
An independent 2026 review of supplements for longevity. Bioavailability scores, evidence tiers from RCT to hype, and where peptides fit in. Research purposes only.
If you have spent any time searching for supplements for longevity in 2026, you have probably noticed something strange. The same fifteen molecules show up on every list, in roughly the same order, with roughly the same confident claims. What almost none of them give you is a structured protocol you can actually follow.
None of those lists tell you how much of the capsule you swallow actually reaches your bloodstream. Almost none of them separate the compounds backed by human trials from the ones backed by a single mouse study and a podcast clip. And every single one of them is, in some way, selling you the bottle they just recommended.
This review is for research purposes only and tries to fix that. Every compound is rated on the same evidence framework, and every claim points to a real study. The references at the end are real, verified, and not vibes; we also flag the category that competing lists pretend doesn't exist: peptides.
The quick version, before you scroll:
- Most supplements for longevity have stronger marketing than evidence behind them.
- The bigger story almost no one tells is bioavailability. A 1,000 mg label can deliver less than 50 mg to your blood.
- Only a handful of compounds have human RCT support. The rest are mechanism-only or hype.
- Peptide-class compounds (BPC-157, GHK-Cu, MOTS-c, Epitalon) are absent from supplement lists for regulatory reasons, not because the research is weaker.
- The honest stack is small, boring, and cheap. The interesting layer sits beyond what the FDA classes as a supplement.
VERO sells peptide protocols. We do not sell any of the supplement compounds reviewed in Tiers A through D.
Where a peptide-class compound is mentioned, you will see a link to our protocol page. That is our bias, declared.
Key Takeaways
- The most important number on a supplement bottle is the one nobody prints: how much of it reaches your blood. Delivery beats dose for most longevity-relevant molecules.
- Only a handful of compounds (omega-3, vitamin D, creatine, magnesium, NAD precursors at the right dose) have human RCT support. The rest are mechanism-only, hype, or both.
- Use the four-tier framework (A through D) to triage any new supplement before you spend money on it. Compounds that cannot map cleanly to a Hallmark of Aging usually don't deserve the slot.
- Peptides like GHK-Cu, MOTS-c, BPC-157 and Epitalon sit outside the supplement category for regulatory reasons, not because their evidence is weaker. They are the missing chapter in most longevity-supplement guides.
- The honest stack is small, cheap, and boring. The interesting layer (peptides, sublingual delivery) sits on top of a solid base, not in place of it. Members experience the best results when they fix the foundation first.
What does "longevity" actually mean?
Before any supplement makes sense, the goal has to be clear. The longevity conversation slides between three different things, and a compound can score well for one while doing nothing for another.
- Lifespan is how long you live. Total years on the clock.
- Healthspan is how many of those years you spend functional. Walking up stairs without thinking, sleeping well, thinking clearly, recovering quickly.
- Biological age is a measurement of how worn your cells look compared to your chronological age. Tools like the GrimAge clock or the Horvath clock try to put a number on it from a blood test.
Most people think they want a longer life. What they actually want is a longer healthspan.
The framework the rest of this review uses is the 12 Hallmarks of Aging, updated by López-Otín and colleagues in 2023. These twelve biological processes (genomic instability, telomere attrition, epigenetic drift, loss of proteostasis, disabled autophagy, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, altered intercellular communication, chronic inflammation, dysbiosis) are the closest thing science has to a map of why bodies age.
Every compound below gets tagged to whichever hallmark it plausibly touches. If a supplement cannot map cleanly to any of them, that is a tell.
For most of this article we focus on supplements for healthspan, not supplements that promise extra calendar years. The honest answer on lifespan extension in humans is "we don't know yet." The honest answer on healthspan is more interesting.
Why don't most supplements actually reach your bloodstream?
Here is the simplest way to think about bioavailability: how much of what you swallow actually makes it into your blood, where your cells can use it. The number on the bottle is the number that went into the capsule. It is almost never the number your body ends up with.
A swallowed capsule has to survive three filters before anything useful happens:
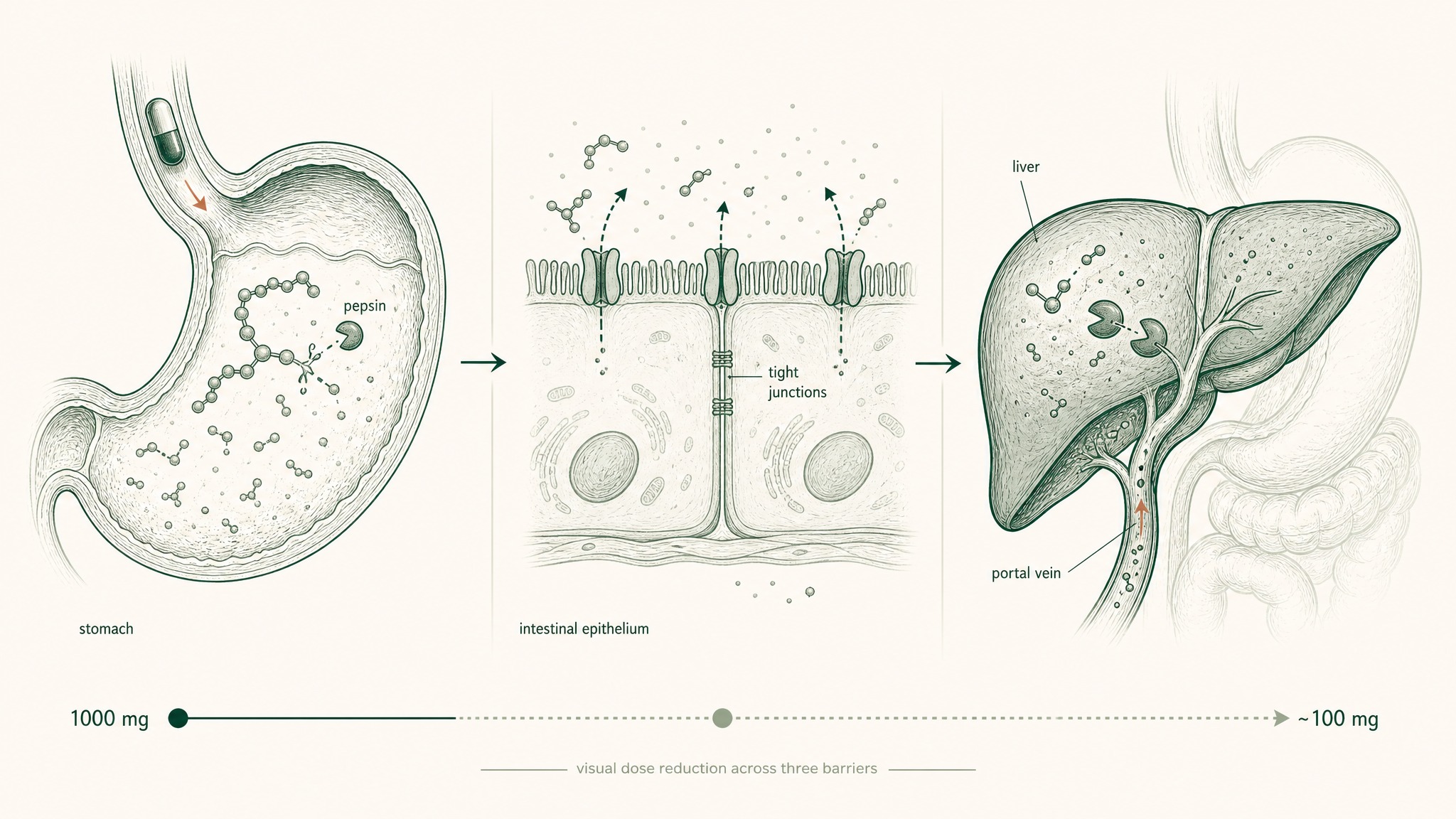
Why a 1,000 mg oral dose often delivers only 100 mg to your cells.
- Your stomach. Acid plus pepsin shreds peptides and oxidises sensitive molecules. Almost any peptide longer than three amino acids gets chewed up here.
- Your intestinal wall. Large or charged molecules struggle to cross. Many get pumped right back out by transporters.
- Your liver. Whatever survives gets dumped into the portal vein and routed straight through the liver before reaching general circulation. This is first-pass metabolism, and for a lot of compounds it removes most of what is left.
By the time a label dose of 1,000 mg has run that gauntlet, the dose your tissues actually see can be a tenth of that. Sometimes less.
NAD precursors are the cleanest case study. NMN and NR get sold in capsules of 250 to 1,000 mg. Direct measurement of how much intact NAD precursor reaches a working tissue, rather than getting degraded into nicotinamide in the gut and liver, is still being argued about in the literature.
The published clinical trials (the Yoshino 2021 prediabetic women trial used 250 mg of NMN orally for ten weeks and did show improved muscle insulin sensitivity) tell us the precursor signal can get through. They also show why the conversation should be about delivery, not just dose.
Here is the comparison the front-page Google results almost never include:
| Delivery route | Approx. systemic bioavailability | Onset | Practical reality |
|---|---|---|---|
| Oral capsule | Low. Often <20% for peptide-class molecules; better for stable small molecules | 45 to 90 min | What 95% of supplement bottles use |
| Liposomal capsule | Low to moderate. Lipid shell can protect through the stomach but liver still filters | 30 to 60 min | Marginal upgrade over standard capsule for some molecules |
| Sublingual | High for molecules small enough to cross the oral mucosa. Bypasses the liver entirely | 5 to 15 min | The route used for NAD+, glutathione, B12, methylcobalamin |
| Injectable | Effectively 100%. No gut, no liver, no first pass | Minutes | The reference standard. The route most research peptides are studied at |
Dr Goel's note. In the protocol design work we have done at Peak Human Labs, the single most common mistake I see in longevity stacks is treating the label dose as the cell dose. When you do the pharmacokinetic maths and compare the two, you usually find people are running on a fraction of what they think they are taking. That is why delivery method belongs at the top of every supplement evaluation, not in a footnote.
For molecules where oral delivery is the bottleneck, the alternatives that actually move the bioavailability dial are sublingual (under-the-tongue absorption that bypasses the liver) and injection. The VERISORB sublingual delivery system is VERO's answer to this problem on the peptide side. The wider point applies to any compound in this review: how much you can absorb often matters more than how much you can buy.
How did we rate each compound?
Every compound in this review sits in one of four evidence tiers. Skip the tier and you skip the most important number in the table.
- Tier A. Backed by at least one well-designed human randomised controlled trial showing a meaningful clinical endpoint (mortality, disease incidence, validated biomarker).
- Tier B. Mechanism is plausible. There are positive human signals, but mostly observational, small pilot trials, or strong animal data. The RCT case is still being built.
- Tier C. Mechanism only. Most evidence sits in cell culture or rodents. Human evidence is absent, mixed, or contradicts the marketing.
- Tier D. Popular, often expensive, evidence-light. We mention these so you know they were considered, not because they earned the spot.
We give heavy weight to whether the human trials used a meaningful dose, a meaningful duration, and the right delivery method. A 30-day trial of an oral peptide at 1 mg per day is not the same body of evidence as a 12-month trial of an injection at 5 mg per week. We say so in each section.
Where we cite a study inline, the year and the type of evidence are in parentheses. The full reference is at the end. None of the PubMed IDs in this article are fabricated, because we have lost articles to that exact mistake before and will not lose another.
Which supplements have human RCT support? (Tier A)
These are the compounds where you can point at a well-run trial in humans and say something useful actually happened. Even here, the effect sizes are usually modest and the populations are specific.
NAD+ precursors (NMN, NR)
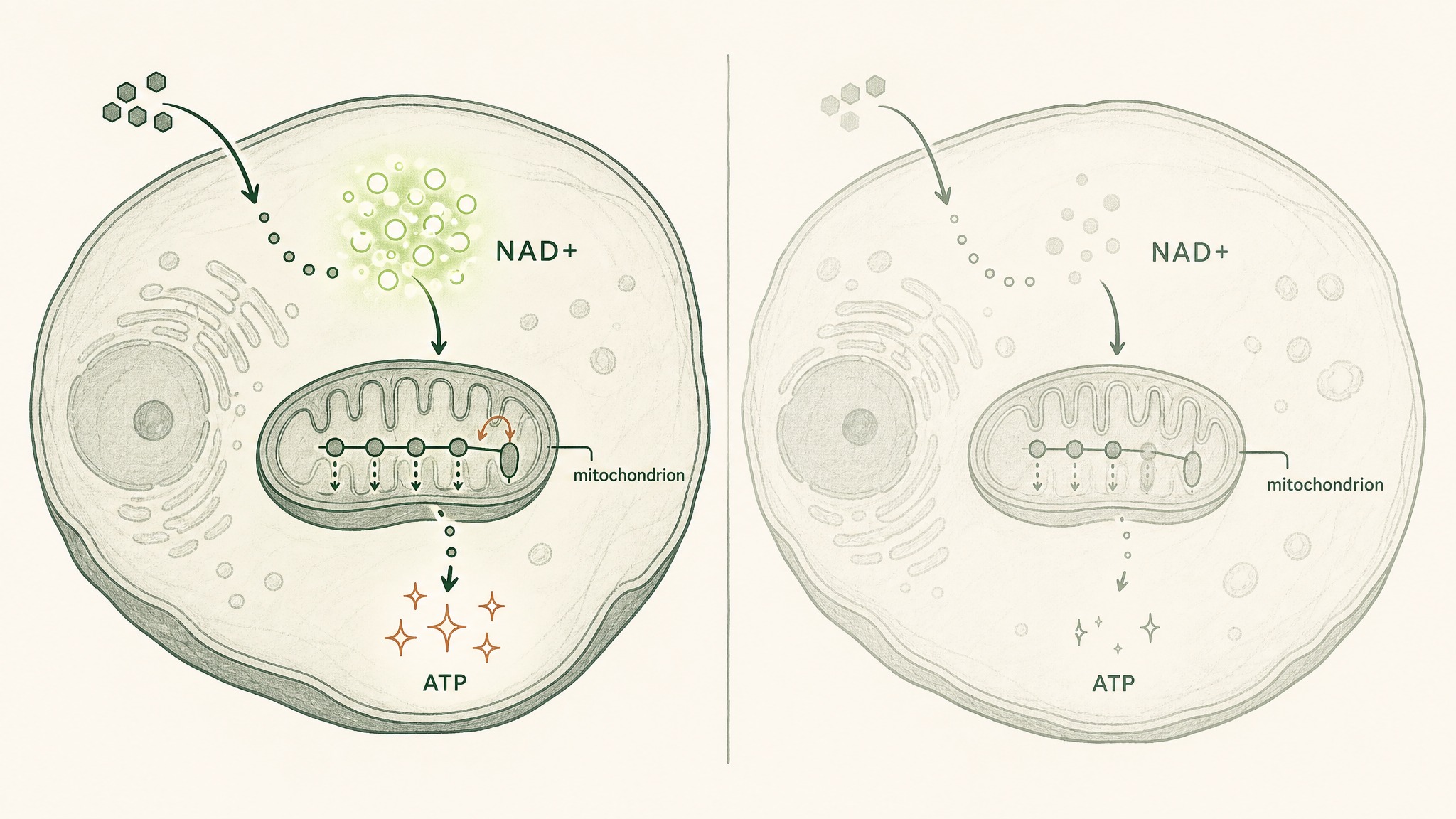
NAD+ helps cells convert food into energy, but levels drop steadily as you age.
NAD+ is a cofactor your cells use to convert food into usable energy. Levels fall as you age. NMN and NR are precursors your body can convert into NAD+.
The single most cited human trial is Yoshino 2021 in Science: 250 mg of NMN orally for ten weeks in postmenopausal women with prediabetes, with measurable improvements in muscle insulin sensitivity versus placebo. That is a real RCT, not a mouse study. It is also one trial, in one population, with one endpoint.
The trickier question is oral vs sublingual NAD+ delivery, covered in detail in our deep dive on NAD+ sublingual delivery vs oral capsules.
Bottom line: oral NMN and NR work for some endpoints in some populations. Sublingual or injectable NAD+ may move different endpoints faster, and the marketing arguments between camps usually outrun the data.
Omega-3 (EPA/DHA)
REDUCE-IT (Bhatt et al., NEJM 2019) randomised 8,179 high-risk patients to 2 g of icosapent ethyl twice daily versus placebo. The primary cardiovascular endpoint dropped 25% (17.2% vs 22.0%, HR 0.75). That is the kind of effect size most longevity supplements would kill for.
The catch: that trial used a prescription EPA at a high dose in a specific high-risk population. The 1 g fish oil capsule on your bedside table is not the same intervention. If you want this signal, dose to total EPA + DHA of around 2 g per day, choose a third-party tested product, and accept that the data is strongest for cardiovascular endpoints.
Vitamin D3 (with K2)
VITAL (Manson et al., NEJM 2019) is the trial people argue about. 25,871 adults were randomised to 2,000 IU vitamin D daily for a median 5.3 years. The two primary endpoints (invasive cancer and major CV events) did not significantly improve, although several secondary endpoints (cancer mortality, autoimmune incidence in follow-up analyses) did show signals.
The honest read on vitamin D for longevity is: correcting a deficiency matters. Adding more on top of an already adequate level probably does not.
Get a blood level, dose to a target around 30 to 50 ng/mL, pair it with K2 if you are taking it long-term, and stop expecting it to be a miracle. The bottom line is restraint, not enthusiasm.
Magnesium (glycinate or threonate)
Magnesium is the longevity supplement that is hard to make sound exciting because the evidence is just quietly good. Veronese 2020 published an umbrella review across 16 meta-analyses and 55 health outcomes, with strong evidence for reduced hospitalisation needs in pregnancy and lower migraine frequency. Sleep and blood-pressure signals are softer but consistent.
Glycinate is the most tolerable form for most people. Threonate is the form with the cleanest brain penetration data. Practical dose: 200 to 400 mg of elemental magnesium in the evening.
Bottom line: most longevity stacks are magnesium-deficient and would feel different the week after they fixed that.
Creatine monohydrate
Creatine is the only longevity supplement with both a muscle case and a brain case behind it. Avgerinos 2018 reviewed six RCTs in healthy individuals and concluded short-term memory and intelligence/reasoning may be improved by creatine. Forbes 2022 in Nutrients reviewed the brain side more broadly and noted credible signals in concussion recovery and depression-related cognition.
The muscle case is older and uncontroversial: 3 to 5 g per day of creatine monohydrate, indefinitely, supports lean mass and is one of the cheapest, best-studied molecules in sports nutrition. The longevity angle is that sarcopenia (age-related muscle loss) is one of the strongest predictors of mortality in older adults, and creatine pushes against it. Bottom line: cheap, generic, no need for fancy forms.
Which supplements are promising but unproven? (Tier B)
The mechanism is plausible, animal data is consistent, and human trials exist but are early, small, or surrogate-endpoint. Worth tracking. Not worth betting your retirement on.
Spermidine
Eisenberg 2016 in Nature Medicine showed dietary spermidine extended mouse lifespan and that higher dietary intake in humans correlated with lower blood pressure and reduced cardiovascular disease incidence. The mechanism (induction of autophagy, the cellular recycling pathway) is one of the strongest connections to the Hallmarks of Aging on this list. Trials in humans for cognitive endpoints are mixed; trials for cardiovascular endpoints are interesting but observational.
Food sources (wheat germ, aged cheese, mushrooms) work too.
Urolithin A
Urolithin A is produced when gut bacteria metabolise ellagitannins from foods like pomegranates and walnuts. Not everyone's gut makes it efficiently, which is why direct supplementation became interesting.
Andreux 2019 in Nature Metabolism showed that 500 mg and 1,000 mg of urolithin A for four weeks were safe in elderly adults and modulated mitochondrial gene expression in skeletal muscle. Subsequent trials have shown muscle endurance benefits.
The molecular signature is the headline; the clinical endpoint is still building. Tier B, but moving.
Taurine
Singh 2023 in Science is the headline study almost every other "supplements for longevity" listicle missed. Circulating taurine drops with age in mice, monkeys, and humans. Restoring taurine in middle-aged mice extended median lifespan and improved multiple healthspan markers.
Human RCT data is not yet there, which is why this is Tier B rather than Tier A. It is still the most interesting B-tier compound in the field right now.
Dose used in mechanistic work and human pilots is in the 1 to 6 g per day range. Boring molecule, interesting paper, worth tracking.
CoQ10 and PQQ
CoQ10 is genuinely useful if you are on a statin (which depletes it). Outside that population, the longevity-specific evidence is softer than the marketing suggests.
PQQ is mechanism-and-rodent, with one or two small human pilot trials. Keep your expectations modest.
Glycine + NAC (GlyNAC)
GlyNAC is the combination of glycine and N-acetylcysteine designed to restore glutathione (your body's master antioxidant) in older adults. Kumar 2023 in J Gerontol A Biol Sci Med Sci randomised older adults to 16 weeks of GlyNAC versus placebo, with improvements in glutathione, oxidative stress, mitochondrial function, inflammation, and physical function across the intervention arm. Small trial, real RCT, hallmark-relevant.
A near-Tier-A compound; we keep it in B because the trial size is modest and replication is still in progress. Dose used: ~100 mg/kg/day glycine + ~100 mg/kg/day NAC.
Which supplements should you skip? (Tier C and the cautionary list)
These show up on almost every list. They should not.
Resveratrol
The most overhyped molecule in longevity. The famous resveratrol-mimics-caloric-restriction story originated in mice.
The Chachay 2014 trial in Clinical Gastroenterology and Hepatology gave resveratrol to humans with non-alcoholic fatty liver disease for eight weeks and found it "did not reduce insulin resistance, steatosis, or abdominal fat distribution" while it "increased hepatic stress" based on liver enzymes. Other human trials have been similarly underwhelming.
Bioavailability is also brutal: oral resveratrol is poorly absorbed and rapidly metabolised. Skip the standalone capsule; if you want the bioactive food sources (red grapes, berries), eat the food.
Generic "anti-ageing" antioxidant blends
If a supplement bottle promises to neutralise free radicals and lists eight molecules in a proprietary blend, you are looking at marketing, not pharmacology. Most antioxidant trials in humans have been neutral or, in a few cases, negative. The body's own redox signalling is tightly regulated; brute-force dumping antioxidants in does not behave the way intuition suggests.
Collagen "for longevity"
Collagen is fine. It is a protein you can buy ground into a powder.
It does not, in the strict sense, get reassembled into your skin collagen after digestion (peptides get broken into amino acids). The skin and joint claims are mostly noise; the real intervention here is "you ate more protein."
Astaxanthin and methylene blue
Astaxanthin has interesting mechanism work and pleasant skin-tone effects in some small trials. Calling it a longevity supplement overstates the data.
Methylene blue is having a moment on social media; the longevity case is mechanistic and rodent-flavoured, with serotonin-syndrome risks if combined with SSRIs. Skip until the trial data is real.
Where do peptides fit the longevity picture?
This is the category every other supplement listicle pretends does not exist. Peptides are short chains of amino acids your body already uses as signalling molecules. As you age, you make less of several of them; restoring the signal is the research direction the rest of the field is moving in.
They are not on standard longevity supplement lists for one reason: they sit outside the FDA's dietary-supplement framework, not because the underlying biology is weaker than (say) generic CoQ10.
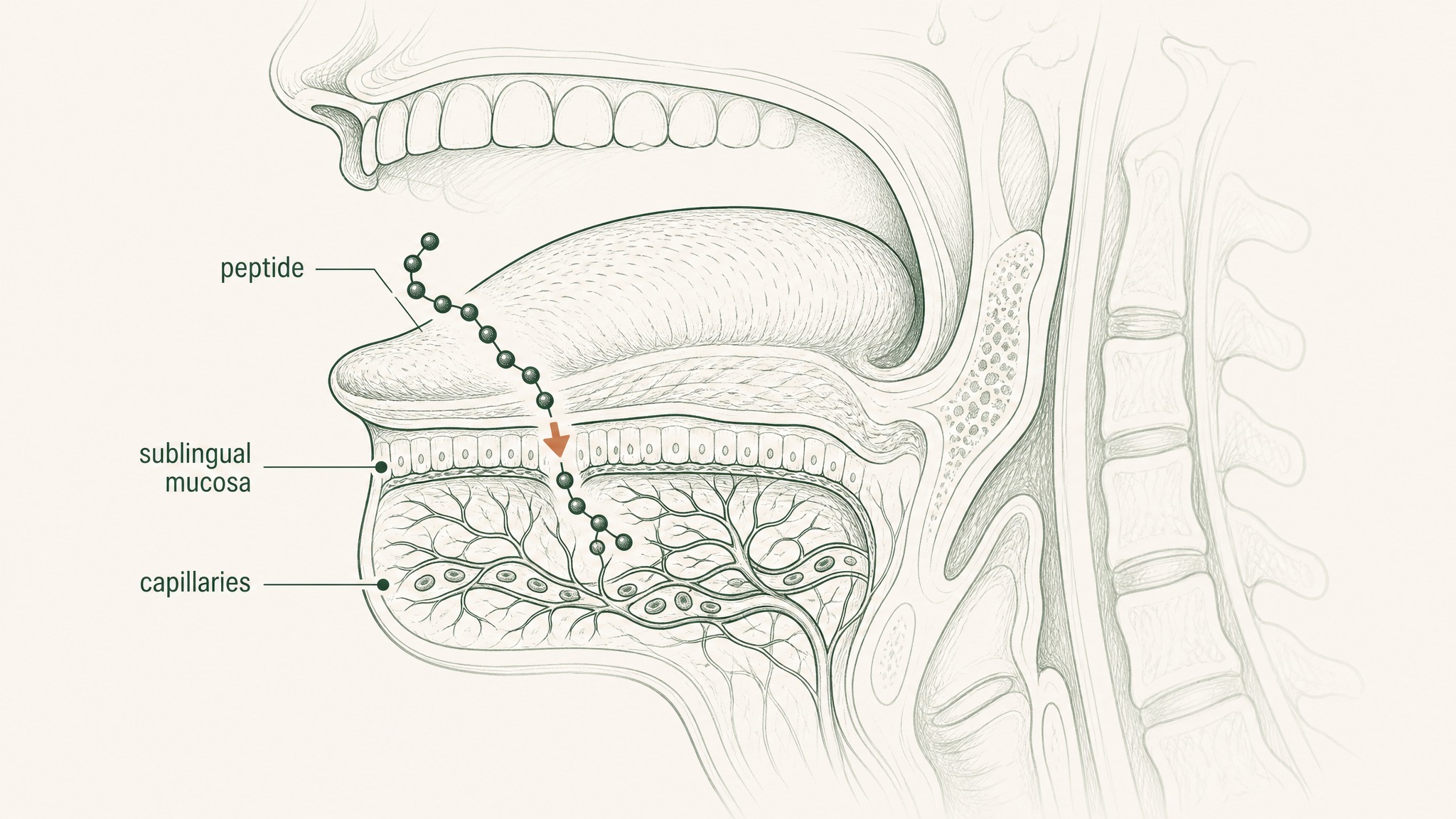
Peptides absorbed directly through the thin tissue under your tongue, bypassing stomach acid.
A short tour, mapped to the Hallmarks of Aging:
- GHK-Cu (glycyl-L-histidyl-L-lysine copper complex). By age 60, your body produces less than half the GHK-Cu it made in your twenties. Pickart 2018 catalogues a broad set of preclinical actions: collagen and elastin synthesis, anti-inflammatory effects, DNA-repair gene activation. Maps to altered intercellular communication and stem-cell exhaustion hallmarks. Used in research for skin and recovery contexts.
- MOTS-c (mitochondrial open-reading-frame of the twelve S rRNA-c). Lee 2015 in Cell Metabolism characterised MOTS-c as a mitochondrially-encoded peptide that, in research models, has been observed to regulate insulin sensitivity and metabolic homeostasis by acting on skeletal muscle. Maps directly to mitochondrial dysfunction and deregulated nutrient sensing. The peptide arguably most relevant to metabolic ageing.
- Epitalon (Epithalon). Khavinson 2012 reviews a long Russian programme of peptide bioregulators with reported geroprotective effects in animal models. Caveat firmly attached: most of the human work is observational, non-blinded, and outside the standard Western RCT framework. Members experience varied responses; the research is hypothesis-generating, not definitive.
- BPC-157. A 15-amino-acid stable gastric pentadecapeptide. Seiwerth 2021 in Frontiers in Pharmacology reviews the wound-healing animal data, where BPC-157 has been observed to support tissue repair across multiple organ systems. Human data is sparse. Maps to stem-cell exhaustion and disabled autophagy indirectly.
- Thymalin / Thymosin alpha-1. Immune-aging peptides studied for restoring T-cell signalling in older adults. Research mostly outside the US; promising mechanism, evidence quality varies by source.
The single biggest practical problem with this category is delivery. Almost every peptide is destroyed in the gut, which is why most research uses injection.
Sublingual delivery (the way the VERISORB sublingual delivery system is built) is the route VERO uses to get research-relevant doses across the mucosa without injection. The trade-off discussion is in our sublingual vs oral peptide absorption data piece.
For a deeper read on the peptides studied for age-supportive use, see our age-supportive peptides explainer. The point of including this category in a supplements review is not to pitch a product; it is to point out that pretending peptides don't exist is the single biggest blind spot in the standard longevity-supplement list.
Users report including them as a research-purposes-only layer on top of a foundational supplement stack, not as a replacement.
What does an actual longevity stack look like?
Three honest stacks. Pick the one that matches your appetite for complexity and cost. The minimum viable version covers more ground than most ten-bottle protocols.
Minimum viable stack (3 compounds).
- Creatine monohydrate, 3 to 5 g daily
- Vitamin D3 + K2, dosed to a 30 to 50 ng/mL blood level
- Omega-3 EPA + DHA, 2 g daily total, third-party tested
This stack is boring on purpose. It covers sarcopenia, the strongest correctable vitamin deficiency in temperate latitudes, and the cardiovascular endpoint with the cleanest big RCT.
Cost: under $50 per month. Most people who add this and remove half their other bottles will feel no different and will be objectively better off.
Intermediate stack (6 compounds).
- Everything in the minimum stack
- Magnesium glycinate, 200 to 400 mg in the evening
- NAD precursor of choice. NMN 250 to 500 mg orally, or sublingual NAD+ at a lower equivalent dose
- Taurine, 1 to 3 g daily
This adds the supplements with the next-best evidence-per-dollar ratio. Magnesium is the quietest sleep and cardiovascular win.
NAD precursors have the Yoshino trial behind them, with sublingual delivery as the bioavailability lever to consider. Taurine has the Singh 2023 paper, which is the most interesting Tier B compound in the field.
Advanced stack (10 compounds, including peptide-class layer).
- Everything in the intermediate stack
- Spermidine (food sources first; supplement if intake is low)
- Urolithin A, 500 to 1,000 mg
- GlyNAC, dosed per Kumar 2023 protocol
- Peptide-class layer including the LEGACY NAD+ Protocol and the broader peptide-bioregulator category from the section above
A few practical synergies and antagonisms to know:
- NMN paired with TMG (trimethylglycine) can offset the methylation drain NAD precursors create over time.
- Resveratrol and curcumin compete for the same absorption pathways and reduce each other's bioavailability when stacked.
- Iron and calcium block each other's absorption when taken together.
- Fat-soluble vitamins (A, D, E, K) should ride with a meal containing fat.
The advanced stack is not better than the intermediate stack for most people. It is more interesting if you are running biomarkers and tuning. If you are not, stop at intermediate and put the extra money into sleep, training, and food.
Frequently asked questions
What is the single best supplement for longevity?
There isn't one. The closest thing to a universal recommendation is omega-3 EPA + DHA at around 2 g per day, because the cardiovascular RCT evidence is the cleanest and cardiovascular disease is the biggest single cause of premature death.
Creatine monohydrate is a close second because of how cheap and broadly useful it is. Anyone who tells you a single capsule extends life is selling that capsule.
Are longevity supplements worth the money?
A small, evidence-led stack is probably worth it; a ten-bottle stack of fashionable compounds usually isn't. The honest spending priority is sleep, training, food quality, social connection, and then supplements. Research suggests the supplement layer adds value at the margins, not at the foundation.
Do longevity supplements actually extend lifespan in humans?
We don't have definitive proof that any single supplement extends human lifespan. We have meaningful evidence that some supplements reduce risk of specific diseases (REDUCE-IT for omega-3, VITAL secondary endpoints for vitamin D), and growing evidence that several improve healthspan markers.
Lifespan claims that go further than that are not yet supported by trial data.
What is the difference between supplements and peptides for longevity?
Supplements are dietary ingredients regulated under the FDA's DSHEA framework: vitamins, minerals, amino acids, herbs. Peptides are short chains of amino acids that often need a prescription route or a research-use designation.
The biology overlaps; the regulatory category is what separates them. Peptides like GHK-Cu and MOTS-c sit outside the supplement framework but have published mechanism work.
Can sublingual delivery improve supplement absorption?
Yes, for the right molecules. Sublingual absorption bypasses the stomach and the liver's first-pass metabolism, which matters most for molecules that get destroyed in the gut or filtered hard by the liver.
NAD+, glutathione, vitamin B12, and most research peptides have meaningfully better bioavailability via sublingual delivery than via swallowed capsules. For stable small molecules like creatine or vitamin D3, sublingual offers little advantage.
How should I cycle longevity supplements?
Most foundational supplements (vitamin D, omega-3, magnesium, creatine) are taken continuously and do not need cycling. NAD precursors are sometimes cycled five days on, two off to manage methylation load.
Peptide-class compounds are usually run in defined research cycles (a common pattern is several weeks on, a wash-out period off). Talk to your doctor before starting any supplement protocol, especially if you are on medication or have a chronic condition.
What's next in 2026?
Three things to watch over the next twelve months.
The first is whether the GlyNAC trial replicates in a larger cohort: if it does, glycine plus NAC moves from Tier B into Tier A and probably onto the minimum-viable list. The second is the rapidly maturing research on GLP-1 receptor agonists (semaglutide and tirzepatide) for endpoints beyond weight, with cardiovascular and cognitive readouts due to publish.
The third is the peptide-bioregulator field, as Western groups attempt to replicate the older Russian Epitalon work under modern trial conditions.
This review will be updated when those readouts land. The date at the top is the date that matters; reviews of this category written even twelve months ago are already out of sync with the science.
References
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G (2023). Hallmarks of aging: An expanding universe. Cell 186(2):243-278. https://pubmed.ncbi.nlm.nih.gov/36599349/. Retrieved 2026-06-01.
- Singh P, Gollapalli K, et al. (2023). Taurine deficiency as a driver of aging. Science 380(6649):eabn9257. https://pubmed.ncbi.nlm.nih.gov/37289866/. Retrieved 2026-06-01.
- Manson JE et al.; VITAL Research Group (2019). Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. NEJM 380(1):33-44. https://pubmed.ncbi.nlm.nih.gov/30415629/. Retrieved 2026-06-01.
- Kumar P, Liu C, Suliburk J, et al. (2023). Supplementing Glycine and N-Acetylcysteine (GlyNAC) in Older Adults Improves Glutathione Deficiency, Oxidative Stress, Mitochondrial Dysfunction, Inflammation, Physical Function, and Aging Hallmarks: A Randomized Clinical Trial. J Gerontol A Biol Sci Med Sci 78(1):75-89. https://pubmed.ncbi.nlm.nih.gov/35975308/. Retrieved 2026-06-01.
- Andreux PA, Blanco-Bose W, Ryu D, et al. (2019). The mitophagy activator urolithin A is safe and induces a molecular signature of improved mitochondrial and cellular health in humans. Nature Metabolism 1(6):595-603. https://pubmed.ncbi.nlm.nih.gov/32694802/. Retrieved 2026-06-01.
- Lee C, Zeng J, Drew BG, et al. (2015). The mitochondrial-derived peptide MOTS-c promotes metabolic homeostasis and reduces obesity and insulin resistance. Cell Metabolism 21(3):443-454. https://pubmed.ncbi.nlm.nih.gov/25738459/. Retrieved 2026-06-01.
- Yoshino M, Yoshino J, Kayser BD, et al. (2021). Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science 372(6547):1224-1229. https://pubmed.ncbi.nlm.nih.gov/33888596/. Retrieved 2026-06-01.
- Eisenberg T, Abdellatif M, Schroeder S, et al. (2016). Cardioprotection and lifespan extension by the natural polyamine spermidine. Nature Medicine 22(12):1428-1438. https://pubmed.ncbi.nlm.nih.gov/27841876/. Retrieved 2026-06-01.
- Forbes SC, Cordingley DM, et al. (2022). Effects of Creatine Supplementation on Brain Function and Health. Nutrients 14(5):921. https://pubmed.ncbi.nlm.nih.gov/35267907/. Retrieved 2026-06-01.
- Avgerinos KI, Spyrou N, Bougioukas KI, Kapogiannis D (2018). Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials. Experimental Gerontology 108:166-173. https://pubmed.ncbi.nlm.nih.gov/29704637/. Retrieved 2026-06-01.
- Veronese N, Demurtas J, et al. (2020). Magnesium and health outcomes: an umbrella review of systematic reviews and meta-analyses. European Journal of Nutrition 59(1):263-272. https://pubmed.ncbi.nlm.nih.gov/30684032/. Retrieved 2026-06-01.
- Bhatt DL, Steg PG, et al.; REDUCE-IT Investigators (2019). Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. NEJM 380(1):11-22. https://pubmed.ncbi.nlm.nih.gov/30415628/. Retrieved 2026-06-01.
- Pickart L, Margolina A (2018). Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci 19(7):1987. https://pubmed.ncbi.nlm.nih.gov/29986520/. Retrieved 2026-06-01.
- Khavinson VKh, Kuznik BI, Ryzhak GA (2012). Peptide bioregulators: the new class of geroprotectors. Communication 1. Results of experimental studies. Advances in Gerontology 25(4):696-708. https://pubmed.ncbi.nlm.nih.gov/23734519/. Retrieved 2026-06-01.
- Seiwerth S, Milavic M, Vukojevic J, et al. (2021). Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. Frontiers in Pharmacology 12:627533. https://pubmed.ncbi.nlm.nih.gov/34267654/. Retrieved 2026-06-01.
- Chachay VS, Macdonald GA, Martin JH, et al. (2014). Resveratrol does not benefit patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 12(12):2092-2103.e6. https://pubmed.ncbi.nlm.nih.gov/24582567/. Retrieved 2026-06-01.
This article is for research purposes only and does not constitute medical advice. Talk to your doctor before starting any supplement protocol, especially if you are on medication or managing a chronic condition.
Ready to explore the peptide-class layer of a longevity stack? Start with the LEGACY NAD+ Protocol →
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.