
Does an NAD supplement really work? What the human trials, blood NAD data and null findings actually show, and how to tell if yours is doing anything.
Introduction
If you've been staring at a forty-dollar bottle of NAD pills wondering whether it does anything at all, you are asking the right question. The longevity shelf has been flooded with confident promises about energy, sharper mornings, and the inside of your cells running like new. Most of those bottles don't tell you the part that actually decides whether any of it matters.
This guide is for research purposes only. It walks through what "really work" honestly means for an NAD supplement, what the human trials show, where the evidence holds up, and where it falls apart. No hype, no hedging, just the data you'd want before spending the money.
The short version:
- The science is real but narrower than the marketing. Human trials show NAD precursors can raise blood NAD+, but raising NAD+ is not the same thing as making you feel different.
- Two precursors have the strongest human evidence: nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN). Direct NAD+ in oral capsules has almost none.
- Some trials show real outcomes (insulin sensitivity, gait speed, grip strength). Others show clean nulls (NR did nothing for insulin sensitivity in obese men, NR didn't improve walking in heart failure).
- Whether yours "works" depends on the form, the dose, the route, and what you're actually trying to change.
- The honest answer for most people is: it does something measurable in your blood, and somewhere between a little and nothing in how you feel, and the route you choose decides which.
What does "really work" actually mean here?
This is where most of the argument falls apart before it starts. "Works" can mean three completely different things, and brands lean on whichever one suits them.
The three meanings, in plain language:
- Raises blood NAD+. Does swallowing this pill actually put more NAD into your bloodstream, where your cells can use it?
- Changes a biomarker your doctor would care about. Things like insulin sensitivity, blood pressure, inflammation markers, or muscle strength on a measurable test.
- Changes how you feel day to day. Energy, sleep, mental sharpness, recovery, the subjective stuff that made you buy the bottle.
A supplement can hit one of those without hitting the other two. NAD precursors are actually quite good at the first, mixed on the second, and almost completely silent in the human trials about the third. That mismatch is the whole reason this question keeps coming up.
Does an NAD supplement raise your blood NAD?
Yes, the right form at the right dose does. This is the strongest single piece of evidence in the whole category, and it is genuinely settled.
The clearest human trial is Martens and colleagues, published in Nature Communications in 2018. Healthy middle-aged and older adults took 1,000 mg of nicotinamide riboside (NR) daily for six weeks. Their blood NAD+ levels rose by about 60% compared to placebo, measured in peripheral blood mononuclear cells.
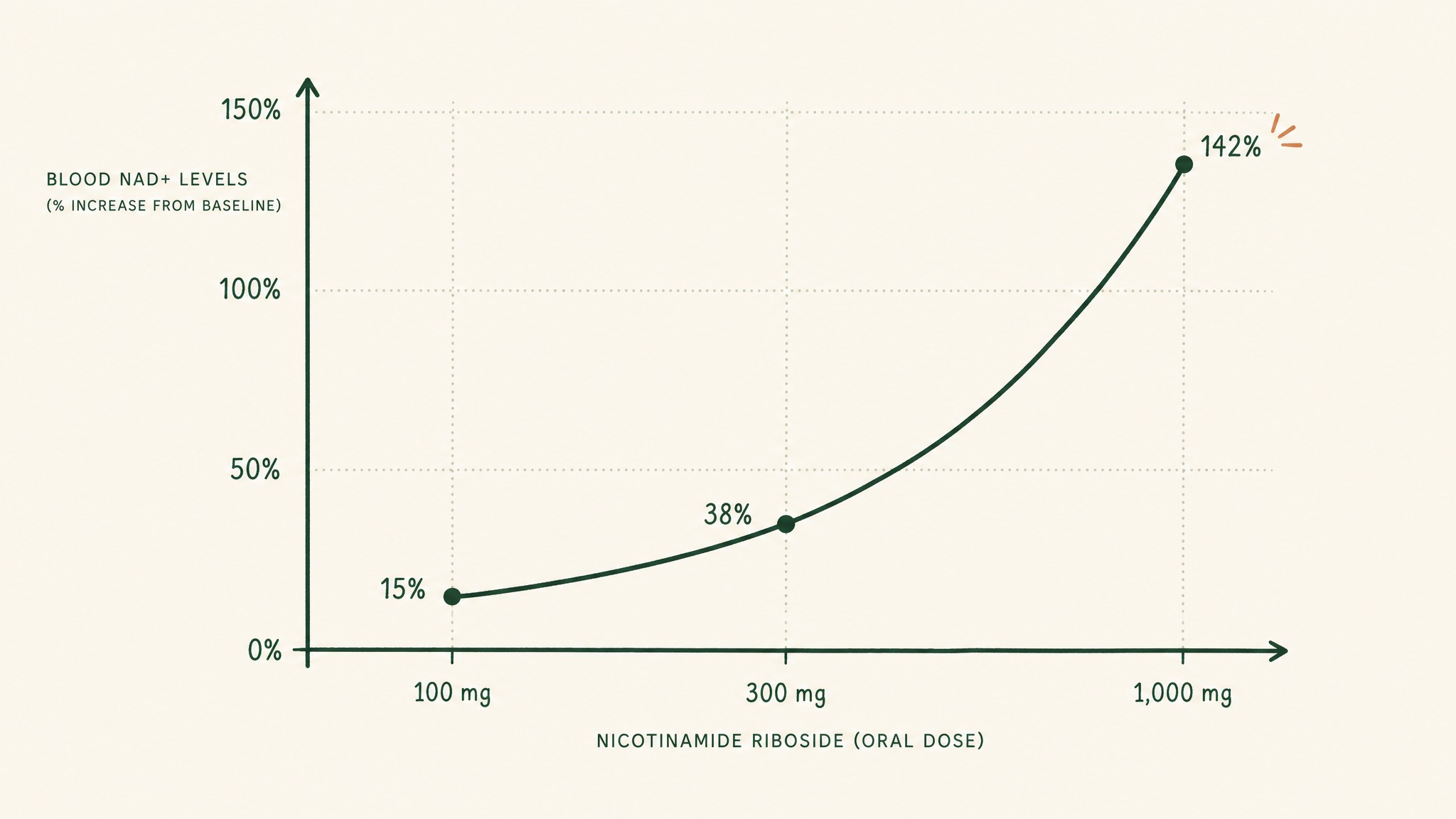
Blood NAD+ rises steeply as oral nicotinamide riboside dose increases from 100 to 1,000 mg.
A follow-up trial by Conze and colleagues in 2019 ran the dose response more carefully. At 100 mg, 300 mg, and 1,000 mg of NR per day, whole-blood NAD+ rose by roughly 22%, 51%, and 142% within two weeks. So dose matters, and the curve is not flat.
On the NMN side, Yamaguchi and colleagues published an eight-week trial in 2024 in middle-aged Japanese men. NAD+ levels in their immune cells rose steadily across the study and the regimen was well tolerated. The pattern is the same as the NR trials: oral precursors get into your blood, your cells convert them, your NAD pool rises.
A quick reality check on that, though. Blood NAD+ rising is the first hurdle, not the finish line. It tells you the molecule is reaching the right place. It does not tell you anything will change because of it.
Does it actually change anything in human trials?
Here the picture gets more honest. Some trials show real outcomes. Others land flat. The pattern is interesting.
The trials that did show something

Why NAD+ rises in both groups, but only one group's health markers improve.
Yoshino and colleagues published a 2021 trial in Science that quietly became the most cited NAD paper in years. Postmenopausal women with prediabetes took 250 mg of NMN daily for ten weeks. Their muscle insulin sensitivity improved by about 25%. Insulin sensitivity is a real biomarker, not a vibe, and the trial used the gold-standard clamp method to measure it.
Igarashi and colleagues, also published in 2022, ran a parallel study in older Japanese men. The same 250 mg daily dose of NMN over twelve weeks led to small but measurable gains:
- Gait speed improved (a marker of healthy ageing that predicts mortality risk)
- Left grip strength improved
- NAD+ in blood rose
These are modest effects. They are also exactly the kind of biomarkers gerontologists care about, and they emerged from a clean, placebo-controlled design.
The trials that landed flat
Dollerup and colleagues ran a 2018 trial in the American Journal of Clinical Nutrition that the supplement industry doesn't quote nearly enough. Obese, prediabetic men took 2,000 mg of NR per day for twelve weeks. Their NAD+ went up. Their insulin sensitivity did not improve. Their lipid metabolism did not improve. Their mitochondrial function did not improve.
In our protocol design work, we've learned to read trials like that one carefully. The Dollerup result isn't a failure of the molecule. It's a signal that the population matters: prediabetic men carry a different metabolic state than postmenopausal women, and what raises NAD+ in both doesn't translate into the same functional benefit in either.
Wang and colleagues published a 2022 trial in JACC Basic Translational Science on NR in heart failure with reduced ejection fraction. NAD+ in the blood roughly doubled. Walking distance on the standard six-minute walk test? No difference. Cardiac function? No difference. Quality of life? No difference. The molecule got in. The clinical needle did not move in twelve weeks.
So the honest reading is: NAD precursors raise NAD+ reliably. Whether that translates into something a doctor can measure depends heavily on the population, the dose, and the outcome being tracked.
Why do most people feel nothing on an NAD supplement?
If the science is real, why do so many users report close to nothing? Three reasons stack up.
The first is bioavailability. NAD+ itself is a big, polar molecule with a molecular weight of about 663 daltons. It does not cross cell membranes easily, which is why the precursor pathway exists in the first place. When you swallow a capsule labelled "NAD+," very little of the actual NAD+ molecule survives the journey from stomach to bloodstream to cell. The precursors NR and NMN do better, but they still face acid, gut enzymes, and a liver that converts most of what arrives into smaller building blocks before sending anything back out.
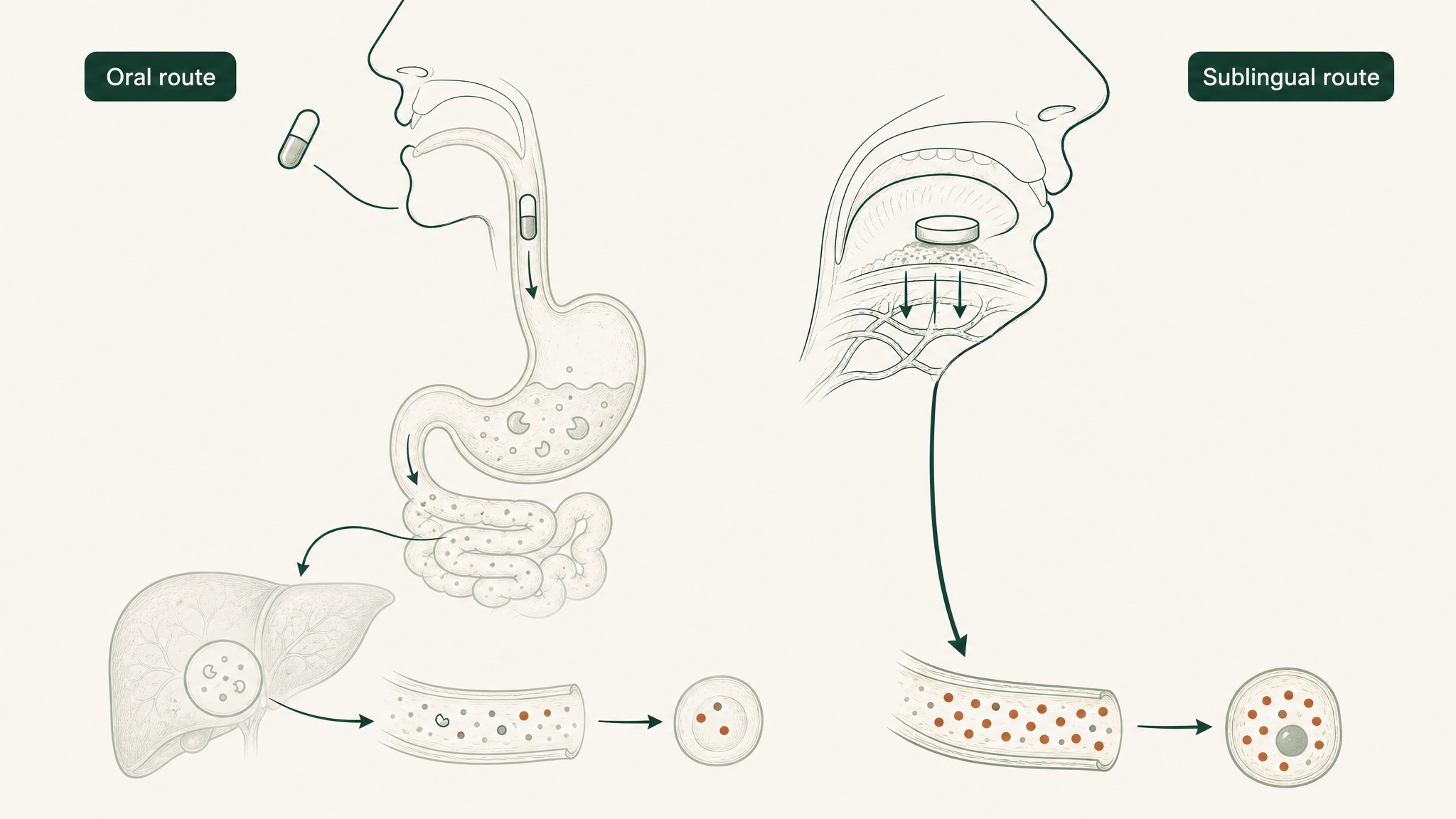
Oral NAD precursors lose potency through stomach acid and liver metabolism; sublingual delivery bypasses both.
The second is the gap between biochemistry and subjective experience. Your cellular energy production is not the same thing as how energetic you feel. Insulin sensitivity is not the same thing as feeling less foggy after lunch. The trials measure the first kind of thing. The subjective stuff is what bottles promise.
The third is the route. Oral capsules and tablets work, but they work the long way around: through your gut, through your liver, into your bloodstream. That route loses a lot of the dose to first-pass metabolism, the process where your liver breaks down compounds before they reach systemic circulation. Sublingual delivery, where a tablet dissolves under your tongue, bypasses that detour and reaches the bloodstream through the thin tissue lining your mouth. This is the same principle behind sublingual nitroglycerin in cardiology, where bypassing the liver is the whole point. For an NAD precursor, that route lets a smaller dose deliver more of itself intact, which is the thinking behind VERO LEGACY and its VERISORB sublingual delivery system.
So is NAD a "real" supplement or longevity theatre?
It's real. It's also narrower than the marketing.
Real, in the sense that:
- Blood NAD+ can be raised by oral NR or NMN, confirmed in multiple placebo-controlled human trials.
- In the right population, that rise tracks with measurable outcomes (Yoshino on insulin sensitivity, Igarashi on muscle function).
- The FDA has issued a "no questions" letter for nicotinamide riboside chloride (GRN 635). That review allows the precursor to be sold legally as a food ingredient in the US.
Narrower, in the sense that:
- Not every trial shows benefit. Dollerup and Wang are real null findings in real populations.
- Most of the positive trials are small, short, and measure surrogates rather than hard clinical endpoints.
- The subjective claims ("more energy," "sharper focus") have not been demonstrated in any large, blinded human trial of NAD precursors. Users report these effects, but the evidence is anecdotal, not clinical.
If someone tells you it's pure marketing, they haven't read Yoshino. If someone tells you it's miracle fuel, they haven't read Dollerup. Both have to be true for the picture to make sense.
How can you tell if your NAD supplement is actually working?
This is the practical question, and there are three reasonable ways to answer it.
The most rigorous: get an NAD+ blood test before you start and after eight to twelve weeks. Several labs offer dried blood spot tests for NAD+. If the number goes up meaningfully, the supplement is doing what the trials say it does. If it doesn't move, change the form, dose, or route before the year of bottles drains your wallet.
The middle option: track a biomarker the trials have shown can shift. For a healthy person, that might be HbA1c, fasting insulin, grip strength, or a timed gait-speed test you can do at home. For an older adult, gait speed and grip strength are the cleanest markers of the kind of changes Igarashi reported.
The least rigorous, but the one most people actually use: a subjective journal. Sleep quality, energy at 3pm, perceived recovery after exercise, mental sharpness. Track for ninety days. Be honest about placebo, dose adjustments, and whether you started anything else at the same time. If nothing shifts, that's data too.
A blunt note from our research work: most users overestimate what they feel in the first month, and underestimate what they see on the third blood test. The trial data follows the same shape. Give it twelve weeks before deciding.
Which form gives you the best shot at it working?
If you've decided to try one, the form and route decide most of the outcome before the dose does. The rough hierarchy looks like this:
- Injectable NAD or NMN. Bypasses your gut and liver entirely, but expensive, clinic-bound, and not a daily proposition for most people.
- Sublingual NMN or NAD+. A small daily dose that absorbs directly into the bloodstream under the tongue, missing the gut and the liver loop.
- Liposomal oral NAD+ or NMN. Encapsulates the molecule in fatty bubbles to improve gut absorption. Better than plain capsules, still goes through the liver.
- Standard capsule NR or NMN. The most studied route in human trials. Works, but needs higher doses (often 250 to 1,000 mg) to overcome first-pass losses.
- "NAD+" capsules. Direct NAD+ in a capsule is the worst-studied form. The molecule's size and charge make oral absorption poor, and the trials use precursors for a reason.
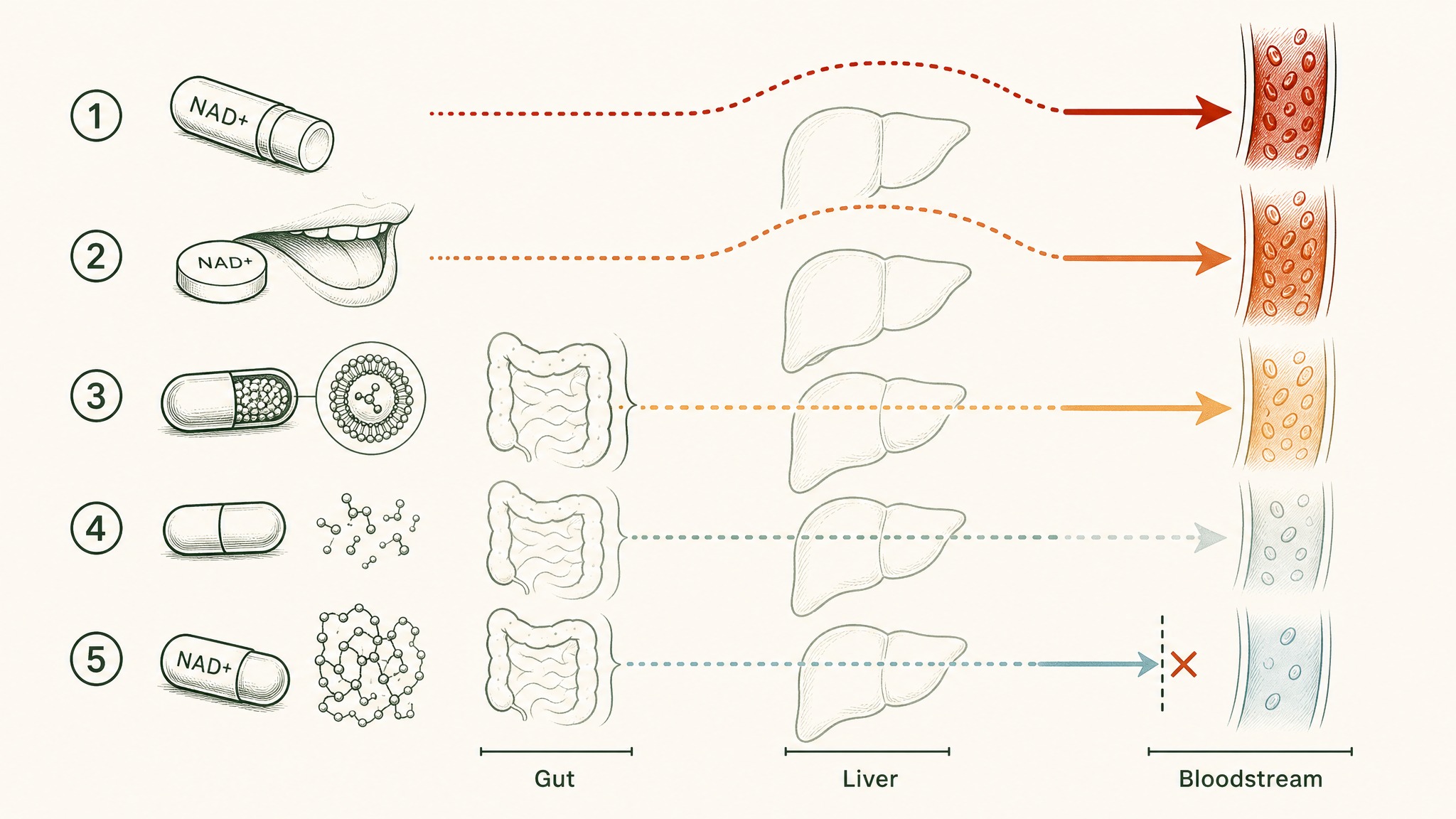
How five NAD+ delivery routes differ in how much actually reaches your bloodstream.
If you've tried a capsule and felt nothing, the next sensible experiment is the route, not the dose. Sublingual NMN at a smaller daily dose often outperforms a larger capsule dose for the same molecule, because more of what you actually swallow reaches your bloodstream.
The honest verdict
Does an NAD supplement really work? In the literal, measurable sense, yes. The best-studied forms raise blood NAD+ reliably, and in the right population they shift biomarkers a careful doctor would notice.
In the marketing sense (energy, focus, the cinematic version of feeling younger), the human trials are quieter than the bottle suggests. What members experience varies enormously. Some feel a real difference. Others feel nothing despite biochemical changes happening in the background.
If you go in expecting a measurable lift in your NAD pool and a slim chance of feeling something noticeable, you'll be where the data actually sits. If you go in expecting a transformation, the trials suggest you'll be disappointed regardless of which bottle you buy.
FAQ
How long until an NAD supplement starts working?
The blood NAD+ rise begins within two weeks at clinically studied doses, based on Conze 2019 and Trammell 2016. Biomarker shifts in the positive trials (Yoshino, Igarashi) appeared at 10 to 12 weeks. If you're tracking subjective effects, give it at least eight weeks before drawing conclusions.
Is NMN or NR better?
Both raise blood NAD+ in human trials. NR has a longer safety record and the FDA "no questions" letter (GRN 635). NMN has the positive Yoshino insulin sensitivity result and the Igarashi muscle function result. Choose the one with the form factor and route you can stick to.
Does an oral NAD supplement work at all?
It raises blood NAD+ when the form is NR or NMN. Direct NAD+ in oral capsules has poor evidence because the molecule is too large and polar for efficient oral absorption. Sublingual and injection routes work around that limit.
Why didn't I feel anything from my NAD supplement?
The most likely reasons: the form was direct NAD+ rather than a precursor, the dose was below the threshold the trials use (usually 250 mg minimum for NMN, 300 mg or more for NR), the route was oral rather than sublingual or injection, or the timeframe was too short. A twelve-week trial of a different form or route is the most sensible next experiment.
Can NAD supplements actually slow ageing?
Research suggests an NAD precursor can shift biomarkers tied to ageing (insulin sensitivity, gait speed, grip strength) in specific populations, including older men and prediabetic women. No human trial has shown that an NAD supplement extends lifespan or slows the ageing process itself, because the trials needed to prove that would take decades. The honest framing is "biomarker improvement in some trials," not "anti-ageing."
Key Takeaways
- NAD precursors (NR, NMN) reliably raise blood NAD+ in human trials. This is the strongest, most replicated finding in the category.
- The effect on biomarkers depends on the population. Yoshino showed insulin sensitivity gains in prediabetic women. Dollerup showed nothing in obese men.
- Subjective effects (energy, focus, recovery) are reported by users but not confirmed in large blinded trials. Members experience varies widely.
- Form and route matter more than brand. Direct oral NAD+ has the weakest evidence. Sublingual delivery bypasses the first-pass liver loop that limits standard capsules.
- The realistic expectation is a measurable rise in your blood NAD pool, with a slim chance of feeling a clear day-to-day difference. The trials look exactly like that.
- If you want to know whether yours is working, blood test before and at twelve weeks. The data beats the journal every time.
References
- Massudi H, Grant R, Braidy N, Guest J, Farnsworth B, Guillemin GJ. Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLoS One. 2012;7(7):e42357. https://pmc.ncbi.nlm.nih.gov/articles/PMC3407129/. Retrieved 2026-06-30.
- Clement J, Wong M, Poljak A, Sachdev P, Braidy N. The plasma NAD+ metabolome is dysregulated in normal aging. Rejuvenation Res. 2019;22(2):121-130. https://pmc.ncbi.nlm.nih.gov/articles/PMC6482912/. Retrieved 2026-06-30.
- Martens CR, Denman BA, Mazzo MR, et al. Chronic nicotinamide riboside supplementation, tolerability, and blood NAD+ measurements in healthy middle-aged and older adults. Nat Commun. 2018;9(1):1286. https://pmc.ncbi.nlm.nih.gov/articles/PMC5876407/. Retrieved 2026-06-30.
- Conze D, Brenner C, Kruger CL. Safety and metabolism of long-term administration of NIAGEN (nicotinamide riboside chloride) in a randomized, double-blind, placebo-controlled clinical trial of healthy overweight adults. Sci Rep. 2019;9:9772. https://www.nature.com/articles/s41598-019-46120-z. Retrieved 2026-06-30.
- Trammell SAJ, Schmidt MS, Weidemann BJ, et al. Nicotinamide riboside oral bioavailability data in mice and humans. Nat Commun. 2016;7:12948. https://pubmed.ncbi.nlm.nih.gov/27721479/. Retrieved 2026-06-30.
- Yoshino M, Yoshino J, Kayser BD, et al. Nicotinamide mononucleotide and muscle insulin sensitivity in prediabetic women. Science. 2021;372(6547):1224-1229. https://pmc.ncbi.nlm.nih.gov/articles/PMC8550608/. Retrieved 2026-06-30.
- Igarashi M, Nakagawa-Nagahama Y, Miura M, et al. Chronic nicotinamide mononucleotide supplementation, blood NAD+ levels, and muscle function in healthy older men. NPJ Aging. 2022;8(1):5. https://pmc.ncbi.nlm.nih.gov/articles/PMC9158788/. Retrieved 2026-06-30.
- Yamaguchi S, Irie J, Mitsuishi M, et al. Safety and long-term NMN supplementation outcomes on metabolism, sleep, and NAD+ biosynthesis in middle-aged Japanese men. Endocr J. 2024;71(2):153-169. https://pubmed.ncbi.nlm.nih.gov/38191197/. Retrieved 2026-06-30.
- Dollerup OL, Christensen B, Svart M, et al. A randomized placebo-controlled clinical trial of nicotinamide riboside in obese men: safety, insulin-sensitivity, and lipid-mobilizing outcomes. Am J Clin Nutr. 2018;108(2):343-353. https://pubmed.ncbi.nlm.nih.gov/29992272/. Retrieved 2026-06-30.
- Wang DD, Airhart SE, Zhou B, et al. Safety and tolerability of nicotinamide riboside in heart failure with reduced ejection fraction. JACC Basic Transl Sci. 2022;7(12):1183-1196. https://pmc.ncbi.nlm.nih.gov/articles/PMC9831861/. Retrieved 2026-06-30.
- Herman TF, Santos C. First-pass effect. StatPearls. NIH National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK551679/. Retrieved 2026-06-30.
- Chini CCS, Tarrago MG, Chini EN. NAD and the aging process: role in life, death and everything in between. Mol Cell Endocrinol. 2017;455:62-74. https://pmc.ncbi.nlm.nih.gov/articles/PMC5419884/. Retrieved 2026-06-30.
- US Food and Drug Administration. Agency response letter GRAS Notice No. GRN 000635 (nicotinamide riboside chloride). https://www.fda.gov/food/gras-notice-inventory/agency-response-letter-gras-notice-no-grn-000635. Retrieved 2026-06-30.
Want a sublingual NAD protocol designed to bypass the gut and liver loop? Explore VERO LEGACY.
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.