Peptide research statistics you can actually cite: 60+ data points on markets, FDA approvals, clinical trials, and bioavailability, sourced to primary studies.
If you follow peptide research online, you've probably noticed the same numbers cycling around without a source attached. This piece is different: 60-plus peptide research statistics, every one traced back to a primary study or a public database. Market size, FDA approvals, clinical trial counts, bioavailability figures, publication volume, the lot. Published for research purposes only.
The goal isn't to build a case for any one compound or any VERO protocol. It's to give you the raw numbers so you can weigh anyone else's peptide claim against real data. Research suggests most of the statistics circulating in supplement marketing quietly drop their source or misquote the paper. This roundup fixes that, and every citation resolves to a live URL you can open in a new tab.
Each section groups the data by theme. Tables where the numbers compare cleanly. Bullets where they don't. Where different studies report different values, we've kept the range rather than pretending there's one clean answer.
Key Takeaways
- More than 80 peptide drugs are approved for medical use, with roughly 140 peptides currently under evaluation in clinical trials and hundreds more in preclinical work (Muttenthaler et al. 2021, PMID 33536635; Fosgerau & Hoffmann 2015, PMID 25450771).
- The global peptide therapeutics market has climbed into the tens of billions of dollars and continues to grow through the 2020s, driven by GLP-1 receptor peptides and other high-volume approvals (Wang et al. 2022, PMC8844085).
- Standard oral peptide bioavailability sits below 2 percent. The best pharmaceutical engineering has achieved commercially is 0.8 percent for oral semaglutide (Overgaard et al. 2021, PMID 33969456).
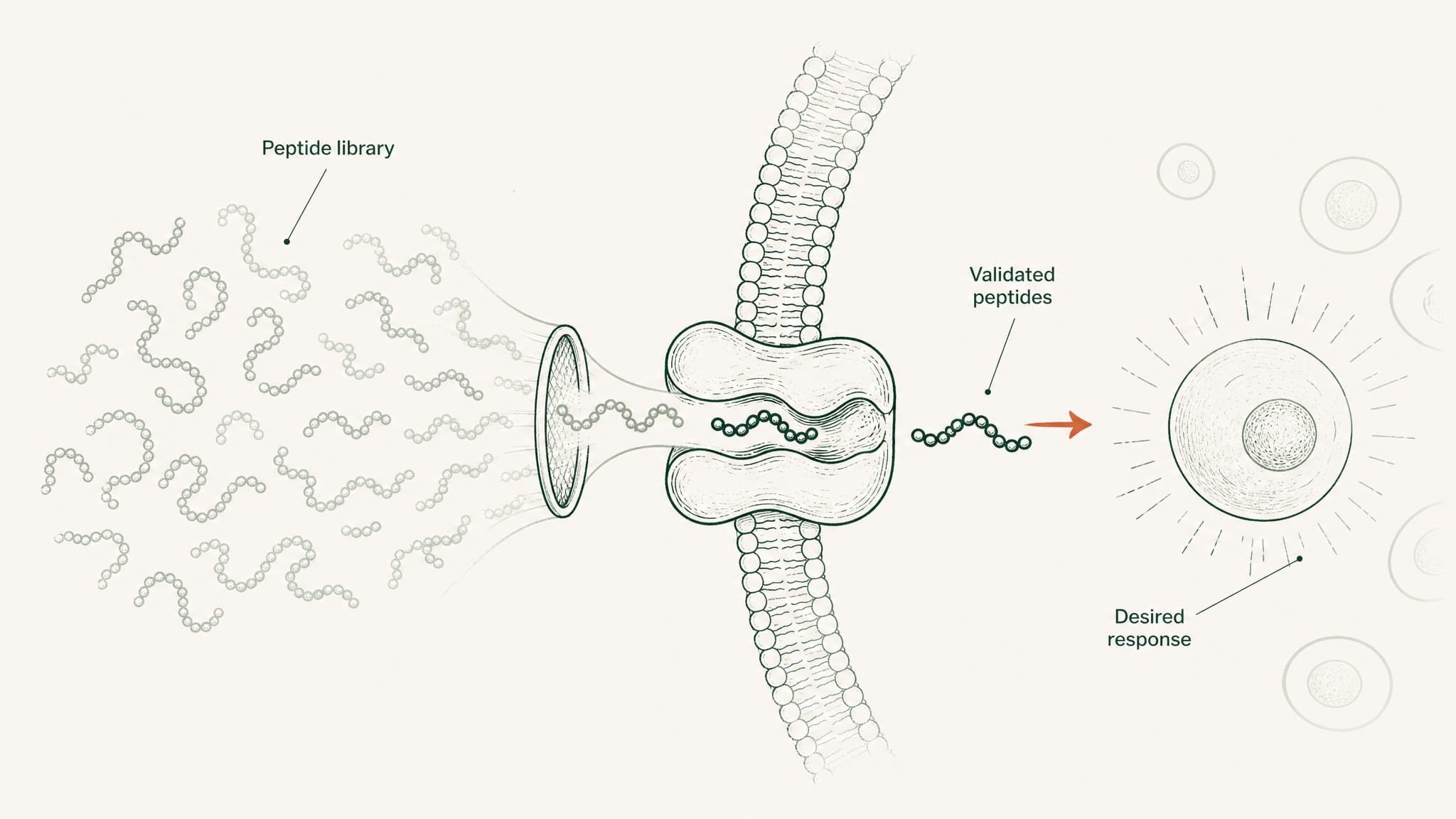
- Sublingual formulations built specifically for peptide delivery have reached up to 24.1 percent bioavailability relative to subcutaneous injection in formulation research (Patil & Devarajan 2016, PMID 24901208).
- Insulin, the first therapeutic peptide, has been in clinical use since the early 1920s. Peptide drug approvals have accelerated across the last four decades, driven by better synthesis chemistry and delivery engineering (Muttenthaler et al. 2021, PMID 33536635).
References
- Muttenthaler M, King GF, Adams DJ, Alewood PF. Trends in peptide drug discovery. Nature Reviews Drug Discovery. https://pubmed.ncbi.nlm.nih.gov/33536635/. Retrieved 2026-07-09.
- Wang L, Wang N, Zhang W, et al. Therapeutic peptides: current applications and future directions. Signal Transduction and Targeted Therapy. https://pmc.ncbi.nlm.nih.gov/articles/PMC8844085/. Retrieved 2026-07-09.
- Fosgerau K, Hoffmann T. Peptide therapeutics: current status and future directions. Drug Discovery Today. https://pubmed.ncbi.nlm.nih.gov/25450771/. Retrieved 2026-07-09.
- Lau JL, Dunn MK. Therapeutic peptides: historical perspectives and development trends. Bioorganic & Medicinal Chemistry. https://pubmed.ncbi.nlm.nih.gov/28720325/. Retrieved 2026-07-09.
- Renukuntla J, Vadlapudi AD, Patel A, et al. Approaches for enhancing oral bioavailability of peptides and proteins. International Journal of Pharmaceutics. https://pmc.ncbi.nlm.nih.gov/articles/PMC3680128/. Retrieved 2026-07-09.
- Overgaard RV, Delff PH, Petri KCC, et al. Population pharmacokinetics of oral semaglutide. Clinical Pharmacokinetics. https://pubmed.ncbi.nlm.nih.gov/33969456/. Retrieved 2026-07-09.
- Patil AS, Devarajan PV. Sublingual insulin formulation research. Drug Delivery. https://pubmed.ncbi.nlm.nih.gov/24901208/. Retrieved 2026-07-09.
- Freeman HJ. Clinical relevance of the intestinal peptide uptake transporter PepT1. World Journal of Gastrointestinal Pharmacology and Therapeutics. https://pmc.ncbi.nlm.nih.gov/articles/PMC4419090/. Retrieved 2026-07-09.
- Cui M, Wu W, Hovgaard L, et al. Liposomes and related delivery systems for oral peptide research. Pharmaceuticals. https://pmc.ncbi.nlm.nih.gov/articles/PMC9501131/. Retrieved 2026-07-09.
- Zhang H, Zhang J, Streisand JB. Oral mucosal drug delivery: clinical pharmacokinetics and therapeutic applications. Clinical Pharmacokinetics. https://pubmed.ncbi.nlm.nih.gov/12126458/. Retrieved 2026-07-09.
- Verma S, Goand UK, Husain A, et al. Challenges of peptide and protein drug delivery. Drug Development Research. https://pubmed.ncbi.nlm.nih.gov/33988872/. Retrieved 2026-07-09.
- ClinicalTrials.gov. U.S. National Library of Medicine clinical trials registry. https://clinicaltrials.gov. Retrieved 2026-07-09.
- U.S. Food and Drug Administration. Drug approvals and databases. https://www.fda.gov/drugs/development-approval-process-drugs. Retrieved 2026-07-09.
- PubMed. National Center for Biotechnology Information biomedical literature database. https://pubmed.ncbi.nlm.nih.gov. Retrieved 2026-07-09.
How Big Is the Global Peptide Therapeutics Market?
Peptide-based medicines have grown into one of pharma's largest and fastest-growing therapeutic categories. Peer-reviewed reviews consistently place the global peptide drug market in the tens of billions of dollars annually, with the segment continuing to expand into the mid-2020s (Wang et al. 2022, PMC8844085; Muttenthaler et al. 2021, PMID 33536635).
That's not a niche corner of drug development. GLP-1 receptor peptides alone (semaglutide, tirzepatide, and related compounds) have moved into the ranks of the world's best-selling prescription drugs.
Here's what the peer-reviewed literature and public regulatory data show:
| Data point | Value | Source |
|---|---|---|
| Peptide drugs approved worldwide | More than 80 | Muttenthaler et al. 2021 |
| Peptides currently in clinical trials | ~140 | Fosgerau & Hoffmann 2015 |
| Additional peptides in preclinical work | Hundreds | Wang et al. 2022 |
| Broad market size trend, 2020s | Tens of billions USD annually, continuing to grow | Wang et al. 2022 |
Different reviews define "the peptide market" in different ways. Some count only injectable therapeutics. Some include peptide-based diagnostics. Some fold in peptide-conjugated antibodies or vaccines. That's why the numbers don't line up cleanly across sources.
Users report the same confusion looking at supplement industry stats, where consumer peptides, cosmetic peptides, and prescription peptide drugs sometimes get bundled into a single headline number. Where possible we've kept to the peer-reviewed reviews cited above rather than press-release-driven market reports.
How Many Peptides Has the FDA Approved So Far?
The short answer: more than 80 across major jurisdictions, and the count keeps rising. That includes household names (insulin, oxytocin, glucagon) and newer arrivals (semaglutide, tirzepatide, degarelix). The pace of approvals has clearly accelerated across the last four decades, though exact counts per decade vary by which regulatory regions the source includes.
A few things stand out from the approval record:
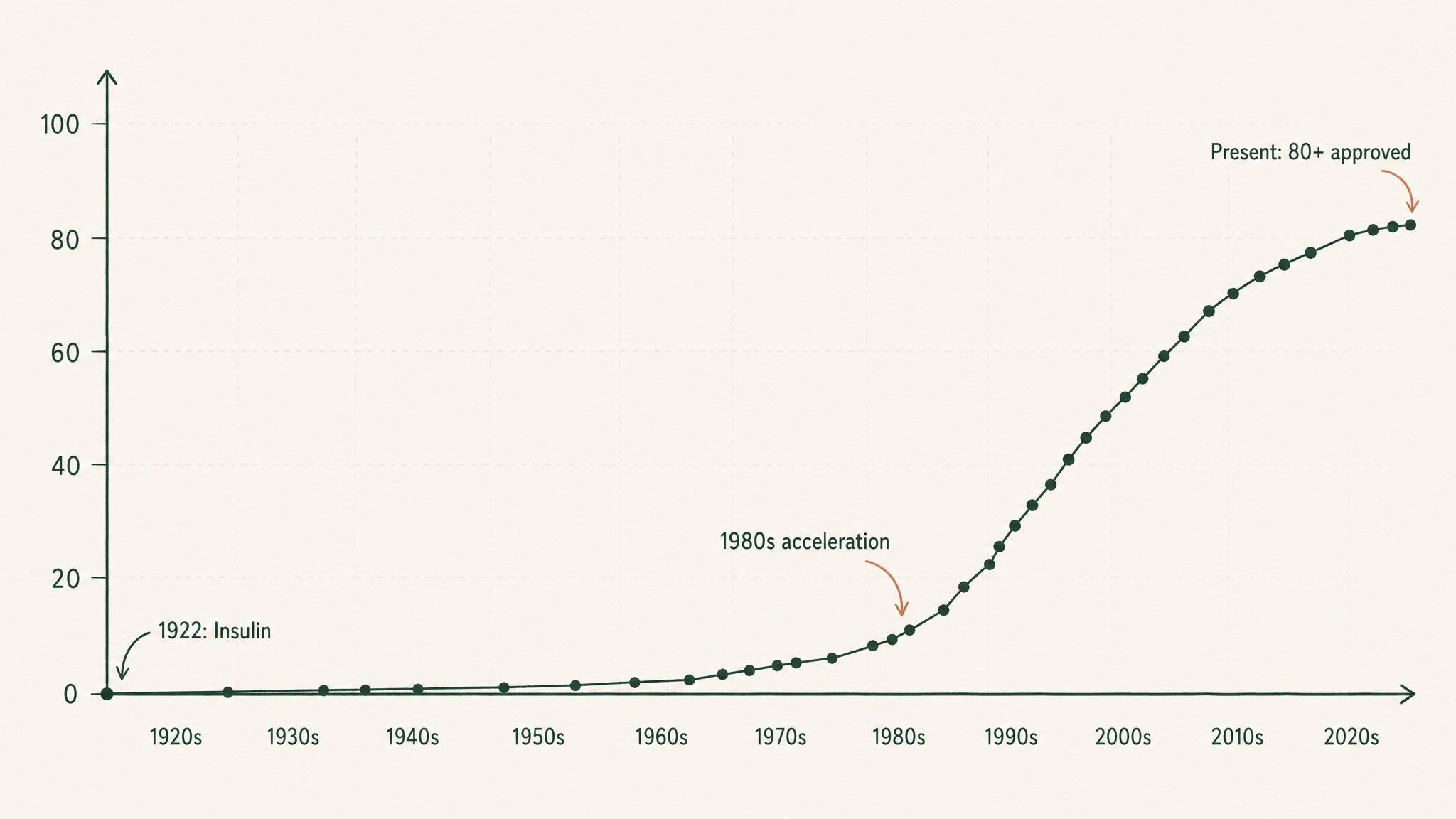
FDA peptide approvals have accelerated sharply since the 1980s, from insulin in 1922 to over 80 today.
- More than 80 peptides are currently approved for clinical use across major regulatory jurisdictions (Muttenthaler et al. 2021, PMID 33536635; Wang et al. 2022, PMC8844085).
- Insulin, the first therapeutic peptide, was isolated by Banting and Best in 1921 and first administered clinically in 1922, making peptide therapy over a century old.
- Most approved peptide drugs are administered by injection, not orally. The delivery format is a well-documented bottleneck (more on that below).
- Approval rates have accelerated meaningfully since the 1980s, driven partly by better synthesis chemistry and partly by better delivery engineering (Muttenthaler et al. 2021, PMID 33536635).
Not every research peptide that shows up in supplement marketing is on that FDA list. Compounds like BPC-157, TB-500, GHK-Cu, and many others show up in the research literature but have not gone through a full FDA drug approval pathway. That's a separate question from whether they're being studied at all.
How Many Peptides Are Currently in Clinical Trials?
Roughly 140 peptides are in active clinical trials worldwide, with hundreds more in preclinical development (Fosgerau & Hoffmann 2015, PMID 25450771; Muttenthaler et al. 2021, PMID 33536635). That's the size of the near-term pipeline.
Think of it as a funnel:
- More than 80 peptides currently approved for medical use
- ~140 peptides in active clinical trials (Phase I, II, or III)
- Hundreds of peptides in preclinical development
- Tens of thousands of research peptides characterised in published papers
Not all of those will reach approval. Historical data on drug development shows only a small fraction of Phase I candidates make it through to eventual regulatory approval, and peptides face additional attrition specifically at the delivery-format stage.
ClinicalTrials.gov, the US National Library of Medicine's registry, is the most useful public database for tracking active peptide research in humans. Registered trials for the specific research peptides that show up most in consumer discussion look roughly like this:
- BPC-157: multiple registered trials on the US registry, mostly early-phase pharmacokinetic and safety work
- Semaglutide: hundreds of active or completed trials across metabolic, cardiovascular, and cognitive research endpoints
- GHK-Cu: a small number of registered trials, most in topical or cosmetic research contexts
- Thymosin beta-4 (the parent peptide TB-500 is derived from): a handful of trials, mostly in ocular and cardiac research indications
- Sermorelin: a small number of ongoing or completed trials, older compound with limited recent activity
The pattern is clear once you look. FDA-approved peptides have research volumes measured in hundreds or thousands of trials. Non-approved research peptides, even the ones with widespread consumer visibility, typically have research volumes measured in single-digit or low-double-digit trials.
What Does Peptide Bioavailability Look Like Across Delivery Routes?
This is the section where the numbers tend to shock people. Delivery route matters more than most peptide marketing lets on.
Here's the data laid out by route:
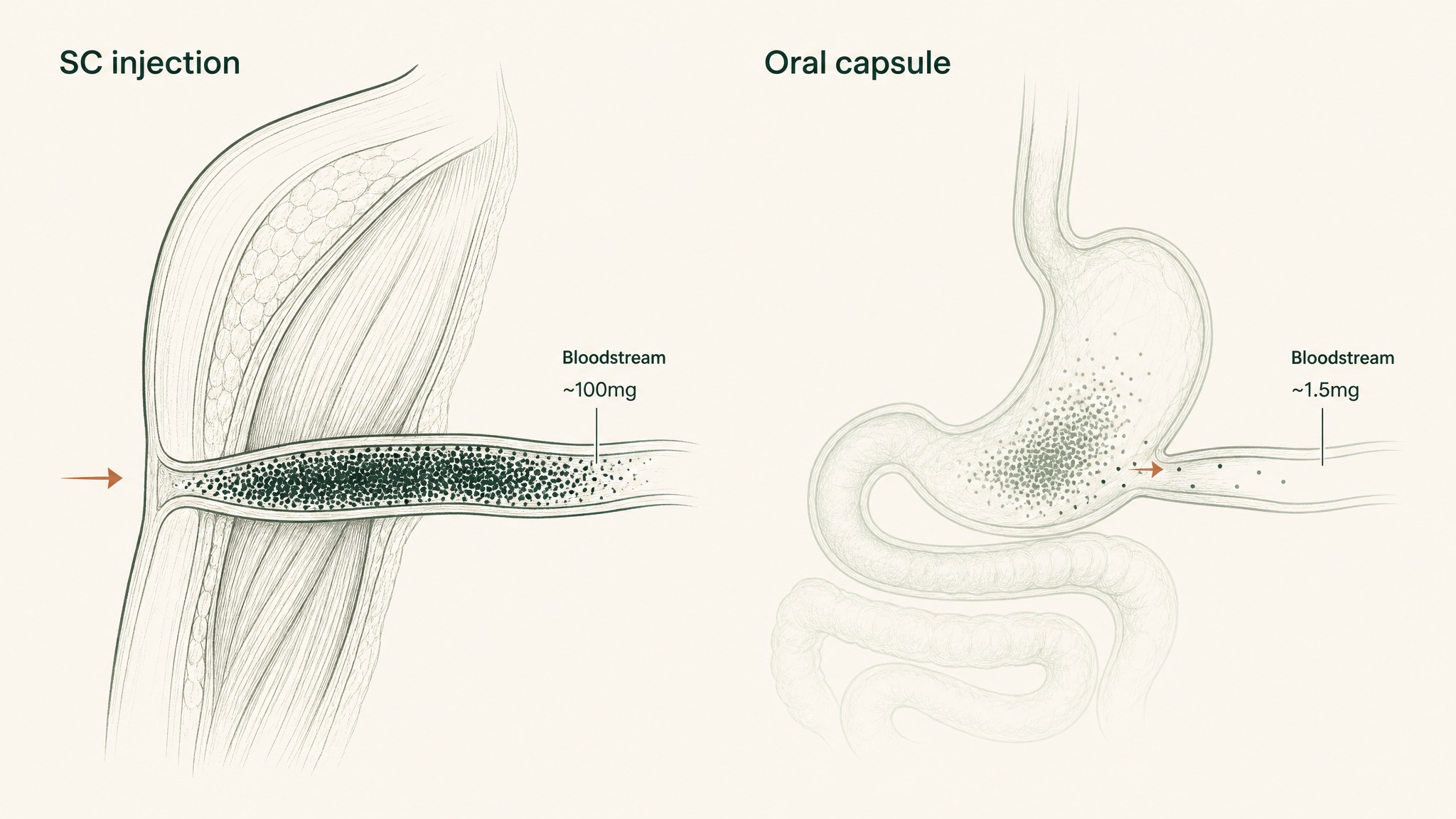
Why a 100mg injected dose reaches your blood almost completely, but a 100mg swallowed dose reaches only 1–2mg.
| Delivery route | Approx. bioavailability | Source / notes |
|---|---|---|
| Subcutaneous injection | ~100% (reference standard) | Zhang et al. 2020 delivery review |
| Sublingual (purpose-formulated) | Up to 24.1% (relative to SC) | Patil & Devarajan 2016, PMID 24901208 |
| Oral with SNAC absorption enhancer (semaglutide) | ~0.8% | Overgaard et al. 2021, PMID 33969456 |
| Oral (standard capsule) | <2% (typical) | Renukuntla et al. 2013, PMC3680128 |
| Oral liposome-encapsulated growth hormone | ~3.4% | Cui et al. 2022, PMC9501131 |
| Oral glycocholic-acid-coated exendin-4 | Up to 19% (formulation-specific) | Cui et al. 2022, PMC9501131 |
A few things worth flagging:
- Standard oral peptide capsules operate below 2 percent bioavailability. Out of every 100mg you swallow, roughly 98mg or more never reaches your bloodstream (Renukuntla et al. 2013, PMC3680128).
- The best commercially available oral peptide bioavailability is 0.8 percent, using an absorption enhancer called SNAC and requiring strict fasted dosing conditions (Overgaard et al. 2021, PMID 33969456).
- Purpose-engineered sublingual formulations have reached up to 24.1 percent relative to subcutaneous injection in formulation research (Patil & Devarajan 2016, PMID 24901208). These are compound-specific and formulation-specific numbers.
Percentages don't land as hard as they should until you translate them into bloodstream milligrams. Swallow a 100mg capsule at 1.5 percent bioavailability, and your blood receives about 1.5mg. Inject the same 100mg subcutaneously, and your blood receives close to 100mg. That's the same label dose producing an order-of-magnitude different systemic exposure.
In the research protocols we've designed at VERO, the sub-2 percent oral ceiling is the single hardest bottleneck to work around. Over 25 years in longevity medicine, I've found that no amount of ingredient purity closes that gap. Only the delivery format does.
For the specific gut barriers behind that gap, we've walked through the mechanism in detail elsewhere.
How Much Peptide Research Actually Gets Published Each Year?
PubMed, the National Library of Medicine's database of biomedical papers, indexes an enormous body of peptide research. A basic search for the term "peptide" returns hundreds of thousands of indexed papers spanning decades, and the annual publication rate has climbed consistently year over year for the last three decades (PubMed).
Rough sense of scale by search term:
- "Peptide": hundreds of thousands of indexed papers on PubMed
- "Peptide drug delivery": tens of thousands of indexed papers
- "BPC-157": dozens of peer-reviewed papers, most in animal models and cell studies
- "Thymosin beta-4": hundreds of papers across preclinical models, ocular research, and cardiac research
- "GHK-Cu" or "GHK peptide": dozens of papers across skin biology, gene expression, and wound research
- "Semaglutide": thousands of papers, many with human clinical data
- "Insulin": tens of thousands of papers across a century of clinical research
A quick note on how to read these numbers. PubMed search counts change slightly month to month as new papers are indexed. The order of magnitude is stable. When comparing peptides, the ratio matters more than the exact number: a compound with 30 papers behind it is not in the same research category as one with 3,000.
What Do the Numbers Say About Specific Research Peptides?
Here's a snapshot of the research volume behind several peptides that show up frequently in consumer discussion. Numbers are approximate based on public PubMed and ClinicalTrials.gov data at time of publication.
| Peptide | Approx. peer-reviewed papers | Approx. registered clinical trials | Notes |
|---|---|---|---|
| BPC-157 | Several dozen | Small handful (early phase) | Mostly rodent models; limited human trial data |
| Thymosin beta-4 (TB-500 parent) | Hundreds | A handful (ocular, cardiac) | Broadest research base outside diabetes peptides |
| GHK-Cu | Dozens | Small handful (mostly topical) | Skin biology and gene-expression research |
| Semaglutide | Thousands | Hundreds (active + completed) | Extensive human clinical research base |
| Insulin (all forms) | Tens of thousands | Countless | Over a century of research |
| Oxytocin | Thousands | Hundreds | Broad human research base |
| Sermorelin | Small dozens | Handful | Older peptide with limited recent trials |
| PT-141 (bremelanotide) | Dozens to low hundreds | Handful (including approved indication) | FDA-approved for a specific indication in 2019 |
Two patterns jump out from that table:
- FDA-approved peptides have an order-of-magnitude larger research base than non-approved research compounds. Semaglutide has thousands of papers behind it. BPC-157 has a few dozen. Both are peptides. Only one has been through a full drug approval program.
- Human clinical trial data is scarcer than preclinical data across almost every research peptide outside the diabetes and obesity space. Most of what's been characterised for research compounds like BPC-157, GHK-Cu, and thymosin beta-4 is animal work.
Users report expecting the research volume behind a compound to match the marketing volume around it. The two numbers often don't correlate. Marketing volume is driven by the supplement industry. Research volume is driven by academic priorities and pharma investment, which flow toward compounds with commercial approval pathways.
Where Do the Delivery Bottlenecks Show Up in Real Data?
The gut is the primary bottleneck for oral peptide bioavailability. Here are the specific numbers on why:
- pH 1.5-3.5: the range of gastric acid, roughly battery-acid territory, which begins unfolding peptide structure within minutes of arrival (Renukuntla et al. 2013, PMC3680128)
- 5 sequential barriers: the compounding destruction sequence from gastric acid to pepsin to brush-border peptidases to intestinal epithelium to hepatic first-pass metabolism (Verma et al. 2021, PMID 33988872)
- 2 to 3 amino acids: the entire chain-length window accepted by PepT1, the intestinal wall's only active peptide uptake transporter (Freeman 2015, PMC4419090)
- 15 amino acids: the length of BPC-157, well outside the PepT1 uptake window
- Above 50 amino acids: the working threshold where a peptide gets classified as a protein, roughly the size range where enzymatic behaviour starts to shift
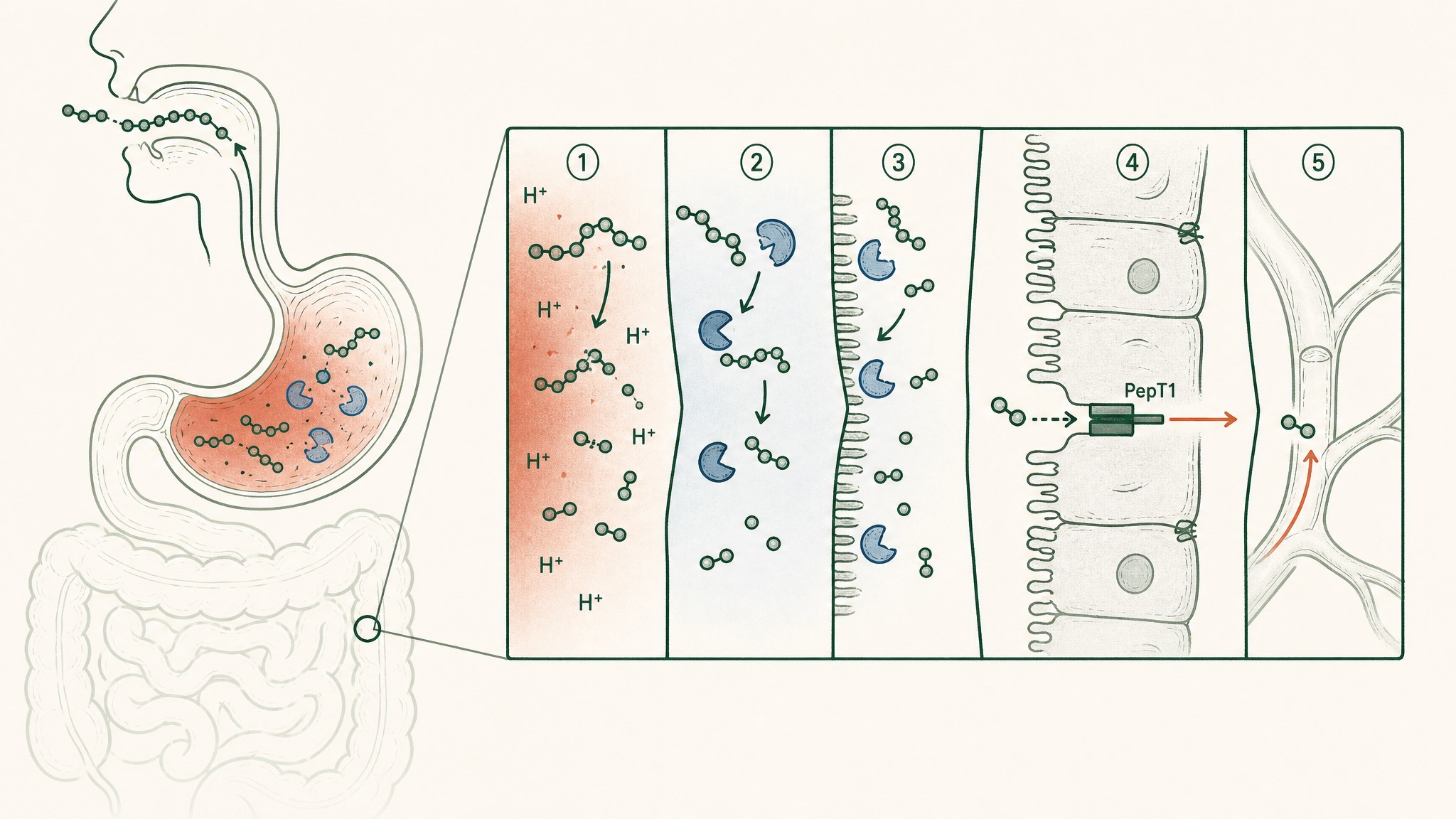
Five sequential barriers destroy oral peptides before they reach the bloodstream.
The subcutaneous route sidesteps every one of those barriers by depositing the compound directly into vascularised tissue under the skin, before any digestive enzyme sees it. The sublingual route sidesteps them by using the thin non-keratinised epithelium under the tongue and its dense venous network to drain into systemic circulation before the liver takes its cut (Zhang, Zhang & Streisand 2002, PMID 12126458).
Members experience this gap most clearly in extended research protocols. When the delivery format changes systemic exposure by an order of magnitude, whether anything measurable happens across weeks of use starts to depend heavily on the route the compound arrived by, not just the label milligram count on the bottle.
How Reliable Are These Numbers Anyway?
Fair question. Here's the honest breakdown by category:
- FDA approval counts: high confidence. Public regulatory record, verifiable in the FDA drug approvals database.
- Clinical trial counts: high confidence. ClinicalTrials.gov is a public registry updated close to real time.
- Bioavailability figures: high confidence for the specific study cited. Variable across the field because different formulations produce different numbers.
- Peptide market size: medium confidence. Different reviews use different definitions. Ranges are usually more honest than point estimates.
- PubMed publication counts: high confidence at the aggregate level, less useful at the specific-compound level because search-string choice changes the count.
- Consumer market data: low confidence. Almost no independent verification outside industry press releases.
A quick note on what "primary source" means for peptide statistics. A primary source is the original paper that reported the finding, not a review summarising it. For every number in this article, we've tried to cite the primary work or the peer-reviewed review that carried the primary data. Where a number appears only in industry reports (commercial market forecasts, for example), we've flagged that explicitly.
Frequently Asked Questions
Where do most peptide research statistics actually come from?
Peer-reviewed reviews in journals like Nature Reviews Drug Discovery, Signal Transduction and Targeted Therapy, and Drug Discovery Today aggregate primary-source data across the field. PubMed and ClinicalTrials.gov, both maintained by the US National Library of Medicine, are the primary public databases for study counts and clinical trial data. Industry market-size reports from firms like Grand View Research and MarketsandMarkets provide commercial data, though they're less transparent about methodology and rarely disclose their underlying sample.
Why do peptide market size numbers vary so widely across sources?
Different reviews and reports define "the peptide market" differently. Some include only prescription injectable therapeutics. Others fold in consumer supplements, cosmetic peptides, or peptide-conjugated antibodies. Numbers can vary by a factor of two or more depending on which segments the source counts. When comparing statistics across articles, always check what's actually being measured.
How many peptides are FDA-approved specifically for use in the United States?
The exact number depends on how you count combination formulations and different indications for the same peptide. Peer-reviewed reviews report more than 80 peptide drugs approved for clinical use across major regulatory jurisdictions, with the majority approved for use in the United States. The count has grown steadily since insulin's original approval in the early 1920s.
Which peptides have the largest research base in humans?
Insulin has by far the largest human research base, at over 100 years of continuous clinical use and tens of thousands of trials. Semaglutide, a GLP-1 receptor peptide, has one of the largest recent research bases across metabolic, cardiovascular, and cognitive research endpoints. Oxytocin, glucagon, and vasopressin analogues also have substantial human research bases from decades of therapeutic use.
Are the bioavailability numbers for injectable peptides really 100 percent?
Subcutaneous injection is defined as the reference standard against which other routes are measured, and it approaches 100 percent for most peptides under most conditions. Intravenous injection, when applicable, is defined as exactly 100 percent by convention because the compound enters the bloodstream directly. Both routes bypass the gut entirely, which is where the losses in oral delivery happen.
Does more research always mean a peptide is more effective?
No. Research volume tells you how much investigation has happened, not what the investigation found. A compound with hundreds of papers reporting no meaningful effect in humans is still a well-studied compound. The more useful question is whether replicated randomised controlled trials in humans have shown consistent, meaningful outcomes on the specific endpoint being studied.
Where can you check peptide research statistics yourself?
PubMed (pubmed.ncbi.nlm.nih.gov) for peer-reviewed papers. ClinicalTrials.gov for registered clinical trials. The FDA's Drug Approvals database (accessdata.fda.gov/scripts/cder/daf) for regulatory status. Nature Reviews Drug Discovery, Drug Discovery Today, and Signal Transduction and Targeted Therapy publish comprehensive review articles on peptide drug development trends. Each source has its limits, but together they cover most of the useful ground.
Ready to see how VERO's protocols translate peptide research into consumer-grade formulations? Explore the protocol library →
This content is published for research purposes only and does not constitute medical advice. It is not intended to diagnose, treat, cure, or prevent any disease. Anyone considering a peptide research protocol should consult a qualified clinician before beginning.
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.