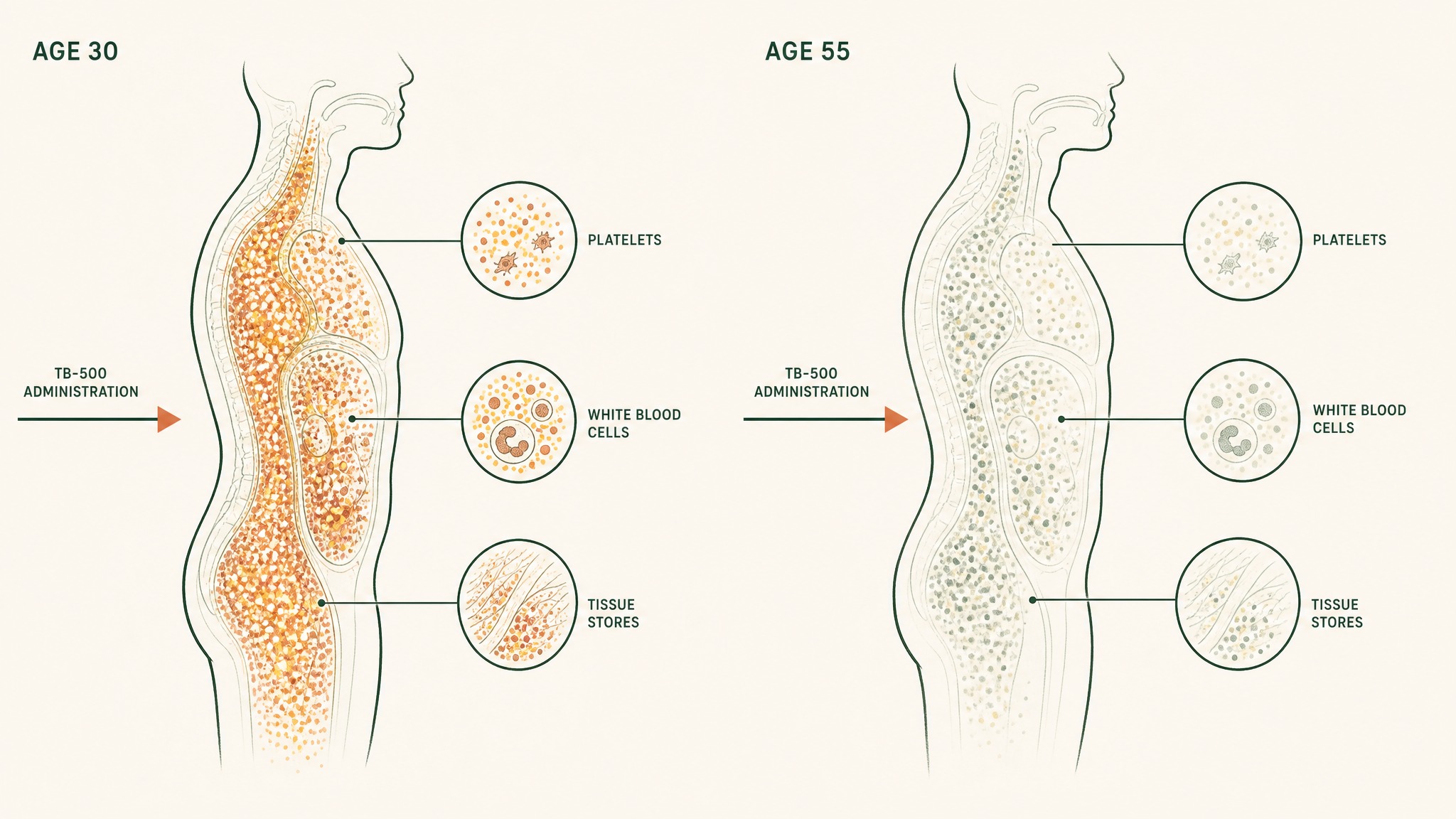
How the same TB-500 dose adds to a lower regenerative baseline in your fifties than your thirties.
The simplest way to think about it: your body's repair-signal factory runs at higher output in your twenties than it does in your fifties. The same TB-500 administration adds the same amount of signalling capacity to whatever your baseline is. The total signal is baseline plus administration; the administration alone is constant, but the baseline you're adding to isn't.
Three honest caveats:
- No human protocol has been calibrated to age in published research.
- The dose doesn't shift mechanically with age inside the standard range.
- What can shift is the cycle structure (longer loading windows, longer maintenance), not the per-dose mg.
For most researchers in the 30 to 65 age band, this variable shifts strategy more than the dose itself. The number stays in the standard range; the cycle pattern adapts.
Variable 6: How do researchers adjust the dose between cycles?
The last and most under-discussed variable is the feedback loop. The dose you start with on cycle one isn't necessarily the dose you'll run on cycle three, because the data you collect between cycles changes the decision.
There's no validated blood marker for TB-500 status in research, which means researchers can't titrate against a number the way you would with a hormone or a vitamin. What they can track is a small set of observable signals across the cycle:
- Recovery time between training sessions
- Soft tissue stiffness and joint discomfort during loading
- Sleep quality (anecdotally responsive in research community reports)
- Subjective inflammation markers (swelling, bruising response, wound closure timing where relevant)
- Adverse-effect signals (injection-site response, lethargy, headache)
Three adjustment patterns show up across published and community protocols:
- No-change cycles. If cycle one delivered the observed signal in the expected window, cycle two runs the same number.
- Frequency adjustments. Shift twice-weekly to every-five-days, or vice versa, before changing the mg.
- Route adjustments. Move from sub-Q to validated sublingual or back, holding the mg constant.
Most researchers exhaust frequency and route adjustments before changing the mg figure itself. Changing too many variables at once collapses the signal: you can't tell which change drove the difference.
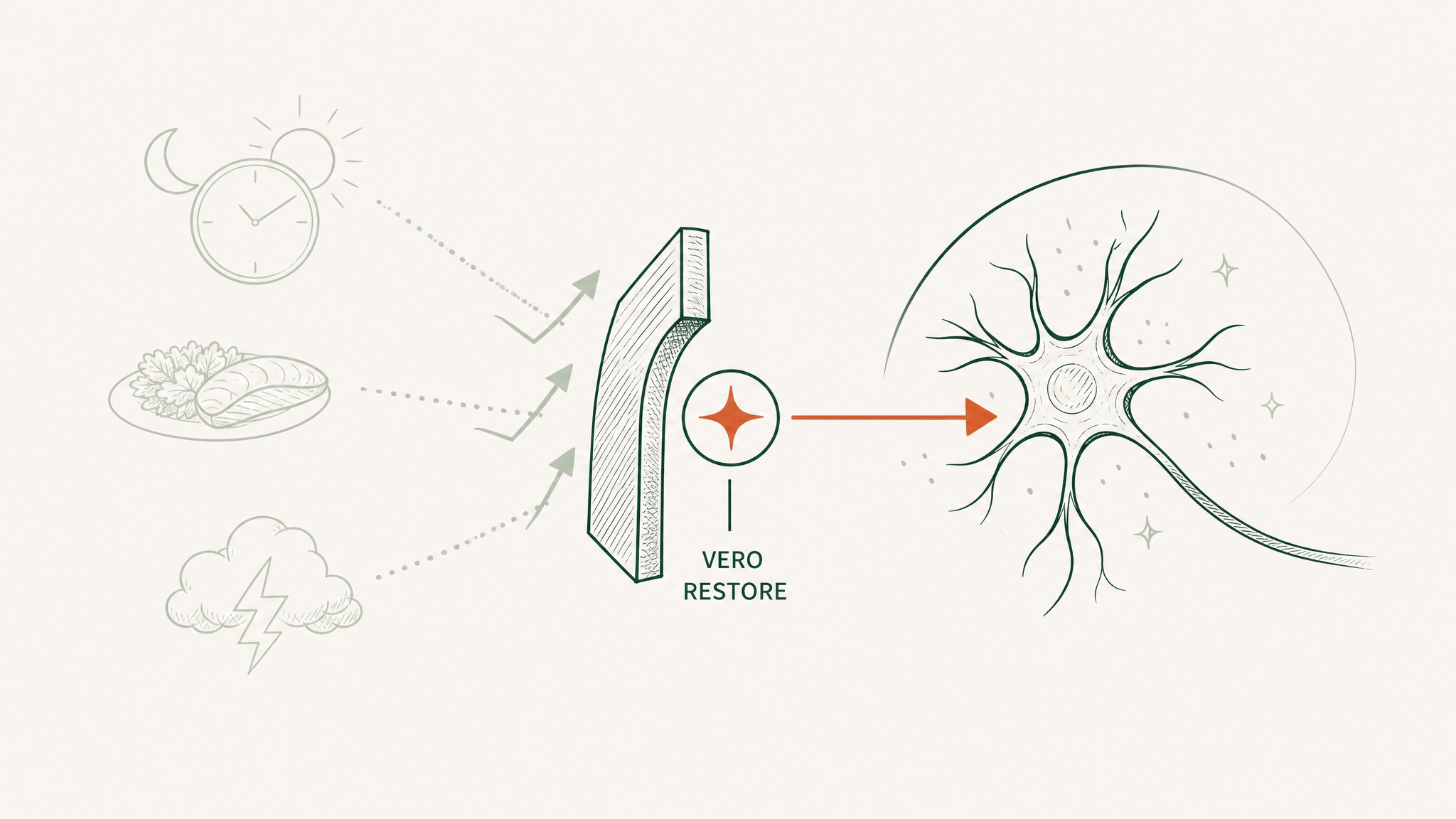
Where does VERO RESTORE fit if you don't want to manage these variables?
Most of the variables above are the cost of self-administering injectable research peptides. Source variance, reconstitution drift, route calculations, weekly scheduling: all of it sits on you when you're running a vial-and-syringe protocol.
RESTORE is the VERO tissue-repair protocol built around sublingual delivery using the VERISORB Quicksome platform, which engineers peptides for mucosal uptake at bioavailability comparable to subcutaneous injection. Members experience a structured protocol without the operational overhead of an injectable cycle:
VERO RESTORE delivers a standardized dose without reconstitution or storage variables.
- No reconstitution math (no vials, no bacteriostatic water, no insulin syringes).
- No storage drift to manage; the formulation is shelf-stable inside the prescribed window.
- No route-to-route absorbed-dose recalculation; the per-dose figure is standardised.
The variables are managed at the formulation layer, not the protocol sheet. RESTORE isn't a substitute for an injectable cycle, and it doesn't change the underlying TB-500 research base. It's a different way of holding the dose constant so the only variable that matters is the one you're actually researching.
Frequently Asked Questions
Is there a single right dose for TB-500? No. The published research community converges on roughly 5 to 10 mg per week split across two subcutaneous administrations, but no FDA-approved human dose exists. Every number is extrapolated from rodent data, and the right figure inside the band shifts with the six variables covered above.
Does dose scale with body weight in TB-500 protocols? Inside the 65 to 95 kg adult band, most published protocols use flat dosing. Below 60 kg, researchers commonly drop to the lower end of the range. Above 100 kg, the FDA interspecies scaling guidance flattens, so researchers stay near the upper end of the standard range rather than scaling proportionally.
How does delivery route change the dose? Sub-Q injection delivers close to 100% of the nominal dose. Standard oral capsules deliver low single-digit percentages because of gastric and first-pass degradation. Engineered sublingual delivery (such as VERISORB) reports bioavailability comparable to sub-Q. If you change routes, recalculate the absorbed dose rather than holding the label number constant.
Should you change the dose between cycles? Most researchers exhaust frequency and route adjustments before shifting the mg figure. Changing too many variables at once collapses the signal. If cycle one delivered the observed response, cycle two often runs the same number.
Does age change the TB-500 dose? Not the per-dose mg, inside the standard range. What can shift is cycle structure: older researchers commonly run longer loading windows and longer maintenance phases. The dose stays in the published band; the rhythm adapts.
Can you combine TB-500 dosing variables across protocols? You can, with caution. The TB-500 dosing schedule guide covers how researchers stack TB-500 with BPC-157 in the recovery research stack. The principle is the same: change one variable at a time, hold the rest constant, so you can read the signal.
Key Takeaways
- The standard TB-500 range (5 to 10 mg per week, twice-weekly sub-Q) is a band, not a single number. Six variables decide where a researcher lands inside it.
- The biggest variable is research goal: acute-window protocols front-load and taper; sustained-recovery protocols hold a steady twice-weekly rhythm for 4 to 6 weeks.
- Route reshapes the absorbed dose more than any other variable. Sub-Q and engineered sublingual (such as VERISORB) deliver close to the nominal dose; standard oral capsules deliver a small fraction.
- Source compound variance is real and under-discussed. Lab purity, batch consistency, and reconstitution stability all shift what's actually in the syringe.
- Body weight matters less than expected inside 65 to 95 kg. Outside that band, scaling is conventional.
- Age shifts the cycle structure more than the per-dose mg. The published band still applies; the rhythm adapts.
- Adjust frequency and route before adjusting the mg figure. Changing too many variables at once collapses the observation.
References
- Ruff D, Crockford D, Girardi G, Zhang Y. (2010). Single and multiple dose study of intravenous thymosin beta-4 in healthy volunteers (Phase I PK trial). Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536472/. Retrieved 2026-06-08.
- Reagan-Shaw S, Nihal M, Ahmad N. (2008). Dose translation between animal and human studies, revisited. FASEB Journal. https://pubmed.ncbi.nlm.nih.gov/17942826/. Retrieved 2026-06-08.
- Goldstein AL, Hannappel E, Kleinman HK. (2005). Thymosin beta-4: actin-sequestering peptide with tissue-repair signalling: review of animal-model evidence. Trends in Molecular Medicine. https://pubmed.ncbi.nlm.nih.gov/16099219/. Retrieved 2026-06-08.
- Crockford D, Turjman N, Allan C, Angel J. (2010). Thymosin beta-4: structure, function, and biological properties supporting research applications. Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536467/. Retrieved 2026-06-08.
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. (2012). Thymosin β4 as a multifunctional regenerative peptide: review of basic properties and clinical applications. Expert Opinion on Biological Therapy. https://pubmed.ncbi.nlm.nih.gov/22074294/. Retrieved 2026-06-08.
- Philp D, Kleinman HK. (2010). Animal studies of thymosin beta-4 in tissue repair and regeneration (review). Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536453/. Retrieved 2026-06-08.
- Xiong Y et al. (2012). Thymosin β4 dosing schedule in a rat traumatic brain injury model (daily IP for three days). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC3392183/. Retrieved 2026-06-08.
- Morris DC et al. (2014). Thymosin β4 dose-response in a rodent embolic stroke model (every-three-days IP dosing). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4177939/. Retrieved 2026-06-08.
- Esposito S et al. (2012). Synthesis and characterisation of the N-terminal acetylated 17-23 fragment of thymosin beta-4 identified in TB-500. Drug Testing and Analysis. https://analyticalsciencejournals.onlinelibrary.wiley.com/doi/abs/10.1002/dta.1402. Retrieved 2026-06-08.
- RegeneRx Biopharmaceuticals. RGN-352 IV thymosin beta-4 dosing regimen in acute myocardial infarction (trial protocol summary, NCT01311518). ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT01311518. Retrieved 2026-06-08.
- U.S. FDA, Center for Drug Evaluation and Research. Guidance for Industry: Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers. July 2005. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/estimating-maximum-safe-starting-dose-initial-clinical-trials-therapeutics-adult-healthy-volunteers. Retrieved 2026-06-08.
Want a TB-500 cycle without the reconstitution math, source variance, and route recalculation? Explore RESTORE →
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.