
NAD supplement vs injection compared on bioavailability, cost, onset and what the research suggests. Oral, sublingual, IV and IM routes side by side.
If you have been looking at NAD lately, you have probably noticed two very different price tags. A bottle of NAD pills runs forty or fifty dollars. An NAD IV drip at a wellness clinic runs four hundred to a thousand. The clinics quietly imply the pills do nothing and the injection is the only thing that "works." The pill brands quietly imply the injection is overkill. This guide is for research purposes only, and it lays out what the bioavailability research actually shows about each route, so you can decide which one fits your goal.
The short version:
- NAD injections (IV or IM) put NAD directly into your bloodstream. Bioavailability is essentially 100% because you bypass your gut and liver entirely.
- Oral NAD supplements (capsules, tablets) lose most of their dose to stomach acid, gut enzymes, and first-pass liver metabolism before anything systemic happens.
- Sublingual NAD (under the tongue) sits in the middle. It bypasses the stomach but still uses much smaller doses than an injection, and it does not require a clinic.
- The honest question is not "which is best." It is "which route fits the dose, frequency, cost and lifestyle you can actually maintain for years."
What's the actual difference between an NAD supplement and an NAD injection?
The cleanest way to think about it: a supplement asks your body to absorb NAD. An injection skips the asking part.
Your gut is built to be picky. It is a security checkpoint that breaks most large, charged molecules down before they reach your bloodstream. NAD is a large, charged molecule. So when you swallow a 500 mg NAD capsule, your stomach acid and gut enzymes start dismantling it within minutes. By the time anything reaches your liver, most of what is left gets converted into smaller building blocks called precursors (mainly nicotinamide), which your liver then has to rebuild back into NAD inside your cells.
How NAD reaches your bloodstream differently by swallowing, placing under tongue, injecting into muscle, or IV drip.
An injection skirts the whole checkpoint. The needle puts NAD directly into a vein (IV) or a muscle (IM), and from there it diffuses into the bloodstream without any digestion at all.
Here is the practical picture:
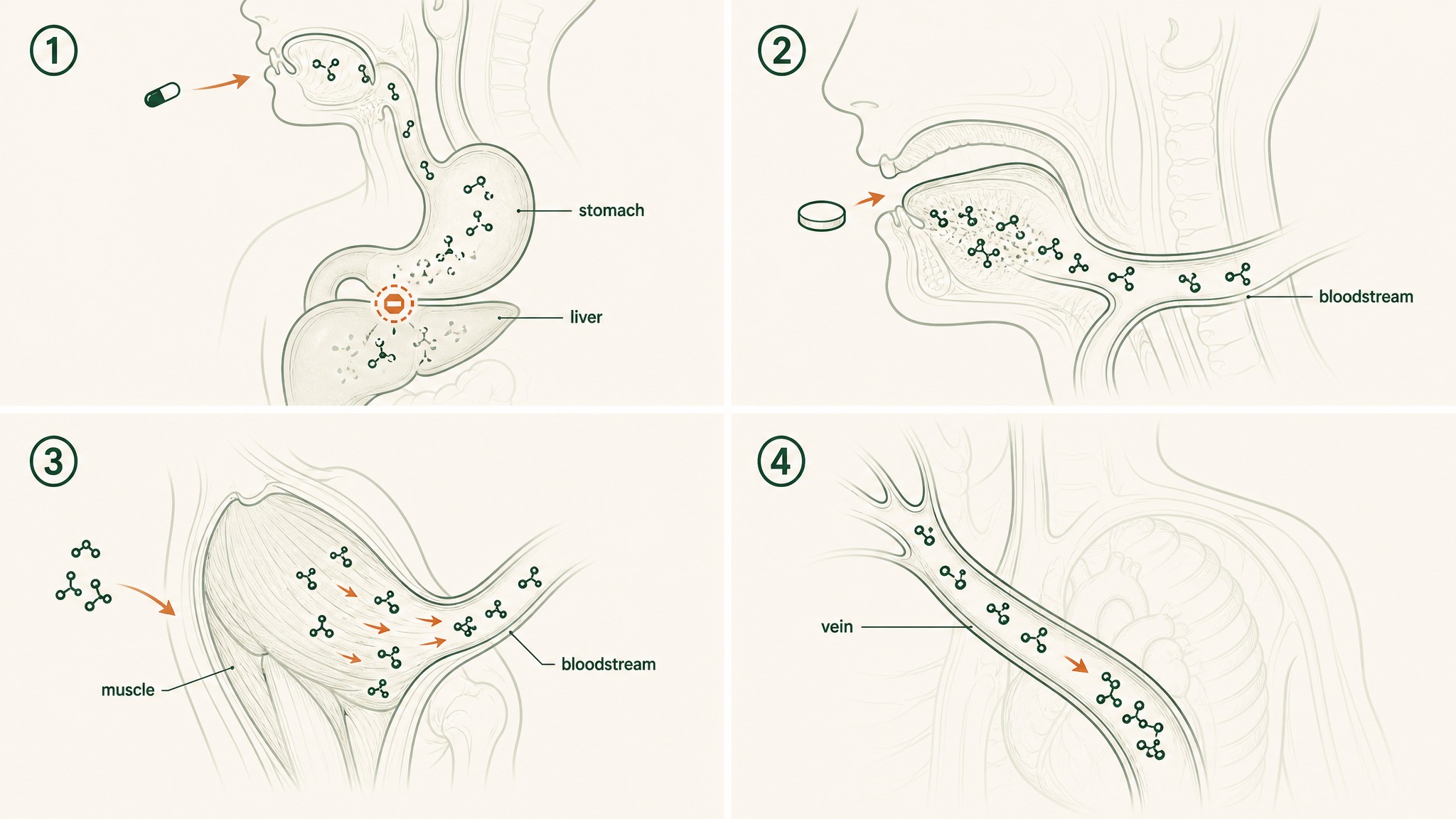
- Oral capsule: swallow → stomach → liver → most degraded → small fraction systemic
- Sublingual tablet: under the tongue → absorbed through mouth lining → into bloodstream, bypassing the stomach
- IM injection: needle into muscle → slow diffusion into bloodstream over hours
- IV drip: needle into vein → direct, immediate, 100% systemic exposure
Each route is solving the same problem (get NAD into your blood) using a completely different strategy. The cost, the inconvenience, and the bioavailability all shift accordingly.
How does an NAD injection actually get NAD into your bloodstream?
The simplest analogy: an injection is the express lane. Everything else is the local road with traffic lights.
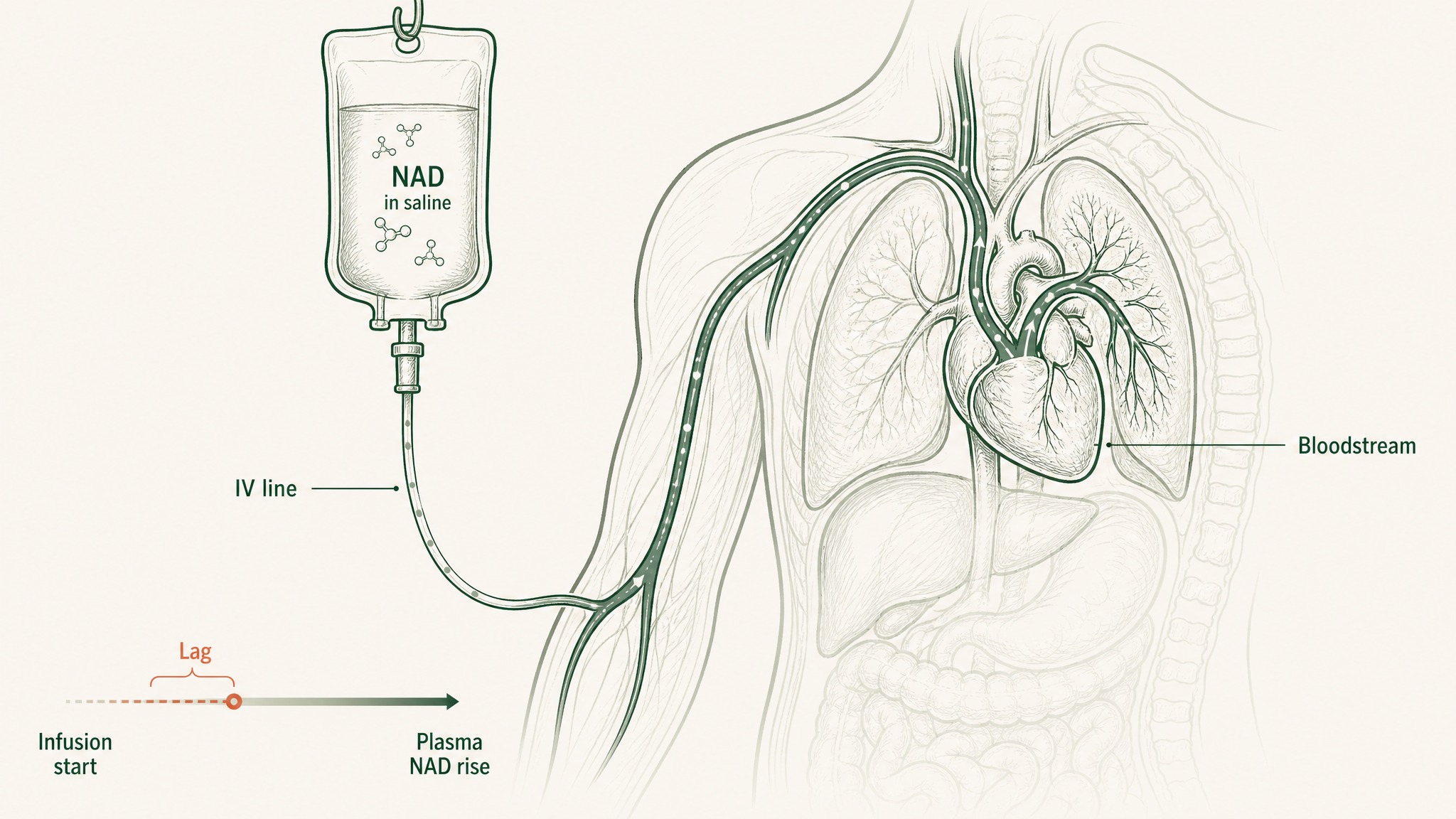
When a clinic gives you an IV NAD drip, they typically mix 250 to 1000 mg of NAD into a saline bag, hook you up to a slow infusion line, and run it in over two to four hours. The slow drip is not optional. Pushed in too fast, IV NAD reliably produces chest pressure, flushing and nausea, which is why the bag has to crawl.
How an IV NAD drip enters the bloodstream slowly over hours, not minutes.
Most clinic visits last longer than a film.
There is also an intramuscular version. Grant and colleagues (2019) ran the first formal pharmacokinetic study of IV NAD in humans, and they reported that plasma NAD did rise during the infusion, but with a measurable lag and significant individual variation. That gap between "infusion started" and "blood levels actually rose" is one of the things the IV-NAD marketing tends to skip.
Two practical realities of the injection route:
- You need a clinic. IV NAD is administered by a nurse or doctor. Most US wellness clinics charge $400 to $1,000 per session, with protocols usually running 4 to 10 sessions to start.
- It is not painless. Even at slow drip rates, members experience pressure in the chest and a wave of nausea that the clinic warns you about before the line goes in.
In our protocol design, we have watched members try IV NAD as a "loading dose" and then move to a sustained sublingual routine to maintain the levels they bought with the drip. The injection is a short, expensive sprint; the supplement is the long, cheaper distance run.
How does an oral or sublingual NAD supplement compare?
Picture your gut as a denaturation chamber: warm, acidic, full of enzymes whose job is to dismantle anything that looks like food. An oral NAD capsule walks straight into that chamber.
Most oral NAD products do not actually contain NAD itself. They contain a precursor (NMN, NR, or niacinamide) which your cells then reassemble into NAD. The reason is simple: direct oral NAD survives the gut poorly enough that brands switched to precursors that survive a bit better. For the full precursor breakdown, see our NAD supplement guide.
Oral NAD breaks down in stomach acid; sublingual NAD absorbs directly into blood through mouth capillaries.
Even with the precursor switch, oral bioavailability is the catch:
- Oral NR: Trammell and colleagues (2016) reported in Nature Communications that single oral doses raised blood NAD in healthy volunteers, but the absorbed fraction varied between individuals and was nowhere near 100%.
- Oral NMN: Yoshino and colleagues (2021) reported metabolic shifts in postmenopausal women taking 250 mg daily, but the intact parent molecule's systemic exposure remains debated.
- Direct oral NAD+: poor. The molecule is too fragile and too charged to make it through the gut in any usable quantity.
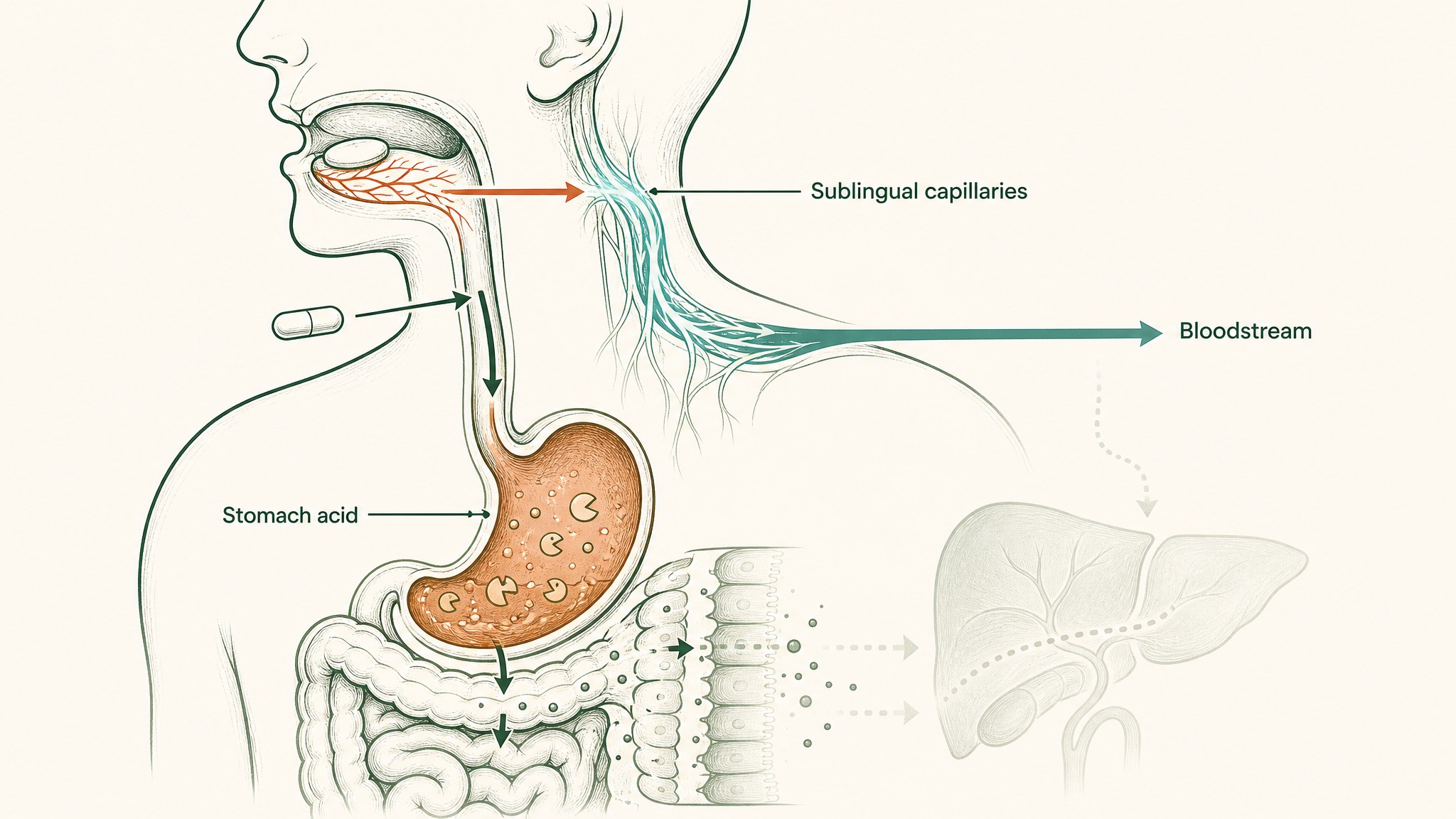
Sublingual delivery sits between these two worlds. A small tablet held under the tongue dissolves into the network of capillaries inside your mouth, which feed directly into the systemic circulation. No stomach acid, no first-pass liver metabolism. This is the principle VERISORB is built around, and it is the same logic behind nitroglycerin tablets and sublingual B12: a small dose absorbed efficiently can match a much larger oral dose on what actually reaches the bloodstream.
This is the whole reason LEGACY, VERO's sublingual NAD+ protocol, uses doses far below what oral capsules carry. The math is built around delivered NAD, not labelled NAD.
What does the bioavailability research actually show?
Here is the rough picture from the published research, translated into human terms.
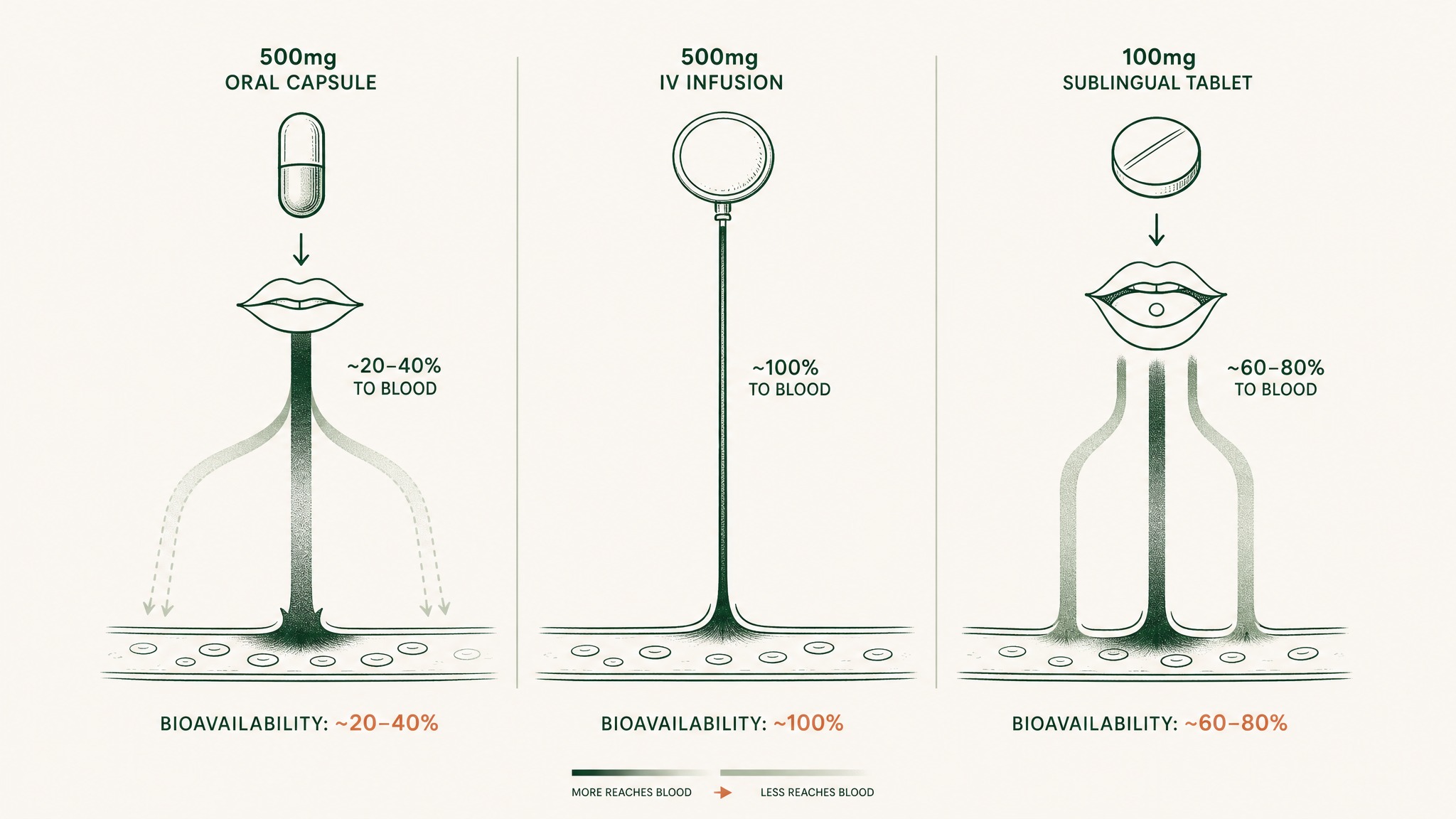
If you swallow a 500 mg oral NAD precursor capsule, your bloodstream does not see 500 mg. It sees a fraction, with the rest broken down or shunted into other pathways before it can do anything systemic. The exact fraction depends on the precursor, the formulation, and your own gut, but research suggests it sits well below half for direct NAD+ and only modestly higher for the better-absorbed precursors.
Why a smaller sublingual dose can deliver as much NAD to your blood as a much larger oral pill.
If a clinic infuses 500 mg of NAD into your vein over three hours, your bloodstream effectively sees the entire dose, spread out across the duration of the infusion. The bioavailability is essentially 100%, which is why injection advocates call it the gold standard for delivered dose.
If you take a 100 mg sublingual NAD tablet, the dose under your tongue is much smaller, but a much higher fraction reaches your bloodstream because it bypasses both the stomach and the first-pass liver clean-up.
Three intuition-level comparisons:
- A 1,000 mg oral capsule and a 100 mg sublingual tablet can deliver comparable amounts of NAD to the bloodstream, depending on the absorbed fraction of each.
- A single IV drip delivers more total NAD in one sitting than weeks of oral dosing, but it is a single-point exposure, not the steady tonic level that maintenance research has tracked.
- Frequency matters as much as peak. Sustained, regular exposure is what the longevity research has chased, not heroic one-off spikes.
For a deeper look at why most pills are competing on the wrong number, see our breakdown of peptide and supplement pill bioavailability.
Are NAD injections legal and what does a clinic visit involve?
Short answer: in the US, IV NAD is administered as an "off-label" or "compounded" therapy through licensed clinics, typically wellness clinics, IV bars, or naturopathic practices. It is not an FDA-approved product, which means it is not regulated like a prescription drug.
What a typical first visit looks like:
- Intake. Medical history, blood pressure, sometimes basic bloodwork. The clinic confirms you do not have contraindications (active cardiac issues, pregnancy, certain kidney conditions).
- Drip start. A nurse places the IV, mixes the NAD bag, and starts the drip slowly to see how you tolerate it.
- Two to four hours in a chair. Most clinics let you read, work or sleep through the drip. Faster drip rates produce more side effects, so they keep it slow.
- Aftercare. Mild fatigue is common for a few hours. Most people drive themselves home.
The reason clinics like to sell "protocols" of 4 to 10 sessions over a few weeks is that single drips rarely produce the sustained shift members are paying for. The plasma NAD bump from one session is largely cleared within days, which is the awkward middle ground that brought sublingual maintenance into the picture.
This is not medical advice. If you are considering IV NAD, the standard hedge is: talk to a clinician who knows your full history, not an IV bar receptionist.
How much does an NAD injection cost compared to a supplement protocol?
This is where the conversation gets uncomfortable for the injection side.
Rough US market pricing in 2026, drawn from publicly listed clinic menus and retail supplement prices:
| Route | Per dose | Per year (typical use) |
|---|---|---|
| IV NAD drip (single 500 mg session) | $400 to $1,000 | $4,800 to $24,000 (monthly maintenance) |
| IM NAD shot (clinic) | $50 to $150 | $1,800 to $7,200 (every 2 weeks) |
| Oral NAD precursor capsule (NMN/NR) | $1 to $3 per day | $400 to $1,100 |
| Sublingual NAD+ tablet | $1 to $4 per day | $400 to $1,500 |
| Direct-to-consumer subcutaneous NAD (rare, by prescription) | Varies | $2,000 to $6,000 |
The injection route's main cost is not the NAD itself; it is the clinic time, the nurse, the rent, and the chair you sit in. The supplement route's cost is essentially the active ingredient and the delivery substrate.
A few honest framings:
- For a "loading" experiment (try it for a month, see if you feel something): IV NAD is the highest-impact option and also the highest-cost one.
- For long-term maintenance (the way most longevity research has tracked NAD): a daily, well-delivered sublingual dose is closer to the protocol design the human trials have used.
- For convenience-first: oral capsules win on simplicity. They lose on delivered dose.
Users report that the financial math drives most people toward a hybrid: a clinic protocol to "feel something" up front, then a daily sublingual or oral routine to hold the line.
What does the research suggest about results from each route?
Honest answer: the human research on NAD itself is younger than the marketing makes it sound. Most of the strongest evidence is animal data. Most of the human data is short-term and uses precursors, not NAD itself.
What the human research has actually examined:
- Oral NR: Trammell and colleagues (2016) showed measurable rises in whole-blood NAD+ after single and repeated oral doses. Subsequent trials have replicated the blood-level shift but human outcome data remains limited.
- Oral NMN: Yoshino and colleagues (2021) reported that 250 mg daily for ten weeks in postmenopausal prediabetic women produced measurable shifts in muscle insulin sensitivity. The trial was small and outcome-focused, not a long-term lifespan study.
- IV NAD: Grant and colleagues (2019) ran a small pilot pharmacokinetic study using a slow IV infusion. They reported measurable shifts in plasma NAD+ metabolites during infusion, with the parent molecule and its metabolites tracking through the dosing window.
- Long-term outcomes for any route: no human lifespan trial exists, for any NAD product, by any route. Read every "anti-ageing" claim with that in mind.
What this means for choosing a route:
- The injection route has the cleanest pharmacokinetic story (high peak, full bioavailability) but the thinnest outcome story (small studies, no long-term human trials).
- The oral and sublingual routes have the thinnest pharmacokinetic story for direct NAD (low absorption) but a steadier, lower-cost maintenance profile that better matches how the precursor trials were actually run.
- Neither route is "proven to extend lifespan." The honest position is: the research suggests NAD biology matters, the human trials are still young, and the smart move is to pick the delivery route you can actually maintain.
For more on how to read the longevity literature without getting sold to, see our overview of supplements for longevity.
Who is each NAD route actually for?
This is where most "which one wins" debates collapse, because the two routes serve different jobs.
Pick the route that matches your goal, not the one with the loudest marketing.

A daily sublingual tablet fits seamlessly into a sustainable long-term wellness routine.
- NAD IV / IM injection is best fit for someone who wants a short, high-impact intervention, has the budget for clinic visits, and is comfortable with the time commitment and mild side effects. It is the right tool for a four-to-eight-session "loading" protocol or for a one-off "see what high NAD feels like" experiment.
- Sublingual NAD supplement is best fit for someone who wants a daily, sustained, lifestyle-compatible protocol. Members experience this route as low-friction (a tablet under the tongue, no clinic, no needle) which is exactly what makes long-term maintenance feasible.
- Oral capsule NAD precursor is best fit for someone who wants the cheapest possible entry point and is willing to accept that most of the labelled dose will not reach systemic circulation. This is the simplest route, with the worst delivered-dose efficiency.
- A hybrid protocol is what most longevity-leaning members eventually land on: an upfront IV course if budget allows, then daily sublingual maintenance to hold steady plasma levels. The injection is the loading phase; the supplement is the maintenance phase.
In our protocol design, we have found that the people who get sustained results are not the ones who paid the most. They are the ones who picked a route they could actually do every day, for years, without quitting.
Frequently asked questions
Is an NAD injection better than an NAD supplement?
"Better" depends on what you mean. For raw bioavailability, an IV injection delivers essentially 100% of the dose; an oral supplement delivers a fraction. For sustained daily exposure (which is closer to how the human trials are run), a well-delivered sublingual dose is much easier to maintain. The two routes solve different problems.
How long does an NAD IV drip take?
Two to four hours per session is typical. The drip has to run slowly because faster infusion rates produce chest pressure, flushing and nausea. Clinics build their schedules around the slow rate.
Are IV NAD treatments FDA-approved?
No. IV NAD is administered through licensed clinics as a compounded therapy. It is not an FDA-approved drug product for any specific indication. That does not mean it is illegal; it means it is not regulated like a prescription medicine.
Can you absorb any NAD from swallowing a capsule?
Some, but much less than the label suggests. Oral direct NAD is largely degraded in the gut. Oral NAD precursors (NR, NMN, niacinamide) survive better and feed NAD synthesis in cells, but the absorbed fraction is still well below 100%. Research suggests sublingual delivery captures more of the labelled dose than swallowing.
Is sublingual NAD as effective as an injection?
The dose is much smaller, but the absorbed fraction is much higher. A daily sublingual protocol cannot match the single-session peak of an IV drip, but it can sustain higher steady-state blood levels than an equivalent oral capsule routine, at a fraction of the cost of a clinic.
Are NAD injections safe?
In the published literature, IV NAD has been administered to small numbers of human volunteers without serious adverse events when delivered slowly. The common side effects (chest pressure, nausea, flushing) are dose- and rate-related. This is not a tested-at-scale therapy and is not medical advice. Talk to a clinician who knows your history.
What is the cheapest way to raise NAD?
The cheapest route is a daily oral NAD precursor (NR, NMN, or niacinamide) at $1 to $3 per day. The trade-off is that much of the labelled dose does not reach systemic circulation. Sublingual delivery sits in the middle on price and delivers more of what you paid for.
Key Takeaways
- NAD injections (IV or IM) bypass the gut entirely and deliver close to 100% bioavailability. They also cost $400 to $1,000 per clinic session and require a 2-to-4-hour appointment.
- Oral NAD supplements (capsules) lose most of the labelled dose to stomach acid, gut enzymes, and first-pass liver metabolism. The brands switched to precursors (NMN, NR, niacinamide) because direct oral NAD survives the gut poorly.
- Sublingual NAD sits in the middle. A small dose under the tongue absorbs through the mouth lining, bypassing the stomach and first-pass metabolism, at a fraction of the cost of an injection.
- The strongest human research has tracked oral precursors (Trammell 2016; Yoshino 2021) and a small IV NAD pharmacokinetic study (Grant 2019). No human lifespan trial exists for any route.
- Pick the route you can actually maintain. Many longevity-leaning members combine an upfront IV loading course with daily sublingual maintenance.
- This article is for research purposes only. Talk to your physician before adjusting any supplement or starting any injectable protocol.
References
- Trammell SAJ, Schmidt MS, Weidemann BJ, et al. (2016). Nicotinamide riboside in humans: pharmacokinetic and bioavailability findings. Nature Communications. https://doi.org/10.1038/ncomms12948. Retrieved 2026-06-29.
- Yoshino M, Yoshino J, Kayser BD, et al. (2021). Nicotinamide mononucleotide and muscle insulin sensitivity in prediabetic women: clinical trial findings. Science. https://doi.org/10.1126/science.abe9985. Retrieved 2026-06-29.
- Grant R, Berg J, Mestayer R, et al. (2019). Intravenous NAD+ pharmacokinetics in humans: first-in-human pilot study. Frontiers in Aging Neuroscience. https://doi.org/10.3389/fnagi.2019.00257. Retrieved 2026-06-29.
- Massudi H, Grant R, Braidy N, Guest J, Farnsworth B, Guillemin GJ. (2012). Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLoS ONE. https://doi.org/10.1371/journal.pone.0042357. Retrieved 2026-06-29.
- Mills KF, Yoshida S, Stein LR, et al. (2016). Long-term nicotinamide mononucleotide administration in mice: age-associated physiological-decline study. Cell Metabolism. https://doi.org/10.1016/j.cmet.2016.09.013. Retrieved 2026-06-29.
- Airhart SE, Shireman LM, Risler LJ, et al. (2017). An open-label, non-randomized study of the pharmacokinetics of the nutritional supplement nicotinamide riboside in human volunteers. PLoS ONE. https://doi.org/10.1371/journal.pone.0186459. Retrieved 2026-06-29.
Ready to move past the clinic vs capsule debate? Explore VERO LEGACY, our sublingual NAD+ protocol →
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.