What does one TB-500 dose actually mean? Unit conversions, body-weight scaling, and the calculation framework researchers use to land on a single number.
The question "what's the TB-500 dose?" sounds like it should have one answer. It doesn't, and the reason isn't dodgy science. Anyone working from a structured research protocol runs into the same ambiguity: "dose" is a slippery word, and the same number on a research label can mean three different things depending on who's reading it.
This guide is about the unit itself. Not the weekly range (that lives in the TB-500 dosage guide), not the schedule (covered in the TB-500 dosing strategy). Just the single number, where it comes from, and what changes between the dose you write down and the dose your tissue actually sees. All content is published for research purposes only.
Key Takeaways
- A TB-500 "dose" is a single administration, not a weekly total. Confusing the two is the most common calculation error.
- Doses are reported in three conventions (mg/kg, mcg per dose, weekly total mg). Identify the convention before copying any number.
- The standard single-dose anchor of ~5 mg per administration for an 80 kg adult is derived from FDA body-surface-area scaling of rodent data, not from a human clinical trial.
- Body-weight scaling matters most under 60 kg and over 100 kg. Inside the 70 to 85 kg band, a flat dose is close enough.
- Route changes the absorbed dose dramatically. The same 2 mg nominal dose can deliver 1.9 mg via injection or a few hundred mcg via oral capsule.
- Sublingual delivery (VERO VERISORB) keeps the absorbed dose close to the nominal dose without injection overhead, which makes single-dose calculations more reliable.
- Practical dose precision is limited by reconstitution math, not just by calculation. Vial concentration sets the floor on what you can accurately draw.
What does "one TB-500 dose" actually mean?
In research, a "dose" is a single administration, not a weekly total. When a paper says the dose was 100 micrograms (mcg), it means each injection delivered 100 mcg of the peptide, on the schedule the study used.
That's the simplest definition, and it's where most confusion starts. Researchers report doses in at least three different framings, and you can read the same protocol three different ways:
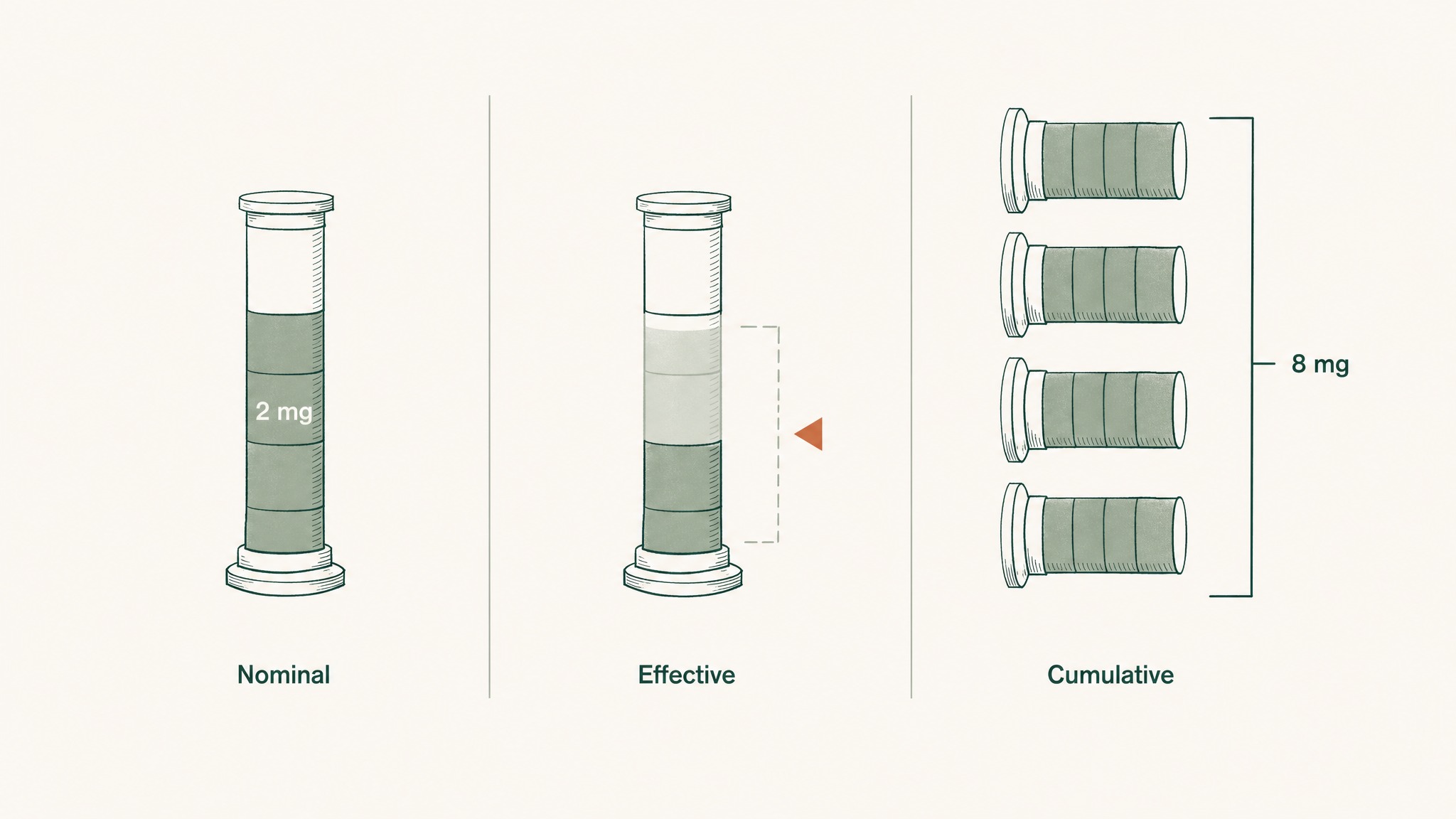
Same TB-500 dose measured three ways: what's drawn up, what reaches your blood, and what adds up over weeks.
- Nominal dose: what's written on the syringe. 2 milligrams (mg) means 2,000 mcg of peptide drawn up.
- Effective dose: what reaches your bloodstream after the body's gatekeepers (stomach, liver, skin barrier) take their cut.
- Cumulative dose: what's been delivered over the cycle (4 weekly doses of 2 mg = 8 mg cumulative).
Same word, three measurements. A "low dose" in one paper is a "moderate dose" in another because the framing shifted.
The unit itself is the next thing to settle. TB-500 protocols use micrograms, milligrams, and milligrams per kilogram of body weight (mg/kg) interchangeably, and the conversion is where most calculation errors creep in. One milligram is 1,000 micrograms. A "100 mcg dose" is one-tenth of a milligram. A "2 mg dose" is 2,000 mcg. Get that wrong and you're off by a factor of ten.
Why is the same TB-500 dose written in so many different ways?
Because peptide research borrowed its dose conventions from three different traditions, and none of them agreed on the units. Pharmacology uses mg/kg. Animal-model labs use mcg per administration. Community research forums use total weekly mg.
Here's what the same dose looks like across the three conventions, for an 80 kg adult on a twice-weekly protocol:
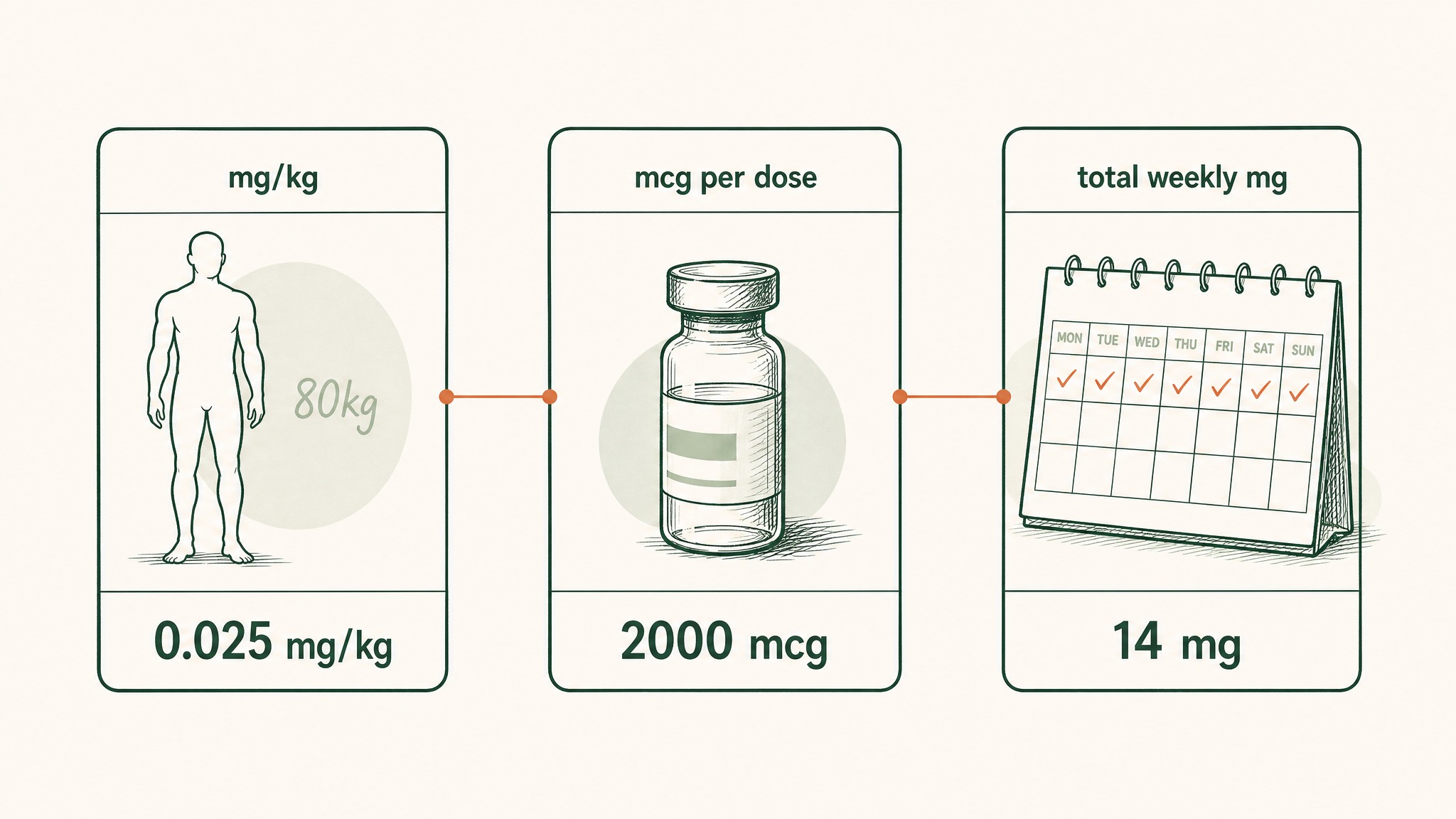
The same TB-500 dose expressed in three different measurement systems used across research fields.
| Convention | What it says | What it means |
|---|---|---|
| mg/kg (pharmacology) | 0.025 mg/kg per dose | 25 mcg of peptide per kilogram, per administration |
| mcg per dose (animal labs) | 2,000 mcg per dose | A single 2 mg administration |
| total weekly mg (community) | 4 mg per week | The cumulative mg over the week, ignoring per-dose math |
All three describe the same protocol. They sound completely different.
A second wrinkle: some sources list TB-500 doses in international units (IU), which is a regulatory unit borrowed from biologics. Thymosin Beta-4 doesn't have a standardised IU-to-mg conversion in the published research, so any source quoting IU should be read with caution. Stick with mass units (mg or mcg) and you avoid the trap.
The takeaway: when you read a research dose, identify which convention the source is using before you copy the number. A "2 mg dose" only matches another "2 mg dose" if both are talking about the same per-administration unit.
Should you scale your TB-500 dose by body weight?
This is the single biggest decision in single-dose calculation, and the published research split is roughly down the middle.
The case for body-weight scaling is that peptides distribute through extracellular fluid, and a larger body has more of that fluid to fill. A flat 2 mg dose in a 60 kg researcher delivers a higher concentration to the tissue compartment than the same 2 mg in a 100 kg researcher. The FDA's interspecies dose-translation guidance, used to convert animal doses into human doses, is built on body surface area, which itself scales with weight (FDA 2005 HED guidance; Reagan-Shaw et al., 2008).
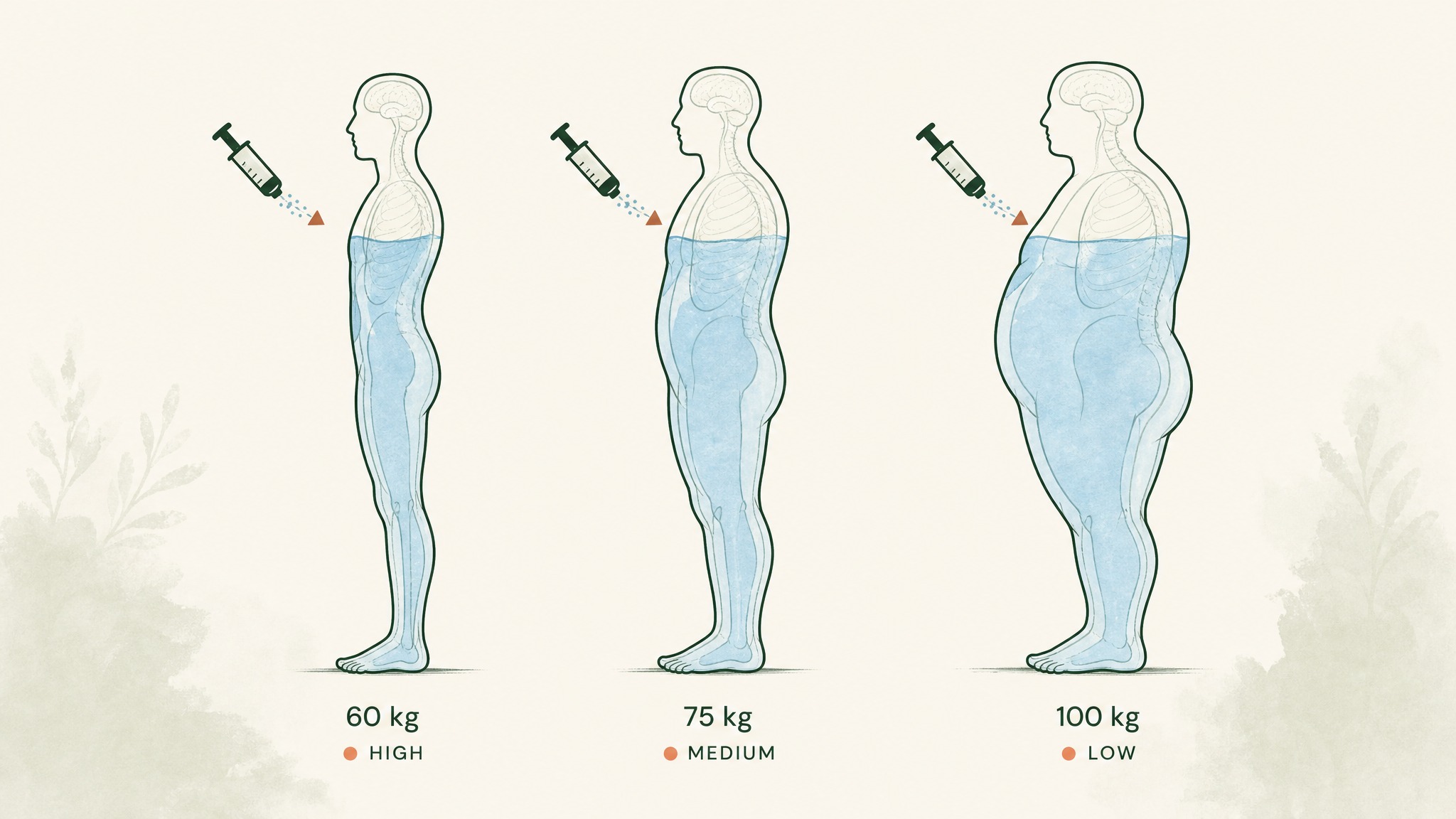
How the same TB-500 dose disperses differently depending on body size and extracellular fluid volume.
The case for a flat dose is practical. Most research-grade TB-500 vials are sold as a fixed 5 mg or 10 mg lot, and most community protocols pre-calculate per-administration doses for a "standard" 70 to 80 kg adult. Adjusting per-kilogram introduces reconstitution math most researchers don't want to redo for every cycle.
In our protocol design at VERO, we've learned that body-weight scaling matters most at the extremes (under 60 kg or over 100 kg) and matters least in the 70 to 85 kg middle band where most published flat-dose protocols were calibrated. Inside that band, a flat dose and a weight-scaled dose come out within 15% of each other, which is well inside the noise of route-driven absorption variance.
A simple rule:
- Under 60 kg: drop the standard flat dose by roughly 20%
- 60 to 85 kg: use the flat dose as published
- Over 100 kg: increase the flat dose by roughly 20%, or recalculate using mg/kg
That's not a clinical recommendation; it's a research-context working rule, and members experience varying responses regardless of how they scale. The peptide's actin-binding and migration-signalling effects are reported as concentration-dependent in cell models (Crockford et al., 2010), which is the mechanism reason scaling shows up in the first place.
What's the difference between the dose you administer and the dose your tissue sees?
This is where the nominal dose and the effective dose diverge, and it's the gap that matters most for whether your research protocol delivers what you think it does.
When you administer 2 mg of TB-500 subcutaneously, somewhere between 80% and 95% of that peptide is generally considered to reach systemic circulation (the published Thymosin Beta-4 pharmacokinetic data in healthy human volunteers used the intravenous route, which is the only published human PK reference; subcutaneous estimates are extrapolated). Research suggests an oral capsule of the same 2 mg delivers a fraction of that, because the seven-amino-acid peptide is largely degraded by stomach acid and intestinal enzymes before it can cross into the bloodstream.
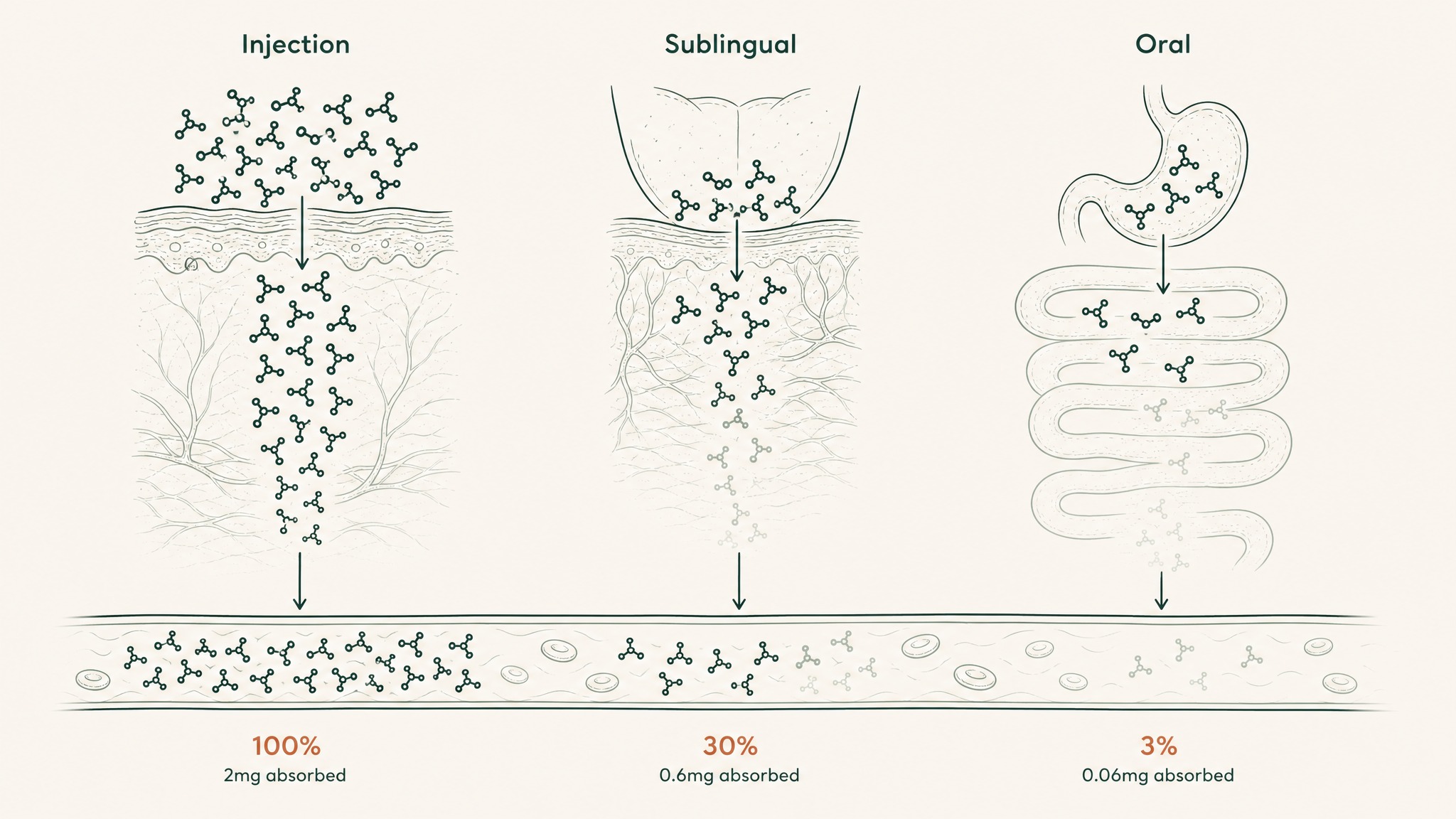
How the same 2mg dose delivers vastly different amounts to your bloodstream depending on route.
In our protocol design, we've learned that the gap between the nominal dose and the absorbed dose is where most research dosing inconsistency lives. Two researchers running identical mg numbers can deliver very different molecular signals depending on route:
- Subcutaneous injection: high systemic delivery, slow steady release from the injection depot
- Sublingual absorption: moderate systemic delivery, fast onset, bypasses the digestive tract
- Oral capsule: low and variable systemic delivery, slow onset, exposed to gut and liver before bloodstream
The same 2 mg "dose" can be 1.9 mg of absorbed peptide via injection, 0.4 to 0.8 mg via sublingual, or a few hundred micrograms via oral. Route is not a small variable. It's the variable.
VERO's RESTORE protocol is built on sublingual VERISORB delivery for exactly this reason: the absorbed dose stays close to the nominal dose without the syringe overhead, which keeps single-dose calculations honest. For the deeper bioavailability comparison, see the oral vs injectable peptides study.
How do researchers calculate a single TB-500 dose from study data?
There's no human TB-500 clinical trial. There's one published human pharmacokinetic study (Ruff et al., 2010) and it used full-length Thymosin Beta-4 via intravenous infusion, not the truncated TB-500 fragment via subcutaneous injection. So every single-dose number you'll read for TB-500 is the output of a two-step calculation:
- Start with a rodent study dose (almost always rat or mouse)
- Translate that dose into a human-equivalent number using the FDA's body-surface-area scaling factor
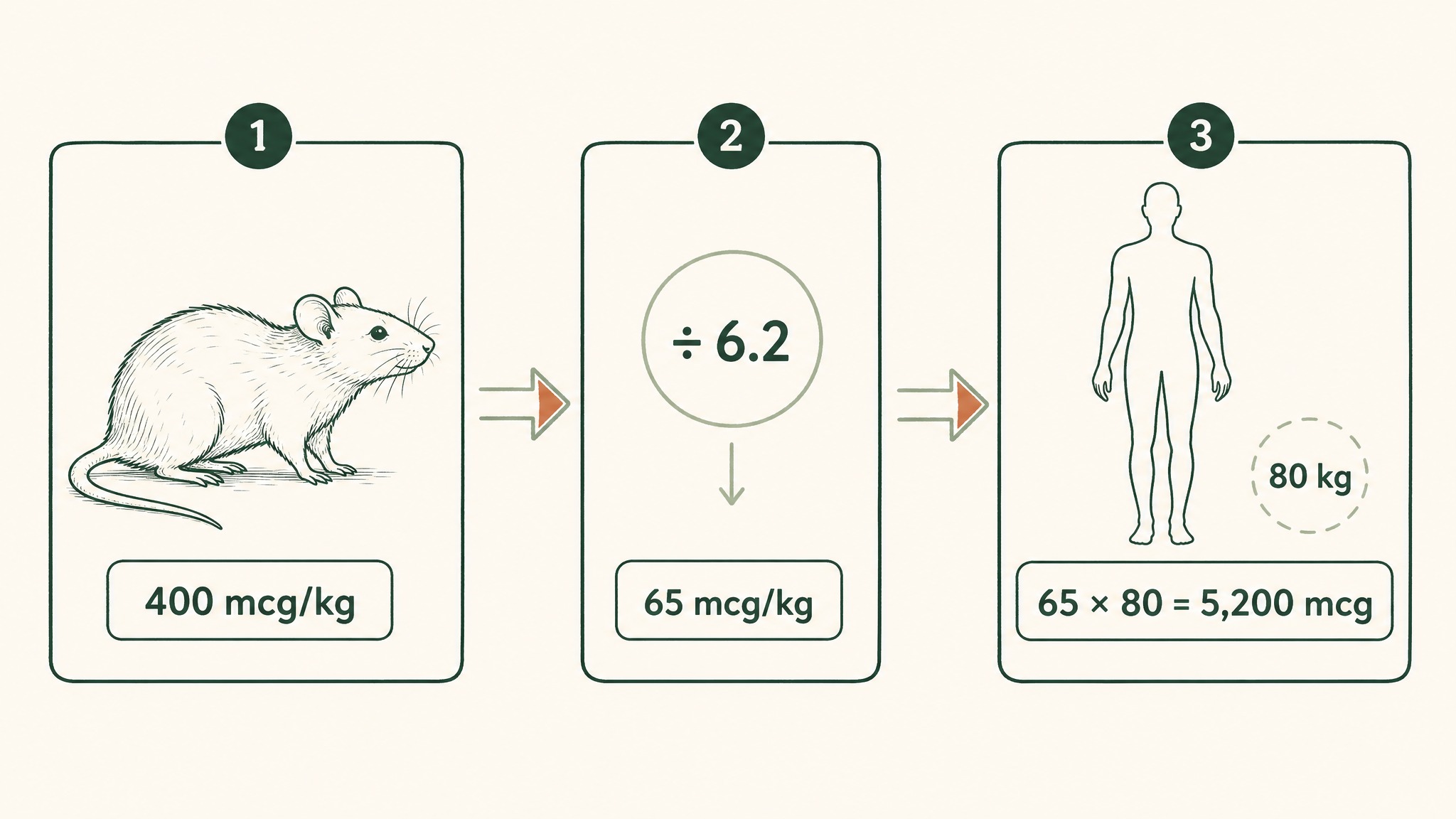
How researchers convert a rat study dose into a human-equivalent TB-500 dose using body weight scaling.
The translation step uses a conversion factor of about 6.2 for rats (Reagan-Shaw et al., 2008). You divide the rat mg/kg dose by 6.2 to get the human-equivalent mg/kg, then multiply by your body weight.
Here's what that looks like for a single dose, using a rat study dose of 400 mcg/kg as the starting point:
- Rat dose: 400 mcg/kg
- Human-equivalent: 400 ÷ 6.2 = ~65 mcg/kg
- For an 80 kg adult: 65 × 80 = ~5,200 mcg per administration
- Convert to mg: 5,200 ÷ 1,000 = ~5.2 mg per administration
That 5.2 mg figure is where the "single TB-500 dose" anchoring number comes from. It's not validated in a clinical trial. It's a body-surface-area translation from animal data, and it's the input that every TB-500 dosing guide is implicitly using even when they don't show the working.
The published human pharmacokinetic study of full-length Thymosin Beta-4 (Ruff et al., 2010) used intravenous doses of 42, 140, 420, or 1,260 mg, given either as a single administration or daily across 14 days, and reported the compound was well tolerated with no evidence of dose-limiting toxicity. Those numbers sit far above any subcutaneous research dose used for the smaller TB-500 fragment, which is one reason the safety data isn't applied directly as a dose-finding source for TB-500 protocols.
What changes a single TB-500 dose decision?
Once you have the anchor number (somewhere around 5 mg per administration for an 80 kg adult on the FDA HED translation), the next question is whether your dose should be that number or something else. Five variables move the decision:
- Body weight: as covered above, scale up or down at the extremes
- Research target: tissue-repair research tends toward the upper range, maintenance research toward the lower
- Route: injection delivers more of the nominal dose than sublingual delivers more than oral
- Cycle phase: loading windows use higher per-dose numbers, maintenance windows use lower
- Vial concentration: the practical limit of how cleanly you can draw a precise dose from a reconstituted vial
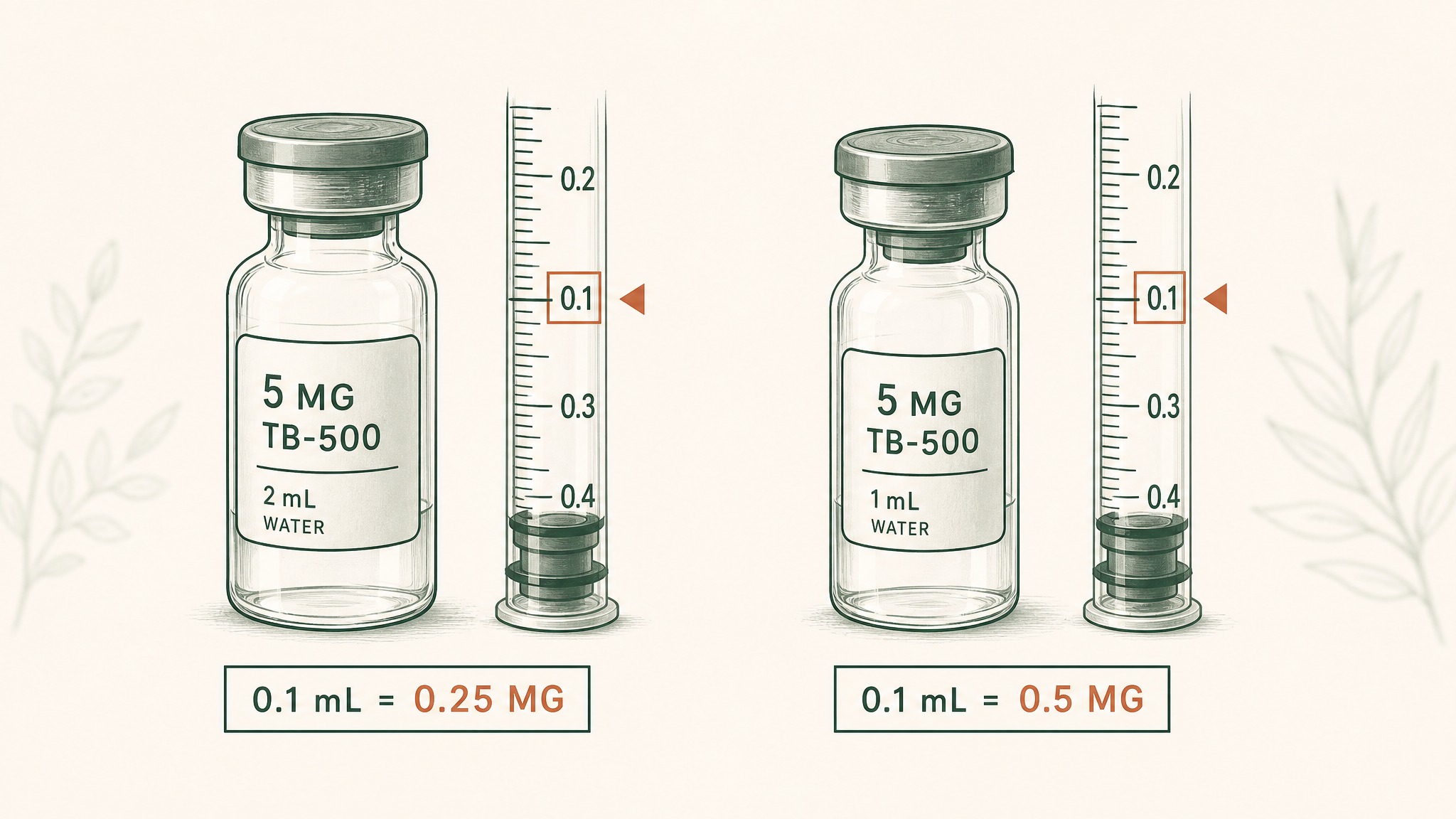
How vial concentration changes the smallest dose you can accurately measure from a syringe.
The last one is underrated. If you've reconstituted a 5 mg vial in 2 mL of bacteriostatic water (a common ratio), each 0.1 mL on the syringe carries 0.25 mg of peptide. That's the smallest dose you can reliably measure. Drop to a 5 mg vial in 1 mL and your minimum-precision dose doubles. Practical research dosing is constrained by what you can accurately draw, not just what the calculation suggests.
Most published research protocols converge in a per-dose range of 2 to 5 mg for an 80 kg adult. Going below 2 mg starts running into measurement-precision issues. Going above 5 mg starts running into the upper bound of the HED translation. The window is narrower than it looks.
What are the most common TB-500 single-dose calculation mistakes?
Three mistakes show up over and over in research community discussions:
- Confusing mcg and mg. A "100 dose" in a protocol that mostly uses mcg is 0.1 mg. A "100 dose" in a protocol that uses mg is a 1,000-fold higher dose. Read the unit, not just the number.
- Treating weekly total as single dose. A "5 mg per week" protocol on a twice-weekly schedule means 2.5 mg per administration, not 5 mg per administration. The unit on the label is the cumulative weekly figure, not the per-shot figure.
- Ignoring route when comparing doses. Users report dramatically different responses to "the same dose" because the route changes what arrives at the tissue. A 2 mg subcutaneous dose and a 2 mg oral capsule are not the same dose in any meaningful sense.
A fourth, quieter one: copying mg/kg numbers from rodent papers without running the HED translation. A "1 mg/kg rat dose" is not 80 mg for an 80 kg human; it's roughly 13 mg after the 6.2-factor correction, and most researchers wouldn't go anywhere near that. Skipping the translation step turns a calibrated calculation into a guess.
Where does delivery method fit in the dose conversation?
The unspoken assumption in most TB-500 single-dose discussions is that you're administering subcutaneously. That's how most published protocols translate. If you're not, the math has to shift.
Sublingual delivery is the under-discussed alternative. The peptide is held under the tongue, absorbed through the mucosal tissue, and lands in systemic circulation without passing through the digestive tract or the liver's first-pass metabolism. Done properly, the absorbed fraction of a sublingual dose is closer to injection than to oral, which is what makes it a credible non-injection option for research protocols.
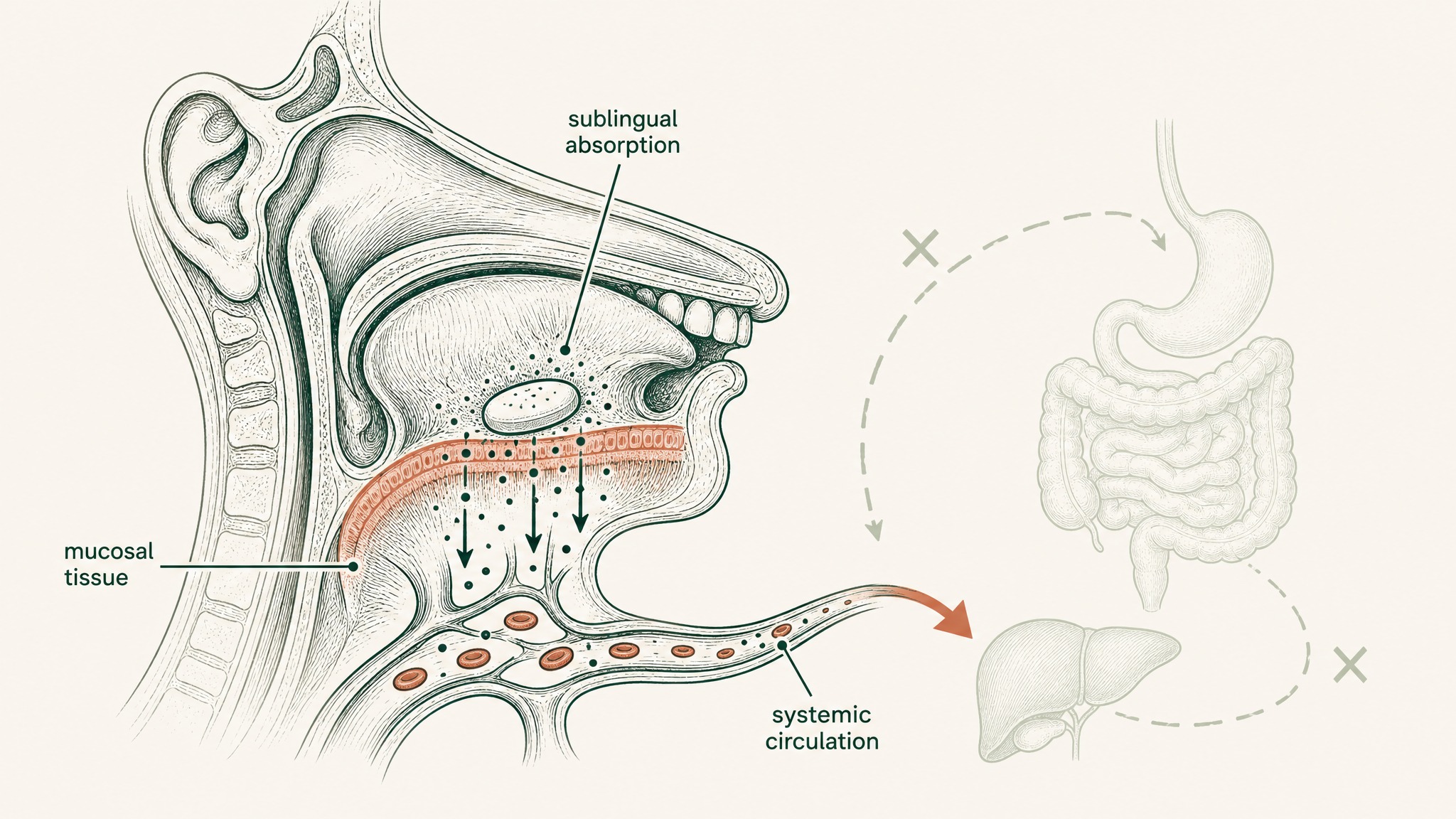
Sublingual delivery bypasses digestion and liver metabolism, sending peptides directly into the bloodstream.
VERO's VERISORB delivery system was designed around this principle. Each lozenge holds a measured dose, the dissolution profile is consistent, and the absorbed fraction is high enough that the nominal dose and the effective dose stay tight. For researchers building protocols where calculation precision matters more than syringe-based maximums, sublingual is the option that keeps single-dose math honest.
The trade-off is the dose ceiling. A sublingual lozenge can only hold so much peptide before the tongue surface saturates, so the absolute maximum per-dose number is lower than injection. For research targets that need the top of the HED-translated range, injection is still the route. For everything inside the standard 2 to 5 mg per-administration window, sublingual is a clean choice.
References
- US Food and Drug Administration. Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/estimating-maximum-safe-starting-dose-initial-clinical-trials-therapeutics-adult-healthy-volunteers. Retrieved 2026-06-06.
- Reagan-Shaw S, Nihal M, Ahmad N. (2008). Dose translation between animal and human studies revisited. FASEB Journal. https://pubmed.ncbi.nlm.nih.gov/17942826/. Retrieved 2026-06-06.
- Goldstein AL, Hannappel E, Kleinman HK. (2005). Thymosin beta-4: actin-sequestering peptide with tissue-repair signalling properties in animal models. Trends in Molecular Medicine. https://pubmed.ncbi.nlm.nih.gov/16099219/. Retrieved 2026-06-06.
- Crockford D, Turjman N, Allan C, Angel J. (2010). Thymosin beta-4: structure, function, and current biological properties supporting future research applications. Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536467/. Retrieved 2026-06-06.
- Ruff D, Crockford D, Girardi G, Zhang Y. (2010). A randomised, placebo-controlled, single and multiple dose study of intravenous thymosin beta-4 in healthy volunteers. Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536472/. Retrieved 2026-06-06.
Ready to apply this in a properly delivered protocol? Explore the RESTORE protocol →
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.