
The top 10 longevity supplements ranked by human trial strength, delivery, and cost. Where peptides sit is the part most 2026 lists skip. Research purposes only.
Type "top 10 longevity supplements" into Google in 2026 and you'll get roughly the same fifteen names shuffled into a slightly different order on every page. The lists rarely tell you which ones have real human trials behind them, how much of the capsule your bloodstream actually sees, or which categories the ranking has quietly left out.
This ranked list, written for research purposes only, tries to fix all three. Each pick has a real study behind it, a note on delivery, and a plain-English reason it earned its spot. Where the data works only in a specific population, we say so. Where the trial evidence is thinner than the marketing, we say that too.
The quick version, before you scroll:
- Rank order below combines human trial strength, delivery method, and cost.
- Numbers 1 to 5 are the boring, cheap, well-supported layer. Start there.
- Numbers 6 to 10 have interesting mechanisms and early human data worth watching.
- Peptides are covered in their own section, because regulatory rules keep them off standard supplement lists, not the strength of the science.
- Delivery matters as much as dose. A great molecule swallowed as a capsule is often a mediocre intervention by the time it clears your liver.
VERO makes peptide protocols. We do not sell any of the 10 supplements below. Where a peptide-class link belongs, we say so plainly.
What actually makes a longevity supplement worth taking?
Before ranking anything, you need to know what "works" means. A pill is worth swallowing if three things line up: the mechanism makes biological sense, at least one properly run human trial has shown a benefit you'd notice, and the delivery method actually gets enough of the molecule into your bloodstream to matter.
Miss any one of those and you're paying for a story.
Why a supplement only works if it passes three critical tests: mechanism, delivery, and human proof.
- Mechanism. Does the compound touch something known to drive aging, like mitochondrial function, senescent cell load, or NAD+ decline?
- Human evidence. Not a mouse study. Not a cell culture experiment. A trial in humans, ideally randomised, with a meaningful endpoint.
- Delivery. How much of the label dose survives your stomach, gut wall, and liver on the way to your cells?
If a supplement can't clear all three bars, it belongs on your "watching" list, not your "taking" list.
We also give bonus weight to cost and safety. A cheap molecule with a decades-long safety record and consistent evidence usually beats an expensive newcomer with a single positive trial, even if the newcomer sounds more exciting.
How did we rank the top 10?
Every pick was scored across four dimensions on a 0 to 3 scale, then ordered by total score. Ties broken by cost and safety record.
- Human trial strength. RCT with a real endpoint scores 3. Small pilot or observational-only scores 1. Mechanism-only scores 0.
- Delivery efficiency. Route delivers most of the dose to systemic circulation scores 3. Most gets destroyed by first-pass metabolism scores 0.
- Safety record. Multi-decade record with well-mapped side-effect profile scores 3. Sparse safety data scores 0.
- Cost per month at effective dose. Under $20 scores 3. Over $100 scores 0.
Dr Goel's note. In the protocol design work we've done at Peak Human Labs over the last decade, the pattern that keeps repeating is that people fixate on the newest, most-marketed compound and skip the four or five cheap ones with the strongest data. When we rebuild a stack around evidence and delivery first, most clients cut their supplement bill and feel better inside a month. That's what the ranking below is trying to reflect.
The top 10 longevity supplements for 2026
Here is the ranked list. If you're new to this and just want a shortlist, take the top five.
1. Omega-3 (EPA and DHA)
Omega-3 fatty acids sit at number one because the strongest cardiovascular endpoint in the entire supplement world belongs to them.
In the REDUCE-IT trial published in the New England Journal of Medicine in 2019, over 8,000 high-risk patients received either 2 g of icosapent ethyl twice daily or placebo. The primary cardiovascular endpoint dropped by around 25% versus placebo. That's a bigger effect than most longevity molecules will ever manage.
- Dose target: 2 g combined EPA + DHA per day.
- Delivery: standard soft-gels are fine, third-party tested products preferred.
- Watch-outs: high doses can thin blood, so co-ordinate with any anticoagulant.
2. Creatine monohydrate
Creatine is the cheapest, best-studied molecule on the list. It's also one of the very few compounds with both a muscle case and a brain case behind it.
Avgerinos and colleagues reviewed six RCTs of creatine in healthy adults in 2018 and found consistent signals for short-term memory and reasoning. On the muscle side, the evidence is old, uncontroversial, and directly relevant to longevity: sarcopenia (age-related muscle loss) is one of the strongest predictors of mortality in older adults, and creatine pushes against it.
Take 3 to 5 g of plain monohydrate powder in water, once a day, indefinitely. Fancy forms cost more and do not out-perform monohydrate.
3. Vitamin D3 (paired with K2)
Vitamin D3 makes the list on the strength of deficiency correction, not on the strength of extra supplementation on top of an adequate level.
The VITAL trial (Manson et al., NEJM 2019) randomised almost 26,000 adults to 2,000 IU of vitamin D or placebo for a median of over five years. The two primary endpoints (cancer and major cardiovascular events) did not significantly improve, though several secondary endpoints hinted at signals worth watching.
The honest read: correct a deficiency and you'll feel it. Pile more on top of an already adequate blood level and you probably won't.
Get a blood level, target 30 to 50 ng/mL, pair with K2 if you're supplementing long-term, and stop expecting miracles.
4. Magnesium (glycinate or threonate)
Magnesium is the quietly-good option most stacks are missing. It's hard to make it sound exciting because the evidence is just consistently reasonable across sleep, blood pressure, migraines, and general metabolic health.
A 2020 umbrella review by Veronese and colleagues pulled together 16 meta-analyses across 55 different health outcomes and found strong evidence for magnesium's role in several endpoints. Sleep and blood-pressure signals are softer but consistent enough that most clinicians recommend it.
- Glycinate is easiest on the gut and best for sleep.
- Threonate has the cleanest brain-penetration data.
- Practical dose: 200 to 400 mg of elemental magnesium in the evening.
5. NAD+ precursors (NMN and NR)
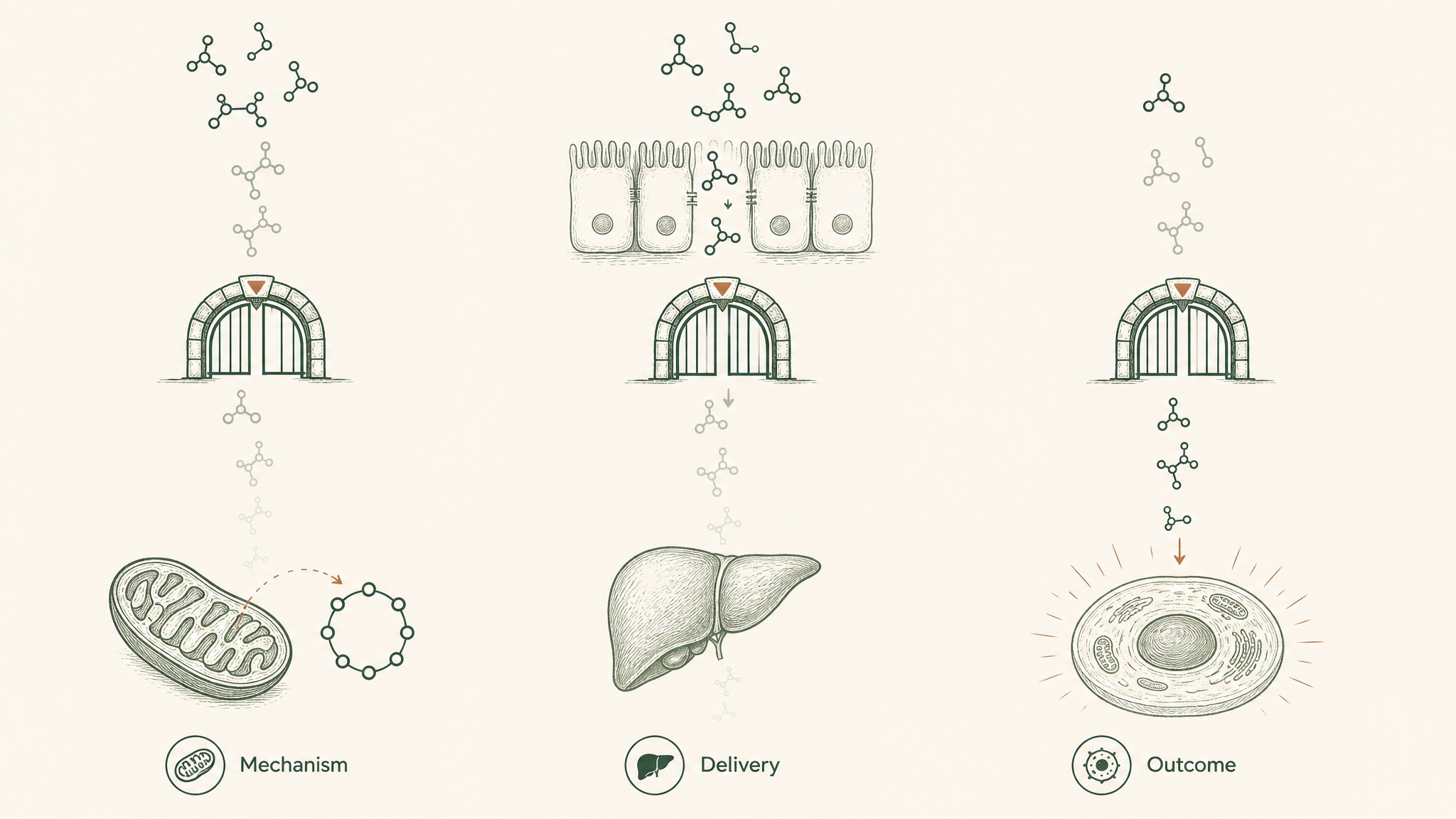
NAD+ is a cofactor your cells use to convert food into usable energy. Levels fall as you age. NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are precursors your body can convert into NAD+.
The most-cited human trial is Yoshino 2021 in Science, which gave 250 mg of NMN orally for ten weeks to postmenopausal women with prediabetes and measured improved muscle insulin sensitivity versus placebo. That's a real RCT in humans, not a mouse study. It's also one trial, in one population, on one endpoint.
Where it gets interesting is delivery. Oral NAD+ precursors have to survive your gut and liver before they can bump NAD+ inside your cells. Sublingual and injectable routes bypass that gauntlet entirely, which is why the LEGACY protocol is built around sublingual delivery via VERISORB: getting more of the signal into circulation without the first-pass tax.
6. GlyNAC (glycine plus N-acetylcysteine)
GlyNAC is the newest entry on this list and one of the most interesting for anyone over 55.
The Kumar 2021 pilot trial in Clinical and Translational Medicine gave older adults a combined glycine and NAC supplement for 24 weeks and tracked oxidative stress markers, mitochondrial function, insulin resistance, strength, and cognition. The trial reported improvements across almost every hallmark of aging it looked at, though sample size was small and follow-up trials are ongoing.
- Typical protocol: 3 g glycine + 3 g NAC (n-acetylcysteine), split morning and evening.
- Both are cheap, generic, and have decades of safety data individually.
- Combined data is early. Users report better recovery and sleep quality.
7. CoQ10 (ubiquinol)
CoQ10 is a mitochondrial cofactor that declines with age and is depleted further by statin use. It sits mid-list because the human trial evidence is decent for specific populations (statin users, heart failure) but softer for healthy-adult longevity.
Q-SYMBIO in 2014 randomised heart failure patients to CoQ10 or placebo and reported reduced major cardiovascular events over two years. It's a specific population, but the signal is consistent enough that most cardiologists no longer object to CoQ10 in that context.
Ubiquinol (the reduced form) is worth the small premium once you're past 40, when your conversion of ubiquinone to ubiquinol slows. Typical dose: 100 to 200 mg per day with a fatty meal.
8. Spermidine
Spermidine is the compound most tightly linked to autophagy, the cellular recycling process that clears out damaged proteins and organelles. Autophagy sits at the centre of several Hallmarks of Aging.
Eisenberg's 2016 paper in Nature Medicine reported extended lifespan in mice given dietary spermidine and observed that higher dietary intake in humans correlated with lower blood pressure and cardiovascular disease incidence. That's a mix of RCT-strength mouse work and observational human data, so we'd class the human evidence as promising rather than settled.
- Food sources (wheat germ, aged cheese, mushrooms) work too.
- Typical supplement dose: 1 to 5 mg per day.
- Watch for follow-up human trials on cognitive endpoints.
9. Urolithin A
Urolithin A is what your gut bacteria produce when they metabolise the ellagitannins in pomegranates, walnuts, and berries. About a third of adults can't produce it efficiently on their own, which is where supplementation comes in.
Andreux 2019 in Nature Metabolism gave healthy older adults either 500 mg or 1,000 mg of urolithin A for four weeks and found the compound was safe and modulated mitochondrial gene expression in muscle. A follow-up trial reported improved muscle endurance.
At current retail prices, urolithin A is one of the most expensive picks on this list. It earns its spot on mechanism and early human data, but the cost score is what keeps it out of the top five.
10. Fisetin
Fisetin is a plant polyphenol most heavily marketed as a senolytic, meaning a compound that helps clear senescent (aged, non-dividing) cells that accumulate with age and drive chronic inflammation.
The animal work is genuinely interesting. Yousefzadeh 2018 in EBioMedicine reported that fisetin cleared senescent cells and extended healthspan in aged mice. Human trials are underway but the human endpoint evidence is not yet where the mouse evidence sits.
Most clinical fisetin protocols follow a pulsed schedule (a large dose for two consecutive days per month) rather than daily dosing. Users report that pulsed protocols feel easier on the wallet and easier on the gut.
Why aren't peptides on most top 10 lists?
Because they're not classified as supplements. That's the honest answer.
Compounds like BPC-157, GHK-Cu, MOTS-c, and Epithalon aren't sitting in supplement lists for a regulatory reason, not because the science is thinner. Most of them can't be sold over-the-counter as a supplement in the US or UK, so mainstream lists don't feature them.
The research picture on the peptide side is genuinely interesting:
- GHK-Cu has been observed in cell studies to modulate gene expression relevant to skin, wound, and connective-tissue biology.
- MOTS-c is a mitochondrial-derived peptide observed in preclinical research to affect metabolic and exercise-related pathways in animal models.
- Epithalon has been studied in observational human cohorts for telomerase-related endpoints, though the trial base remains limited.
Every peptide claim in that list is preclinical or early human research, not clinical prescribing evidence. Research suggests the mechanisms are worth watching. Users report varied protocols in the research setting.
Peptides are the category the standard top-10 lists refuse to acknowledge exist. Whether they belong in your own thinking depends on how you weight regulatory classification versus mechanism plausibility.
For the tissue-repair side of the peptide conversation, see our overview of the RESTORE protocol. For the longevity-signalling side, see LEGACY.
Which of these actually reach your bloodstream?
Here's the delivery question most supplement lists skip. A capsule label is the dose that went into the capsule. It is not the dose your cells will see.
Every swallowed molecule has to survive three filters:
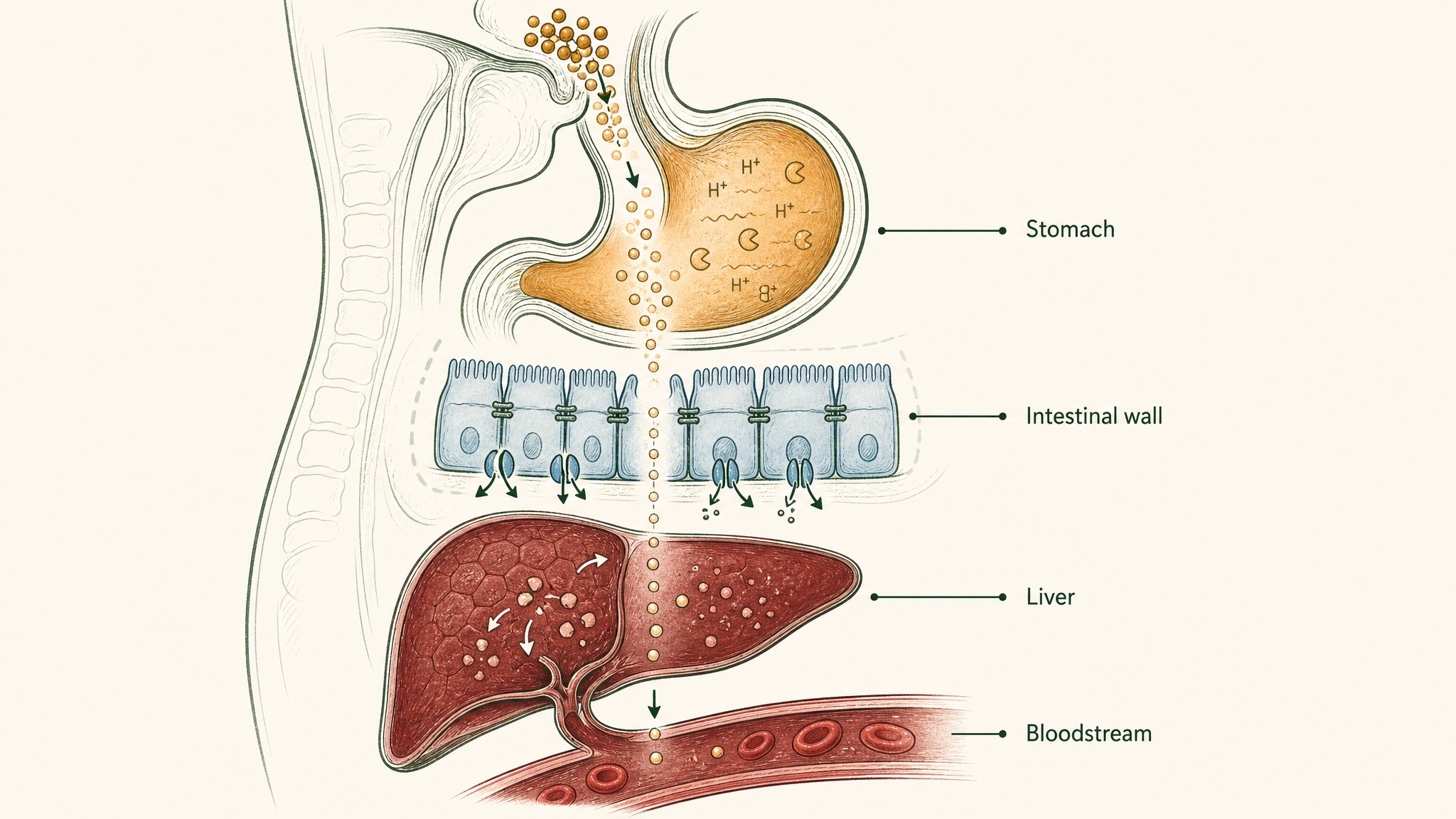
How stomach acid, intestinal barriers, and liver metabolism reduce oral supplement dose before it reaches your blood.
- Your stomach. Acid and pepsin destroy peptides and oxidise sensitive molecules.
- Your intestinal wall. Large or charged molecules struggle to cross, and many get pumped straight back out.
- Your liver. First-pass metabolism removes a chunk of whatever survives before it ever reaches general circulation.
By the time a 1,000 mg oral dose has run that gauntlet, the amount your tissues actually see can be a tenth or less of what the label promised.
| Delivery route | Typical bioavailability | Onset | Where you'll see it |
|---|---|---|---|
| Standard oral capsule | Low, often under 20% for peptide-class molecules | 45 to 90 min | 95% of supplement bottles |
| Liposomal capsule | Low to moderate | 30 to 60 min | Marketed as "enhanced" oral |
| Sublingual | High for small molecules | 5 to 15 min | NAD+, glutathione, B12 |
| Injectable | Effectively 100% | Minutes | Reference standard for research peptides |
The molecules on this top 10 vary wildly in how well they clear this filter. Omega-3, creatine, vitamin D, and magnesium survive oral delivery well. NAD+ precursors are the group where delivery route matters most, and where the sublingual and injectable debates have real substance behind them. For a deeper look at that specific problem, see our companion piece on supplements for longevity.
What should a beginner longevity stack actually look like?
If you took nothing from this article except the shortlist, we'd want that shortlist to be honest.
For most adults, the boring, well-supported, cheap layer covers 80% of the meaningful signal:
- 2 g omega-3 (EPA + DHA) daily.
- 3 to 5 g creatine monohydrate daily.
- Vitamin D3 dosed to a target blood level of 30 to 50 ng/mL, paired with K2.
- 200 to 400 mg magnesium glycinate or threonate in the evening.
That's four supplements, well under $30 a month, and matches the strongest human data. Add NAD+ precursor, GlyNAC, or CoQ10 next, based on your age and blood work, not based on what a podcast promoted last week.
Members experience the biggest changes not from the shiniest new molecule but from finally taking the boring four consistently for three months. That's the pattern we see over and over again.
What are the biggest myths about longevity supplements?
Three keep showing up.
Myth 1: More expensive means more effective. Creatine, magnesium, and vitamin D3 are among the strongest-evidence picks and among the cheapest. Price tracks marketing budget more than mechanism.
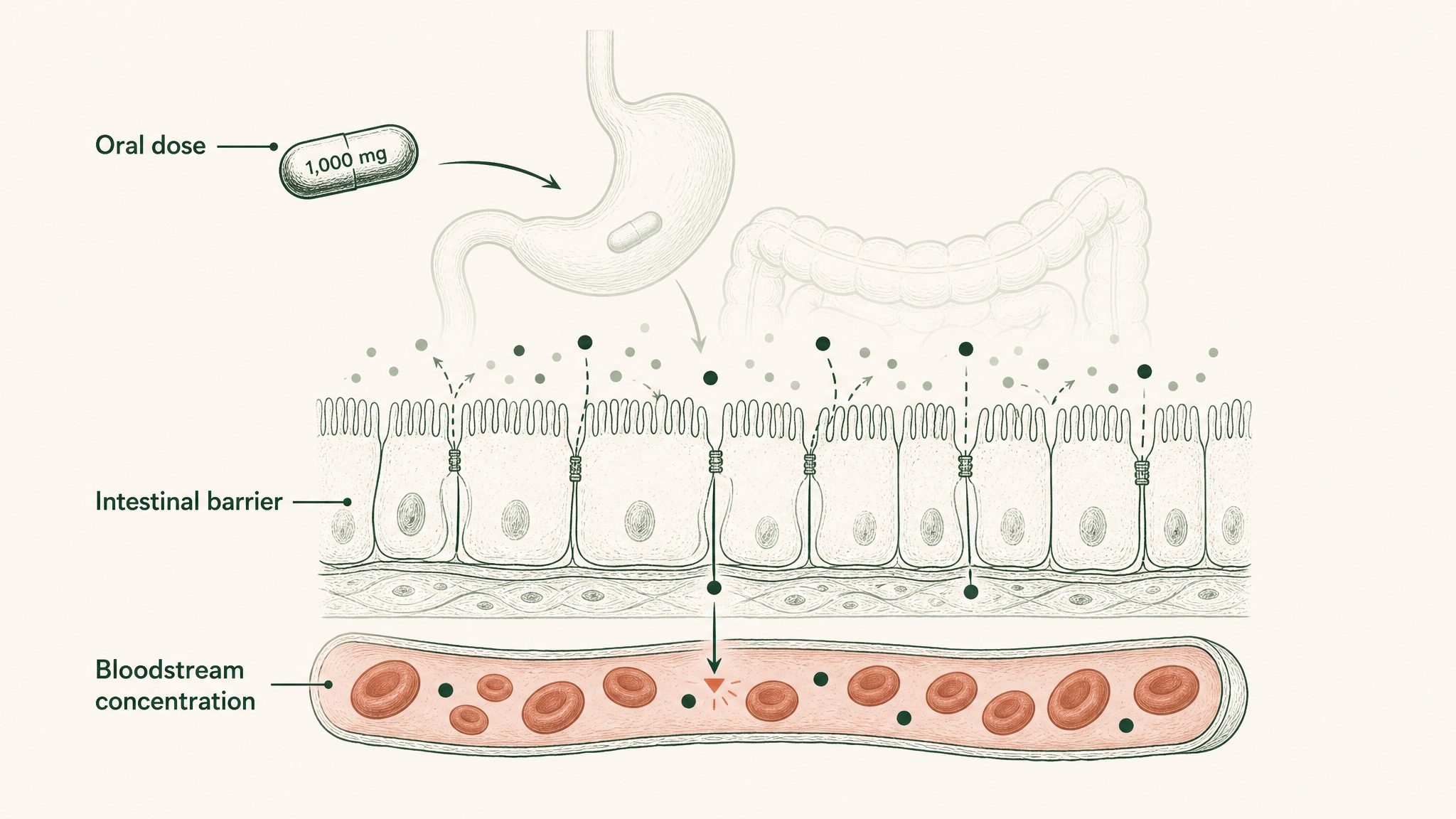
Only a fraction of an oral supplement's labeled dose actually enters your bloodstream.
Myth 2: Label dose equals cell dose. Every capsule that says 1,000 mg is a capsule that contains 1,000 mg. What reaches your bloodstream is a completely separate question, and for many molecules it's a small fraction.
Myth 3: Peptides are a fringe rabbit hole. They're a regulated category, which is different from a fringe one. The preclinical and early clinical research on several peptide-class compounds is stronger than the human evidence behind several of the polyphenols in the top 10.
Frequently asked questions
What is the single most effective longevity supplement in 2026?
Omega-3 (EPA + DHA at around 2 g per day) has the strongest cardiovascular endpoint data of any longevity-relevant supplement. That doesn't make it a fix-everything answer; it makes it the pick with the cleanest human trial behind it.
Should I take NMN or NR for NAD+?
Both raise blood NAD+ metabolites in trials. NMN has the higher-profile insulin sensitivity trial; NR has the longer commercial safety record. Delivery route may matter more than which precursor you pick, especially past age 45.
Is rapamycin a longevity supplement?
No, it's a prescription drug. It appears on some influencer lists but it's not sold as a supplement and shouldn't be lumped in with over-the-counter picks in this ranking.
Are peptides safer than supplements?
They're a different regulatory category, so a like-for-like comparison isn't clean. Research peptides are usually dosed under research protocols, not self-experimentation, and the safety data varies compound by compound. This article and VERO's protocol content are for research purposes only.
How long before I feel a difference?
Magnesium and creatine tend to show subjective changes inside a fortnight. Omega-3 and vitamin D correction take longer, often 8 to 12 weeks. NAD+ precursors vary hugely by individual and by delivery route.
Key Takeaways
- The top 10 longevity supplements combine mechanism, human trial strength, and delivery efficiency; ignore any one of those and you're buying a story.
- Numbers 1 to 5 (omega-3, creatine, vitamin D3, magnesium, NAD+ precursors) cover most of the meaningful signal at under $30 a month.
- Numbers 6 to 10 (GlyNAC, CoQ10, spermidine, urolithin A, fisetin) have interesting mechanisms and early human data; consider them watch-list additions, not foundations.
- Delivery matters as much as dose. Oral capsules under-perform on peptide-class molecules; sublingual and injectable routes exist for a reason.
- Peptide-class compounds sit outside the standard top 10 lists for regulatory reasons, not because the mechanism work is thinner. VERO's protocol pages cover the science in detail.
References
- Bhatt et al. (2019). Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMoa1812792. Retrieved 2026-07-03.
- Yoshino et al. (2021). NMN and insulin sensitivity in postmenopausal women with prediabetes. Science. https://www.science.org/doi/10.1126/science.abe9985. Retrieved 2026-07-03.
- Manson et al. (2019). Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease (VITAL). New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMoa1809944. Retrieved 2026-07-03.
- Avgerinos et al. (2018). Creatine supplementation and cognitive function in healthy individuals: a systematic review. Experimental Gerontology. https://pubmed.ncbi.nlm.nih.gov/29704637/. Retrieved 2026-07-03.
- Eisenberg et al. (2016). Cardioprotection and lifespan extension by spermidine in mice, and dietary intake correlations in humans. Nature Medicine. https://pubmed.ncbi.nlm.nih.gov/27841876/. Retrieved 2026-07-03.
- Andreux et al. (2019). Urolithin A safety and mitochondrial gene expression in older adults. Nature Metabolism. https://www.nature.com/articles/s42255-019-0073-4. Retrieved 2026-07-03.
- Kumar et al. (2021). GlyNAC supplementation in older adults: hallmarks of aging pilot trial. Clinical and Translational Medicine. https://pubmed.ncbi.nlm.nih.gov/33783984/. Retrieved 2026-07-03.
- Yousefzadeh et al. (2018). Fisetin as a senotherapeutic candidate in aged mice. EBioMedicine. https://pubmed.ncbi.nlm.nih.gov/30279143/. Retrieved 2026-07-03.
- Veronese et al. (2020). Magnesium and health outcomes umbrella review of meta-analyses. https://pubmed.ncbi.nlm.nih.gov/33260096/. Retrieved 2026-07-03.
- Mortensen et al. (2014). CoQ10 in heart failure (Q-SYMBIO trial). JACC Heart Failure. https://pubmed.ncbi.nlm.nih.gov/25282031/. Retrieved 2026-07-03.
Curious how the VERO protocol side of the longevity conversation lines up with the supplement side above? Start with the LEGACY protocol for the aging-signal work, or explore every VERO protocol to see where each peptide fits.
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.