Evidence-graded look at TB-500 benefits: wound healing, muscle recovery, cardiac and corneal research, and the parent-vs-fragment gap most write-ups skip. Research purposes only.
Search "TB-500 benefits" and you'll get a wall of claims: wounds, tendons, hearts, hair, joints — as if one small research peptide covered every recovery box a person could tick. Some of that is close to what the research says. A lot of it is a game of telephone from decades of work on a different molecule.
This guide is the honest version — what's actually in the papers, what's still animal-only, and what changes when you look at the fragment researchers hold versus the parent protein everyone keeps citing. If you want a structured, evidence-graded way to think about tissue-repair research, the framing behind the RESTORE protocol is where we start, because it's built to separate claim depth from claim volume.
All content is published for research purposes only. TB-500 is not an FDA-approved drug, and this article is not medical advice.
Key Takeaways
- Almost every "TB-500 benefit" you'll read is really a benefit of Thymosin Beta-4 — the full 43-amino-acid parent protein — not the 7-amino-acid fragment sold in research vials.
- The strongest, most-replicated finding is skin wound healing in animals, with human data limited to two small phase 2 trials in stasis and pressure ulcers.
- Cardiac, corneal, and muscle-regeneration data are real but almost entirely animal or cell-culture work — no approved human indication.
- TB-500 is not FDA-approved and is on WADA's Prohibited List. It is sold and studied as a research peptide only.
- The gap between "what the parent molecule does" and "what the fragment on your bench does" is the single most under-discussed part of this space.
What TB-500 Actually Is — Because The Answer Changes Every Benefit Claim
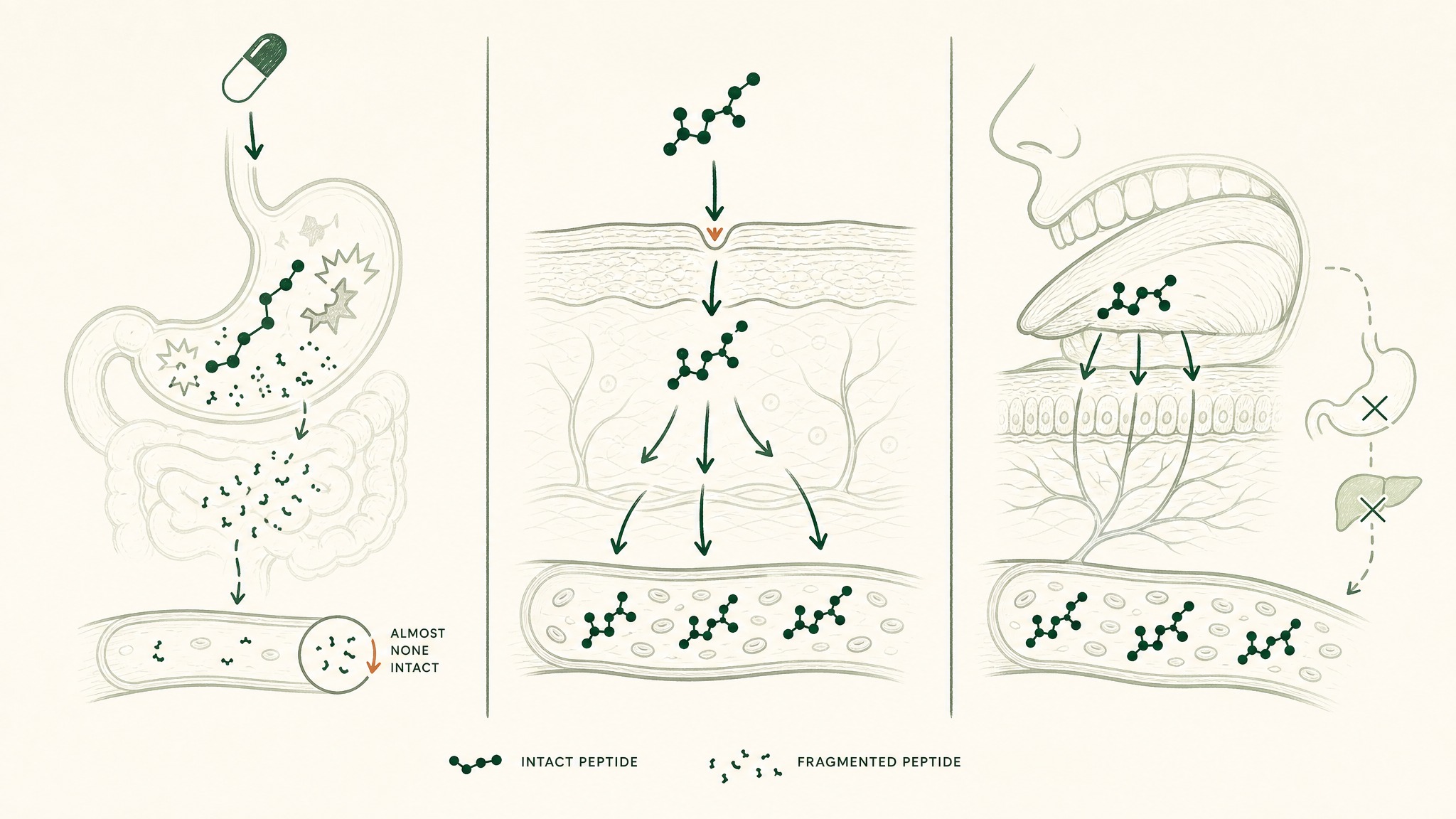
Before we grade any TB-500 benefit, one distinction has to sit at the front. TB-500 is a short synthetic fragment — seven amino acids long, sequence Ac-LKKTETQ, positions 17-23 of a much larger molecule called Thymosin Beta-4. The parent protein is 43 amino acids and made by your own body, especially by your platelets when tissue gets damaged.
Here's the analogy that helps: Thymosin Beta-4 is the whole toolbox your body sends to a repair site. TB-500 is one wrench pulled from that toolbox, mass-produced, and sold on its own. It might do a specific job well, but it won't do the whole job the toolbox does.
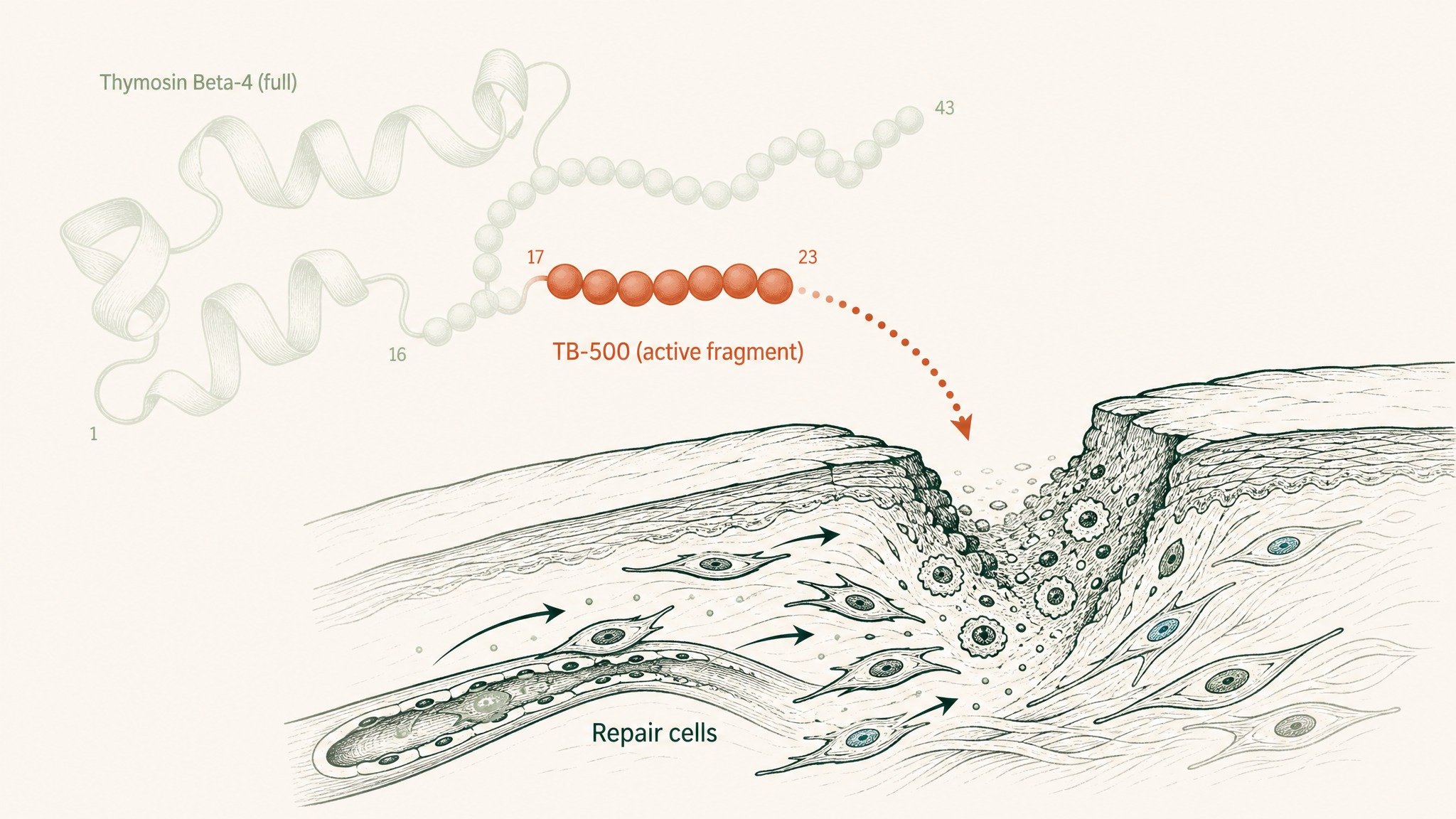
TB-500 is a seven-amino-acid fragment extracted from the much larger Thymosin Beta-4 protein.
That's not speculation — it's what a doping-lab mass-spectrometry paper actually found when it analysed commercial TB-500 vials:
- Esposito 2012 (PMID 22962027, Drug Test Anal) identified the contents of TB-500 as N-acetylated LKKTETQ — the 17-23 fragment, not the full parent.
- Ho 2012 (PMID 23084823, J Chromatogr A) then confirmed the same fragment showed up in racehorse urine and plasma after TB-500 administration.
Every benefit claim below hinges on this. When the paper studied full Thymosin Beta-4, we say so. When it studied the fragment, we say so. That distinction is what keeps a research article honest.
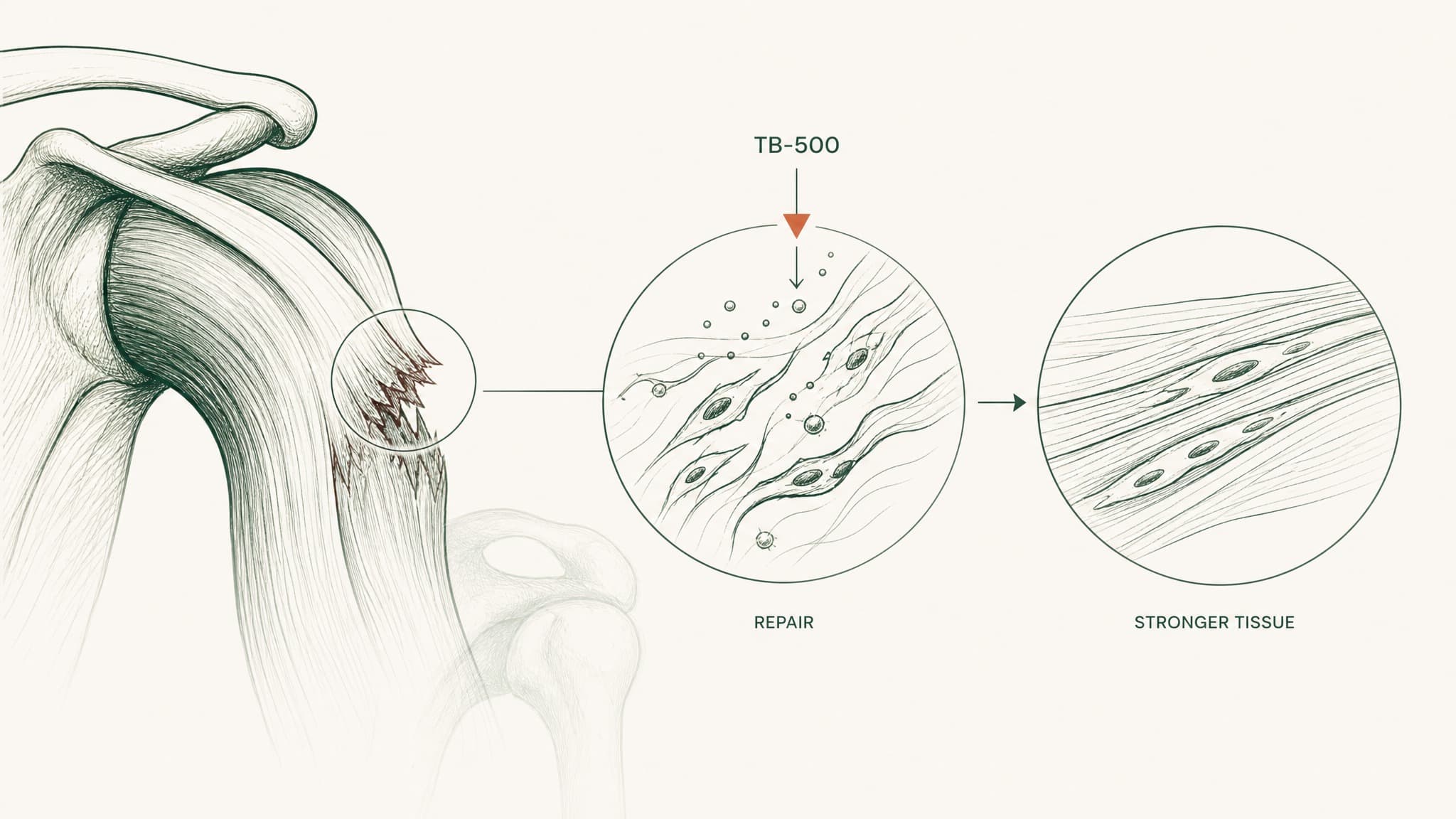
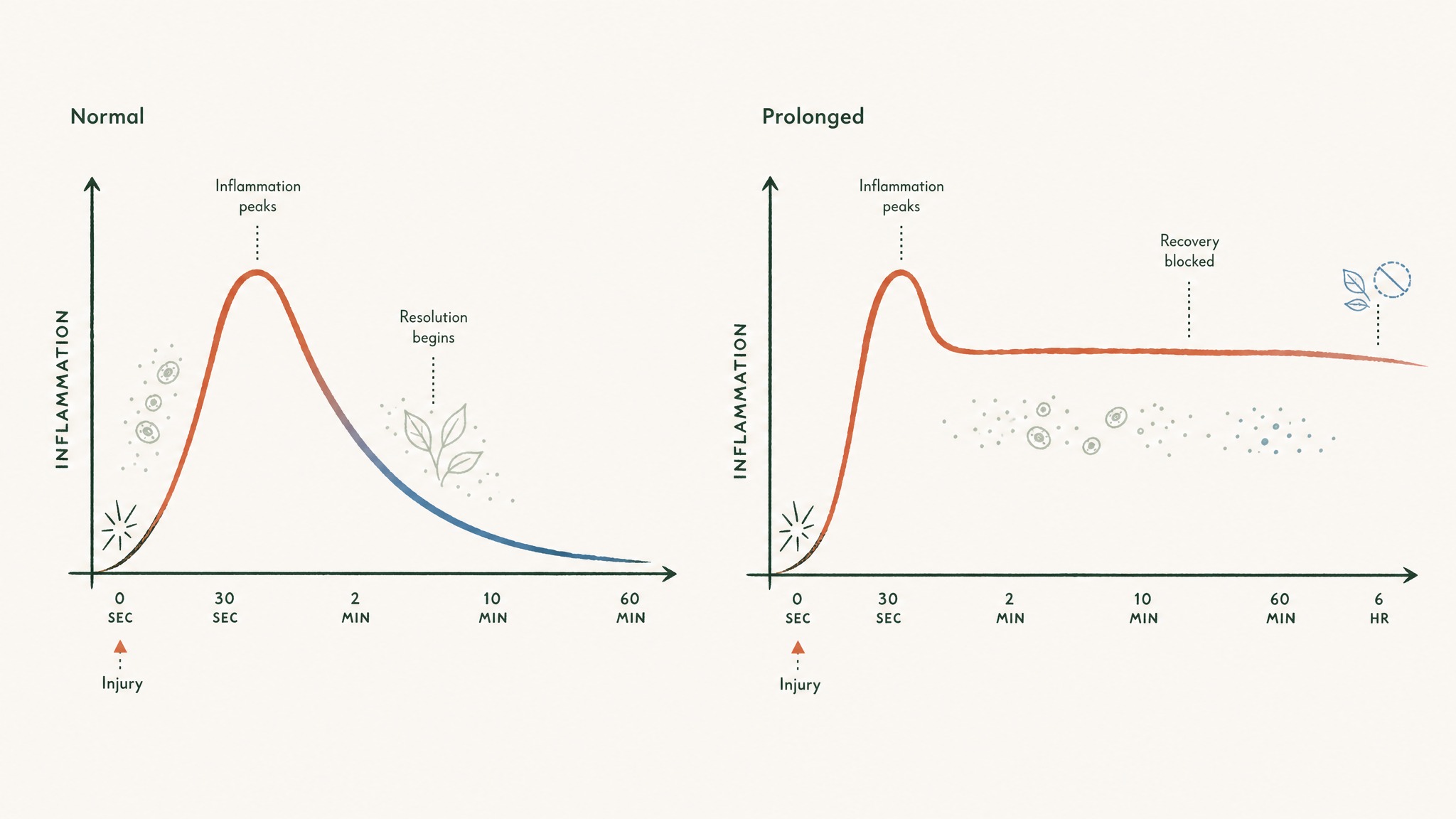
The Skin And Wound Healing Data — The Strongest Case
This is the domain where the evidence is deepest, and it's the one users report first when they talk about TB-500. Think of an injured patch of skin as a construction site with three crews: cleanup, framing, and finishing. Thymosin Beta-4 seems to speed up all three at once by acting as a chemical whistle that pulls the crews in faster and keeps them working longer.
The two anchor papers on skin:
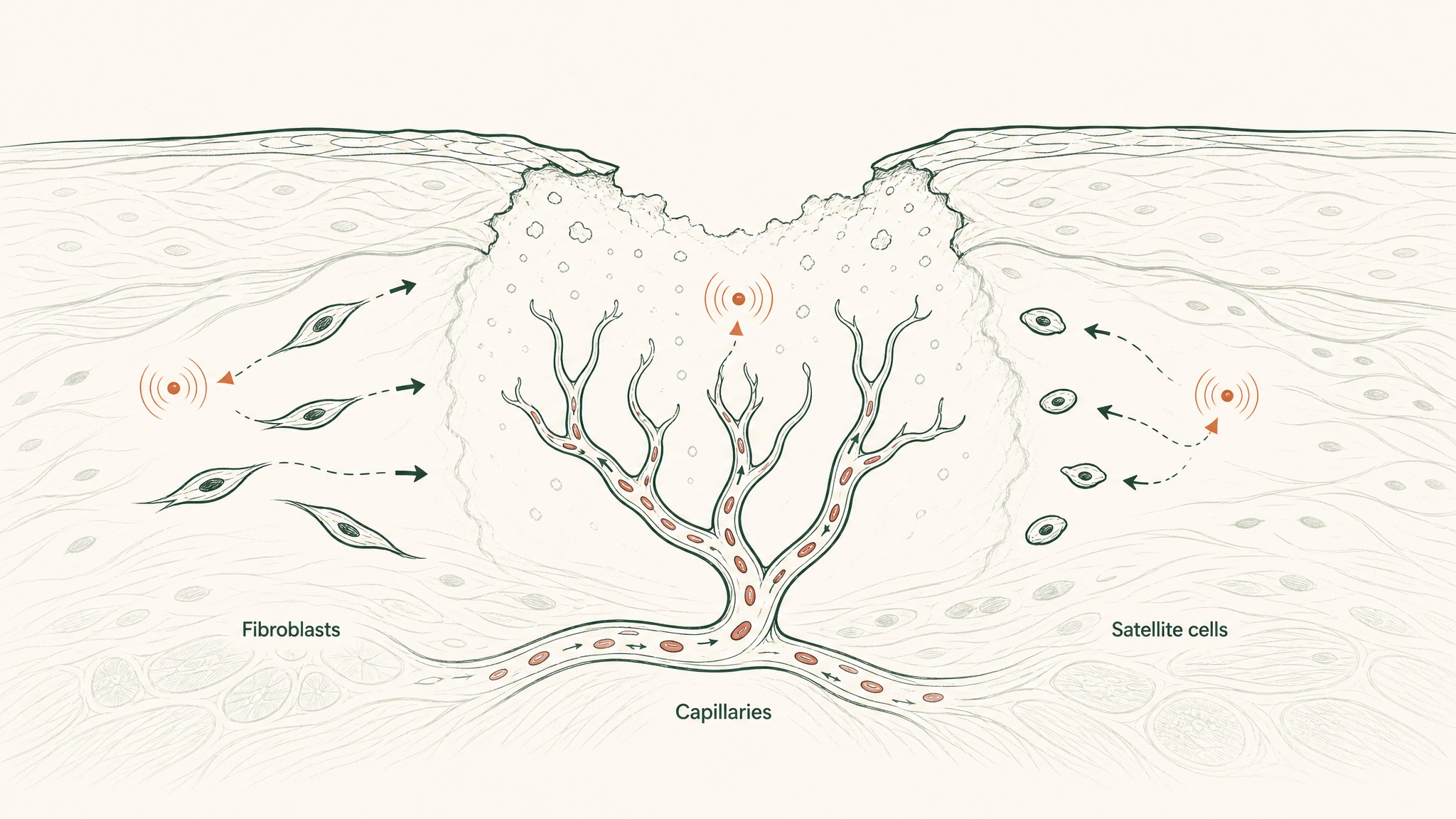
Three wound-— crews working simultaneously: skin cells closing the gap, collagen reinforcing underneath, and new blood vessels forming.
- Malinda 1999 (PMID 10469335, J Invest Dermatol) — Thymosin Beta-4 applied topically or by injection into rats sped up wound "reepithelialization" (the skin closing back over the raw area) by 42% at day 4 and up to 61% at day 7 versus saline controls. Treated wounds also showed more collagen laid down and more new blood vessels forming.
- Treadwell 2012 (PMID 23050815, Ann N Y Acad Sci) — a review paper that includes the closest thing to human data: two small phase 2 trials, one in venous stasis ulcers and one in pressure ulcers, where Thymosin Beta-4 accelerated healing by "almost a month" among the patients who did heal.
Read that carefully — "among the patients who did heal." It didn't rescue wounds that weren't already improving. It shortened the timeline for wounds already trending toward closure.
Both anchor papers are on the full parent molecule, not the fragment. If you're pattern-matching from Malinda to a research vial in front of you, you're extrapolating across a molecular boundary the papers themselves don't cross.
The Muscle And Tendon Angle — Popular Claim, Thinner Evidence
This is the benefit domain that drives most of the athletic and gym-forum interest, and it's also where the gap between claim and evidence is widest. The muscle-repair story rests on a small number of animal papers, and the exciting ones came out of injury models where researchers deliberately damaged a muscle to see what happened next.
The clearest paper:
Myoblasts migrate toward a muscle injury site when TB-500 signals them to begin repair.
- Tokura 2011 (PMID 20880960, J Biochem) — in mice, Thymosin Beta-4 expression jumped up in the first days of regenerating muscle fibres after injury. Both the natural and the modified form of Tβ4 pulled myoblasts (the cells that build new muscle fibres) toward the injury site and sped up wound closure in culture.
The mechanism is intuitive: myoblasts are the workers that rebuild muscle tissue; Tβ4 is one of the signals that tells them where to go. What we don't have is a human muscle-injury trial. No paper follows a group of humans with hamstring tears through a Tβ4 or TB-500 protocol and measures return-to-play times.
Internet-forum reports of faster recovery are not a substitute for controlled human trials. The biology has real support in animal work — what's missing is the specific claim that a research peptide fragment reliably shortens human soft-tissue injury timelines.
What The Cardiac Studies Actually Found
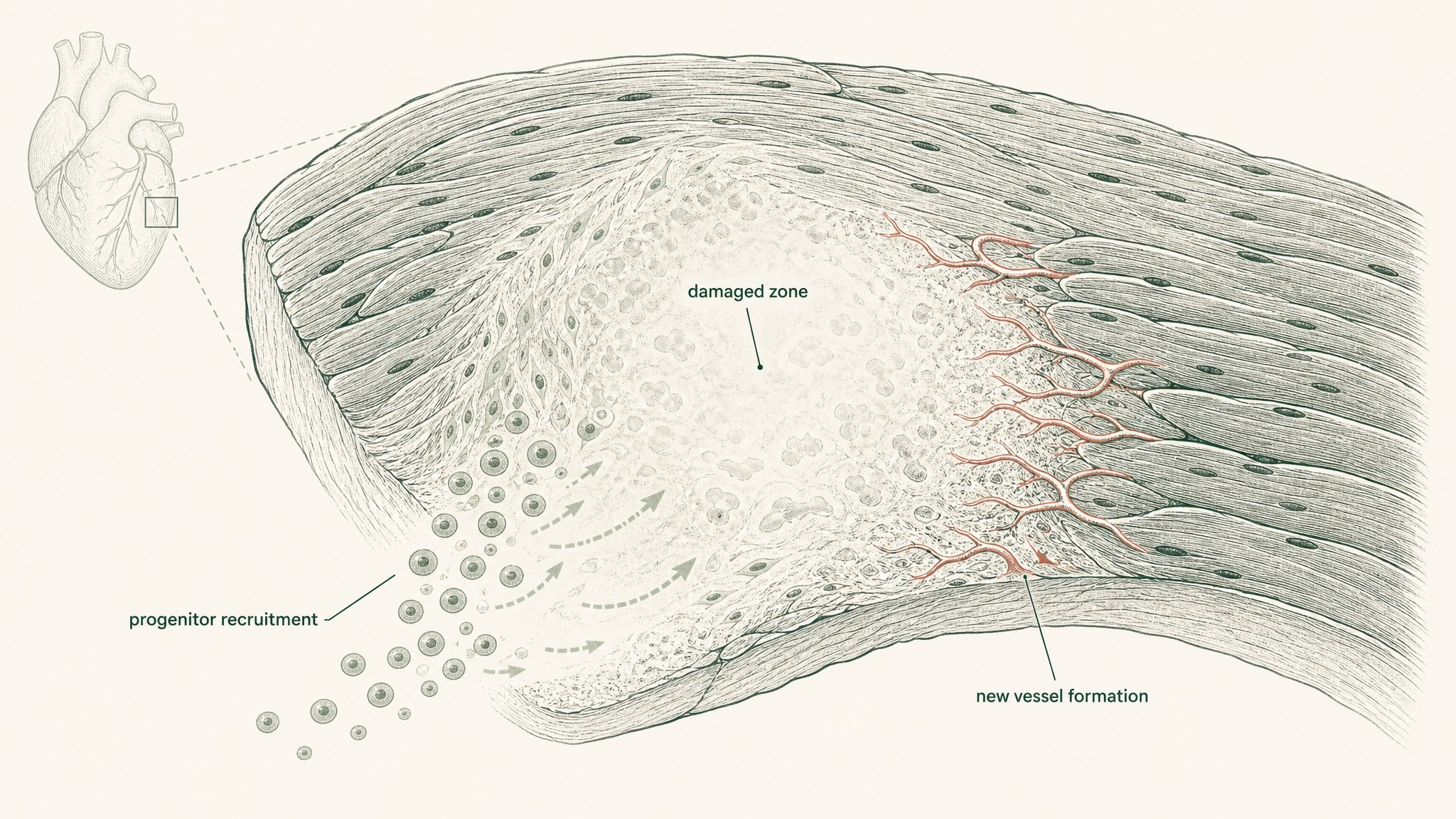
The cardiac work is the most attention-grabbing entry in the whole TB-500 story, because it hints at something bigger than wound care. Imagine a heart attack as a section of the electrical grid going dark — cells starved of oxygen die, and the surrounding tissue scars over into a patch that no longer conducts properly. The claim on the table is that Thymosin Beta-4 can keep more of the grid alive during that first blackout.
The paper that put this on the map:
How a heart attack creates a dead zone that stops electrical signals from traveling through the heart wall.
- Bock-Marquette 2004 (PMID 15565145, Nature) — in mice with coronary artery ligation (a lab model of heart attack), Thymosin Beta-4 activated two survival signals inside cardiac cells (a protein complex called integrin-linked kinase, or ILK, and a downstream signal called Akt). Treated hearts had more surviving muscle cells early and better measured heart function later.
That is a big-deal result in a top journal, and it's also — and this matters — a mouse model. No approved human cardiac indication exists for Thymosin Beta-4 or for TB-500. What research suggests is a genuinely interesting mechanism; what regulators have not approved is a therapy.
The nuance: the Nature paper worked on the full parent molecule, and the ILK/Akt pathway is triggered by parts of the parent that may or may not be preserved in the 17-23 fragment. Fragment-specific cardiac data is thinner than the headline suggests.
Corneal Healing — Where Human Data Is Strongest Outside The Skin
Eyes are quietly the domain where Thymosin Beta-4 has traveled furthest into clinical work. The cornea (the clear window at the front of your eye) is a delicate tissue that reveals damage fast and heals slowly — perfect terrain to study a repair molecule.
- Sosne 2001 (PMID 11311052, Exp Eye Res) — the founding paper showing thymosin beta 4 promotes corneal wound healing in vivo and dials down local inflammation.
The cornea's layered surface cells and how quickly visible damage appears there.
That paper opened the door to a decade-plus of eye-specific work — mostly on the parent Tβ4 — culminating in clinical development for conditions like neurotrophic keratopathy and dry eye. The eye is one of the few surfaces where research on this molecule has reliably reached actual humans in trial settings, not just cell dishes.
For the TB-500 buyer, though, the same caveat lands hard: the ophthalmology work is on the full molecule. The fragment isn't a shortcut around a decade of clinical development.
The Big Regulatory Caveat: Why You Won't Find TB-500 In A Pharmacy
TB-500 isn't scheduled the way opioids are, and it isn't approved the way a prescription drug is. It sits in a middle zone that's confusing on purpose. Two facts define that zone.
- It's not FDA-approved for any indication. No human disease has TB-500 as a licensed therapy. Vials sold in the research-peptide market are labelled for laboratory use only.
- It's on WADA's Prohibited List. Thymosin Beta-4 and related peptides were added under section S2.5, which is why the doping-control literature (Esposito, Ho) even exists. Elite athletes get tested for exactly this compound.
Practical translation:
- Buying TB-500 is not the same as buying a supplement or a prescription drug.
- Any coach, personal trainer, or online seller who tells you it's "just a repair peptide" is glossing over both facts above.
- If you're a competitive athlete tested under a WADA-compliant framework, this compound will show up.
VERO does not sell TB-500. Nothing in this article should be read as a suggestion to source, buy, or use it. It's here because researchers, clinicians, and curious readers deserve an accurate benefit map instead of a hype list.
How TB-500 Compares To BPC-157 — The Question Everyone Asks
TB-500 and BPC-157 sit next to each other on every "healing peptide" listicle, and readers reasonably want to know how they differ. The short answer: they're studied in a lot of the same injury contexts, but the evidence stacks look different.
- BPC-157 has more repeated rodent work across gut, tendon, and joint models, with a small amount of human observational data. See our BPC-157 benefits guide for the full grading.
- TB-500 / Thymosin Beta-4 has fewer replications per domain, but reaches slightly further into human trial territory in skin and eye work.
TB-500 and BPC-157 studied in different injury contexts, with different evidence depths.
One is not "better" than the other in the abstract. What they share is the same core problem: most of the exciting data is preclinical, and the fragment you can actually get your hands on isn't always the molecule the papers used.
If you're trying to think about tissue-repair research the right way, the useful move isn't picking a peptide first. It's picking a framework — one that grades evidence, respects the parent-vs-fragment distinction, and doesn't oversell mouse results as human ones.
Where VERO Stands On TB-500 — And What We Actually Build
VERO's protocols are built on peptides where the sublingual VERISORB delivery system has meaningful data and where the underlying safety and regulatory position is clear. TB-500 does not currently sit inside a VERO protocol — because the human evidence is thin, the fragment-vs-parent gap is unresolved, and the regulatory status is what it is.
What VERO does build is a structured, sublingual-delivered peptide framework aimed at the same underlying goal — better daily recovery — through compounds with cleaner data and cleaner status. That's the RESTORE protocol.
The three things worth taking away:
- The TB-500 benefit map is real, but shallower and more parent-molecule-shaped than most write-ups admit.
- Skin and eye work reach humans; muscle, tendon, and cardiac work mostly don't.
- A structured protocol built around evidence and delivery beats a research vial with a marketing label every time.
For research purposes only. This article is editorial content about peptide science, not medical advice, and nothing here is a recommendation to use, source, or self-administer TB-500.
Ready to build a recovery protocol on peptides with real evidence and a real delivery system? Explore the RESTORE protocol →
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.