
What TB-500 actually is — a synthetic seven-amino-acid fragment of Thymosin Beta-4 — plus the parent-vs-fragment distinction that reshapes every research claim. Research purposes only.
Ask ten people what TB-500 is and you'll get ten different answers. A tissue-repair peptide. A muscle-recovery compound. A cousin of BPC-157. A racehorse-doping agent. All of those describe something the research community has studied. None of them actually answer the question.
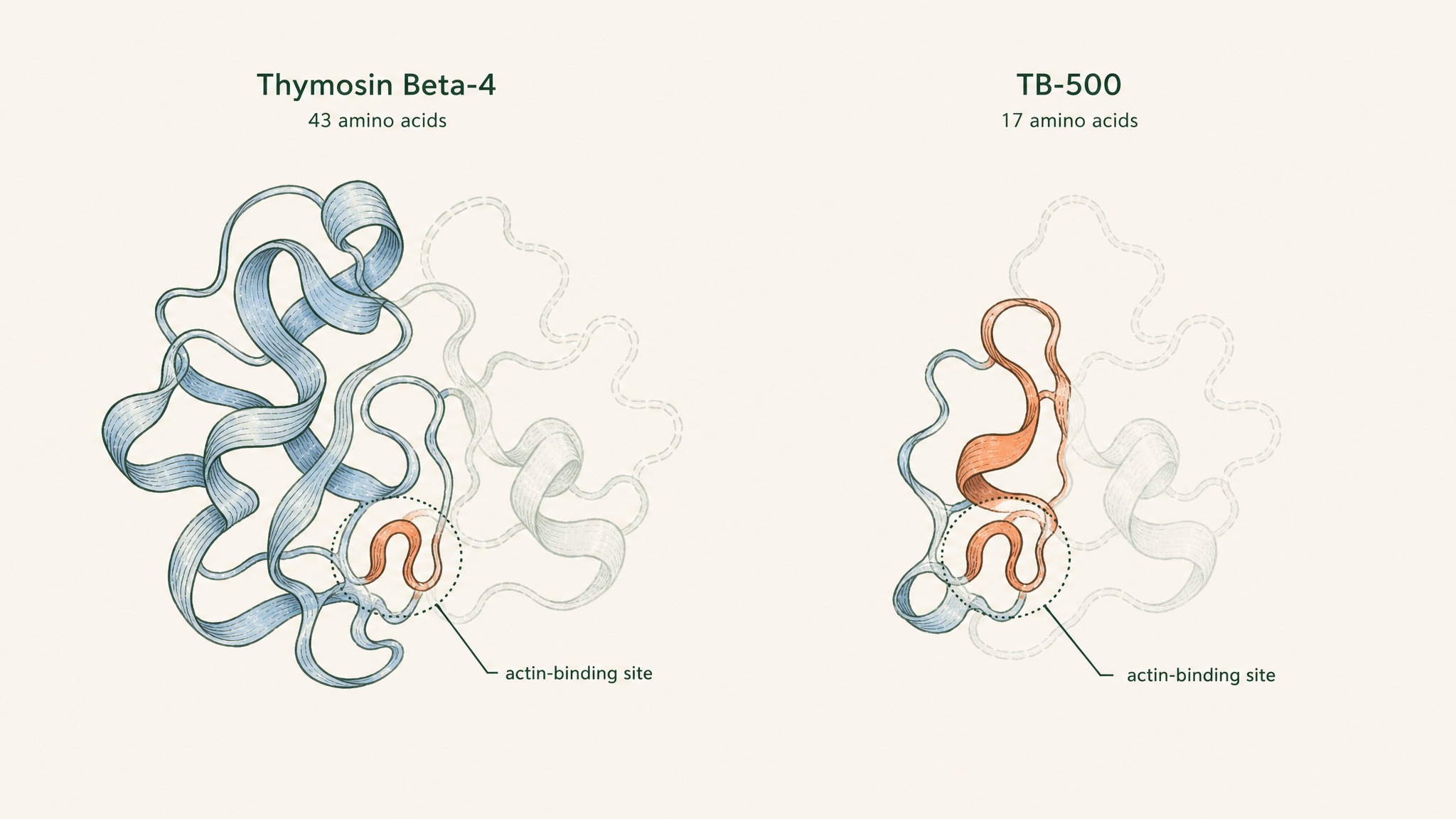
Here's the short version. TB-500 is a synthetic seven-amino-acid fragment lifted out of a much larger, naturally-occurring human protein called Thymosin Beta-4. That's the molecule. Everything else (the tissue-repair claims, the athlete testing, the vials sold on research-supply websites) is a story built on top of that one fact.
This guide unpacks what the fragment actually is, what the parent protein does inside your body, and why the difference between the two is the most under-discussed thing in the whole space. For the benefit-by-benefit evidence map, see our TB-500 benefits guide. If you want a sober framework for thinking about tissue-repair peptides in the first place, VERO's RESTORE protocol is where we do that work. All content is published for research purposes only.
Key Takeaways
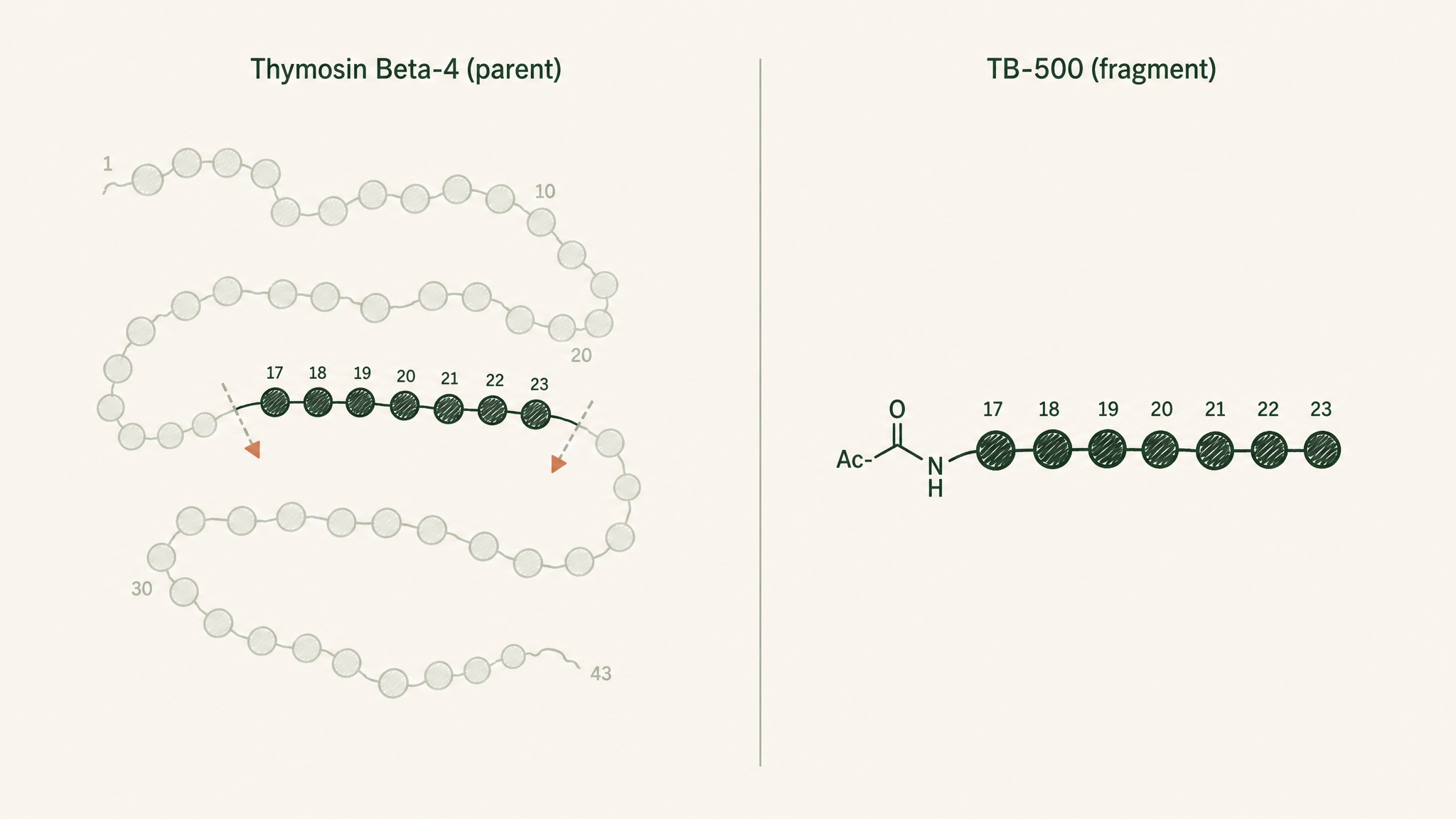
- TB-500 is a lab-made peptide fragment: seven amino acids long, sequence Ac-LKKTETQ, positions 17–23 of a larger protein called Thymosin Beta-4.
- Thymosin Beta-4 is the parent. It's the 43-amino-acid protein your platelets carry and release at injury sites, and it's what most of the "TB-500 research" is actually studying.
- Doping-lab papers have confirmed that commercial TB-500 vials contain the fragment, not the full parent protein.
- No human disease has TB-500 as an approved therapy. It sits on WADA's Prohibited List and is sold as a research peptide only.
- Almost every mechanism you'll read about was mapped on the parent molecule, not on the fragment on your bench.
So What Is TB-500, Really?
Skip the marketing pages for a second. In a doping-control lab, TB-500 has a specific chemical identity, and it isn't what most consumer-facing sites claim it to be.
Two papers made that identification concrete:
- Esposito 2012 (PMID 22962027, Drug Test Analysis) — synthesised and characterised the N-acetylated 17–23 fragment of Thymosin Beta-4, then matched it against commercial TB-500 product. The vials contained the fragment. Not the parent protein.
- Ho 2012 (PMID 23084823, Journal of Chromatography A) — followed the same fragment into racehorse urine and plasma after TB-500 was administered, developing detection methods sensitive to 0.01 nanograms per millilitre.
- The consequence — every claim you read about "TB-500" is grounded in a paper that studied either the fragment or the parent. Most studied the parent. Marketing rarely says so.
Think of it like a poster print of the Mona Lisa. You can hang it up, call it a Mona Lisa, and it does depict the same face. But the paint, the aging, the brushstrokes Da Vinci put in? That's the original in the Louvre.
TB-500 is the poster. Thymosin Beta-4 is the painting.
Every time a supplement site or forum post says "TB-500 does X", the honest question is whether the underlying paper studied the fragment or the parent. The distinction sounds like hair-splitting. It changes what "does X" actually means.
Meet The Parent: Thymosin Beta-4
Now let's zoom out to the molecule TB-500 came from. Thymosin Beta-4 (usually shortened to Tβ4) is a 43-amino-acid protein your body makes on its own. It's one of the most abundant proteins in your platelets — the tiny cell fragments that arrive at a cut within seconds.
Here's the picture worth carrying. Think of Tβ4 as the emergency envelope your platelets rip open the moment tissue gets damaged. Inside that envelope is a signalling molecule that talks to nearby cells and says "get the repair crew moving."
A platelet dumps its pre-loaded Tβ4 into a fresh wound within seconds of injury.
Three plain-English facts that put Tβ4 in context:
- It's small. Most proteins are hundreds or thousands of amino acids long; Tβ4 is 43. That size lets it move through tissue easily.
- It's ancient. Versions of Tβ4 show up in animals across the evolutionary tree, which usually flags a molecule doing something biologically important.
- It's stored, not made on demand. Your platelets pre-load it so the release can happen the instant an injury opens up.
That last point matters. The reason wound sites see a spike in Tβ4 within minutes isn't because your genes suddenly start pumping it out. The pre-loaded reserves get dumped into the wound the way a canister of gas gets popped, and the surrounding cells respond to that signal.
If you've ever wondered why researchers keep circling back to this molecule, it's because they describe it as sitting at a point in the repair cascade that fires earlier than most of the others.
What Thymosin Beta-4 Does Inside Your Body
The mechanism the biochemistry papers describe is deceptively simple: Tβ4 binds a molecule called G-actin. Actin is the scaffolding your cells build and rebuild constantly. G-actin is the loose, unpolymerised form. F-actin is when those units link into filaments.
Here's the analogy that keeps this straight. Actin is Lego bricks. G-actin is the loose bricks in the bin. F-actin is the model you've built out of them. Tβ4 is the loose-brick holder — it grabs G-actin bricks and keeps them in reserve, ready for the moment a cell needs to build fast.
Tβ4 holds loose actin bricks in reserve so cells can rebuild their scaffolding fast during migration.
Why does that matter for the repair story? Two reasons:
- Cells move by rebuilding actin. When immune cells crawl into a wound, when a keratinocyte migrates across a cut, when a heart-muscle cell repositions itself, the actin scaffolding gets torn down and rebuilt at the leading edge.
- Rapid rebuild needs a reserve. If the loose G-actin bricks are all floating free, they polymerise on their own before a cell can direct where they should go. Tβ4 is one of the sequestering proteins that holds them ready.
That's the most consistently documented part of the picture. Everything downstream (wound-closure observations, myoblast-migration signals, cardiac-cell survival work) traces back through actin dynamics as one of the connecting threads. There are other interactions the papers describe, including inflammatory signalling and integrin-linked kinase in cardiac tissue, but the actin story is the most reproduced one across preclinical research.
The Fragment Question: Why It Won't Go Away
Here's where "what is TB-500" gets sticky. If you scan the actual research base — dozens of papers on Thymosin Beta-4 across skin, eyes, heart, and muscle — almost all of it was done on the full parent protein. The 43-amino-acid molecule. What you can buy as a research vial is not that.
Three details that most consumer coverage skips:
- The fragment covers positions 17–23. That's a specific stretch inside the parent, and it happens to be a region researchers identified as an "actin-binding motif" — the piece that grabs G-actin bricks. So the fragment does share at least one of the parent's core functions.
- The parent has more than one active region. Thymosin Beta-4 also carries surfaces that engage inflammatory signalling, immune-cell recruitment, and cardiac-specific pathways. Those don't necessarily sit inside the 17–23 window.
- Fragment-specific papers are the minority. When you audit the literature, papers labelled "TB-500" or explicitly using the LKKTETQ sequence are a small slice of the total. Most "Tβ4" work uses the full molecule.
Users report that "TB-500 helped my recovery" is a common refrain online. What research suggests, in the peer-reviewed sense, applies mostly to the parent. The two claims aren't the same claim, even though they read that way in a forum post.
The Research Trail: A Quick Tour
To make the fragment-vs-parent point concrete, here are the papers that put Thymosin Beta-4 on the research map. Every one of them used the parent molecule, not the LKKTETQ fragment.
- Malinda 1999 (PMID 10469335, Journal of Investigative Dermatology) — in a rat wound model, Tβ4 was linked to faster reepithelialization (the skin closing back over the raw area) with measurements 42% higher at day 4 and up to 61% higher at day 7 versus saline controls.
- Sosne 2001 (PMID 11311052, Experimental Eye Research) — the founding paper describing Tβ4's role in corneal wound closure in an animal model, with anti-inflammatory signalling as part of the observed profile.
- Bock-Marquette 2004 (PMID 15565145, Nature) — in a mouse coronary-ligation model of heart attack, Tβ4 activated the integrin-linked kinase and Akt survival pathways, and treated hearts showed better measured function.
Each paper landed in a serious journal. Each used the parent molecule. Members experience of TB-500 vials is grounded in the general biology those papers established, but the fragment-to-parent leap is one the papers themselves don't make.
The Regulatory Reality
Here's the part that rarely makes the forum posts. TB-500 isn't a scheduled controlled substance, isn't an approved drug, and isn't a supplement. It sits in a category of its own, and two facts define that category.
- No approval, anywhere. No major regulator (FDA in the US, Health Canada, EMA in Europe) has approved TB-500 for any human condition. Vials are labelled "for research use only" for a reason.
- WADA prohibits it. The World Anti-Doping Agency lists Thymosin Beta-4 and related peptides on its Prohibited List. That's the direct reason doping-lab papers like Esposito 2012 and Ho 2012 exist. Testing labs needed detection methods for a compound athletes started using off-label.
Practical consequence: anyone framing TB-500 as "just a repair peptide" is skipping the two facts above. It's a compound with an active research profile, an unresolved regulatory status, and a positive-drug-test consequence for anyone competing under a WADA-compliant framework.
VERO does not sell TB-500. Nothing in this article is a recommendation to source, buy, or self-administer it. It's here because the topic deserves an honest answer instead of a hype list.
The Frequently Asked Version
Is TB-500 the same as Thymosin Beta-4?
No. TB-500 is a synthetic seven-amino-acid fragment (Ac-LKKTETQ) taken from positions 17–23 of Thymosin Beta-4. The parent protein is 43 amino acids long. Most of the peer-reviewed research is on the parent, not the fragment.
Is TB-500 FDA-approved?
No. It has no approved human indication with any major regulator. Research vials are labelled for laboratory use only.
Why is TB-500 banned in sport?
It's covered by the World Anti-Doping Agency's Prohibited List. Detection methods for it in athlete samples exist because of that ban — the Ho 2012 paper walks through how a regulatory lab actually finds it in urine and plasma.
What does TB-500 do at the biochemical level?
The parent Thymosin Beta-4 sequesters G-actin and is involved in early signalling at injury sites, and the 17–23 fragment carries one of the parent's actin-binding motifs. That much is documented in preclinical research. Whether the fragment reproduces every function of the parent isn't something the literature answers cleanly.
Where can I read the actual research?
Start with the peer-reviewed papers linked above (Esposito, Ho, Malinda, Sosne, Bock-Marquette). Each PMID resolves to the abstract on PubMed, and most of the abstracts are open-access.
Where VERO Sits
VERO builds protocols around peptides where the research is deeper, the delivery is cleaner, and the regulatory picture is unambiguous. TB-500 isn't currently one of those. The evidence base is real but preclinical-heavy, the fragment-vs-parent question is unresolved in the consumer-facing space, and the WADA status makes it a poor fit for anyone competing.
What VERO does build is a sublingually-delivered, structured peptide framework aimed at recovery and daily function. That's the RESTORE protocol — designed for the same underlying goal (better repair, better recovery) using compounds with cleaner data and no positive-test risk. The delivery layer, VERISORB sublingual technology, is a separate story worth the read.
The three things worth carrying away:
- The word "TB-500" refers to a specific fragment, not the parent Thymosin Beta-4. That distinction is the whole story.
- The research base is real, but the fragment-to-parent extrapolation is where consumer-facing coverage overreaches.
- A structured protocol with clean regulatory status beats a research vial with a marketing label every time.
For research purposes only. This article is editorial content about peptide science, not medical advice, and nothing here is a recommendation to source, use, or self-administer TB-500.
Want a recovery protocol grounded in peptides with real evidence and a clean regulatory picture? Explore the RESTORE protocol →
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.