
How to build a longevity supplement stack that actually compounds. Sequencing, timing, peptide layer, and the interactions that undermine yours.
If you scroll long enough on supplements longevity content, you will end up with a shopping list of twelve bottles and no plan for how to take them. That is the gap this guide fills, for research purposes only. The compound list is the easy half of the problem; the stack design is the half that decides whether anything compounds.
Most people start with a confident bottle, add another one after the next podcast, and end up six months in with a row of capsules that overlap, interact, or block each other in the gut. The list looks impressive on the shelf. The pharmacology underneath is a tangle.
Research suggests the order, timing, and route you take things matters at least as much as the molecules themselves.
This article is the companion piece to our 2026 evidence review of supplements for longevity. That one rates the compounds. This one shows you how to sequence them.
Before you read on, a heads up:
- Most longevity stacks fail on timing and absorption, not on compound choice.
- The right base stack is small, cheap, and boring; the interesting work happens in the layers above it.
- Peptides sit on top of a foundation, never instead of it.
- Two compounds taken together can quietly cancel each other out.
Why does most stacking advice fall apart?
The internet treats supplements longevity like a draft pick. Pick the molecule with the strongest study, add it to the pile, repeat.
That works for a week. It falls apart by month three for a simple reason: most stacks ignore that compounds have to share three things: your gut, your liver, and your dosing window.
A few common failure modes you will spot in your own routine if you look:
- Two fat-soluble vitamins taken on an empty stomach so neither absorbs.
- Iron and your morning coffee within twenty minutes of each other, gutting absorption.
- Resveratrol and curcumin in the same dose, competing for the same metabolic pathway.
- An NAD precursor taken alone for nine months with no attention to the methylation cost it stacks up.
The mistake is not the compound. It is the sequence.
Most stacks are also overweighted toward the compound end of the problem. People will spend $200 on a fancy spermidine, then ruin its absorption by taking it with a stimulant. Fixing the sequence costs nothing, and it is the cheapest performance gain in this entire space.
What is your stack actually supposed to do?
Before you choose a single capsule, you have to decide what longevity even means to you. The word covers three different goals, and a stack tuned for one might do nothing for the others.
- Lifespan. How many calendar years you live.
- Healthspan. How many of those years you spend walking up stairs, thinking clearly, sleeping well, and recovering quickly.
- Biological age. A measurement of cellular wear-and-tear, scored by blood tests like the GrimAge or Horvath clocks.
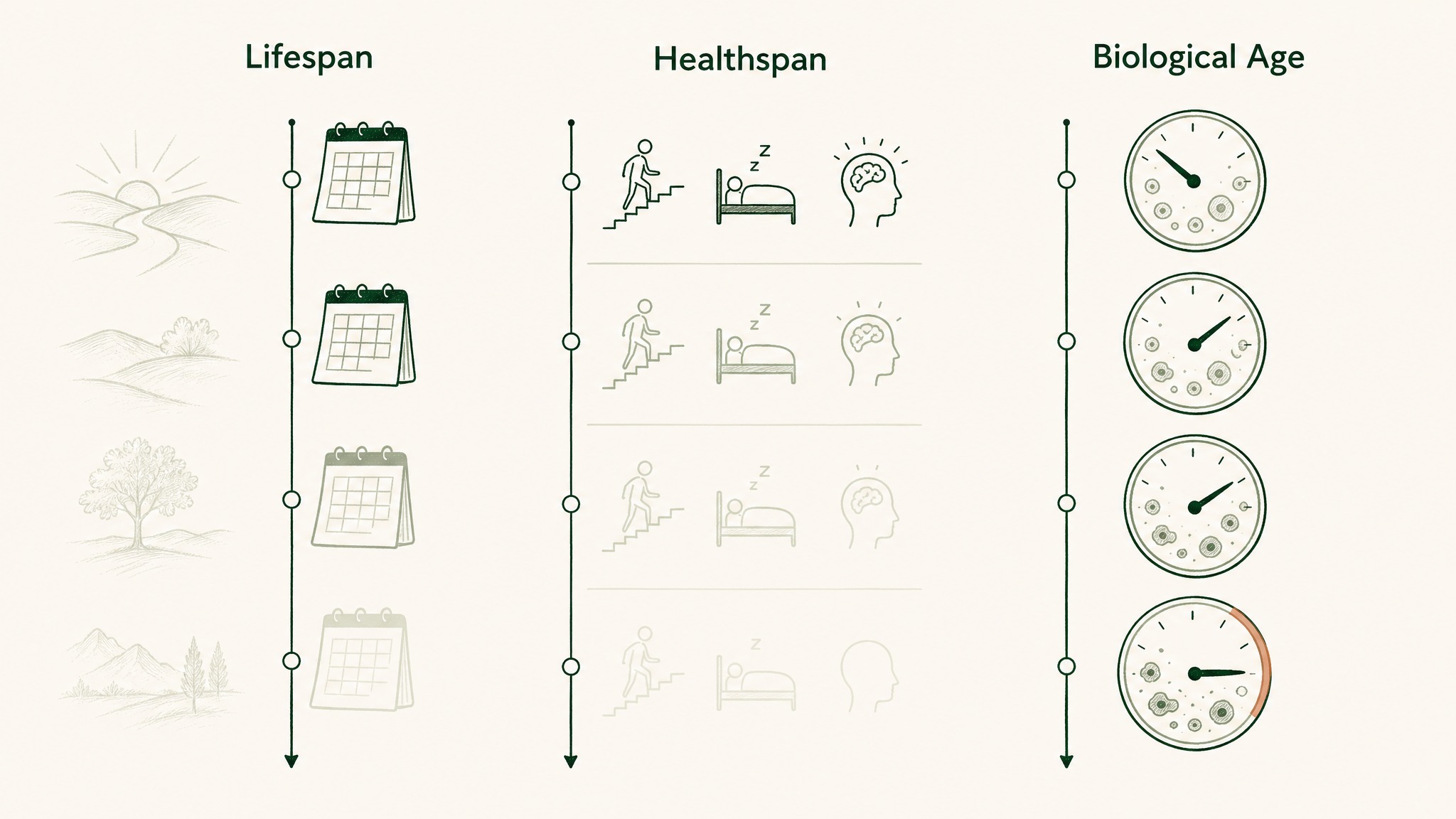
Lifespan, healthspan, and biological age measure three different aspects of aging.
Most people who say lifespan actually mean healthspan. The honest stack is built for healthspan first; the lifespan signal in any single supplement is, in humans, still mostly a hope.
Once the goal is set, the design map almost everyone in longevity research now uses is the 12 Hallmarks of Aging, updated by López-Otín and colleagues in 2023 in Cell. Each hallmark (mitochondrial dysfunction, chronic inflammation, deregulated nutrient sensing, and nine more) is a biological process that drifts with age. A useful stack covers three or four hallmarks, not one of them six different ways.
If a compound cannot map cleanly to a hallmark, it probably does not belong in your stack. That single filter cuts a typical twelve-bottle stack in half before you have spent another dollar.
How do you sequence a stack so it compounds?
Sequencing is the part nobody on YouTube covers because it is unglamorous. It is also where the entire compounding effect lives. Three rules do most of the work.
- Group by route. Fat-soluble vitamins (A, D, E, K) ride with a meal that has fat. Water-soluble vitamins (B-complex, C) can go on an empty stomach. Iron and calcium should be separated by at least two hours because they block each other.
- Group by time of day. Anything stimulating (B-complex, creatine pre-workout, alpha-GPC) goes early. Anything calming (magnesium glycinate, glycine, taurine) goes evening. NAD precursors are usually morning because they nudge metabolism in a direction your body should not be in at midnight.
- Group by methylation cost. NAD precursors (NMN, NR) consume methyl donors as they get used. Run them long enough without pairing TMG (trimethylglycine), a cheap methyl donor, and you can drift homocysteine in the wrong direction. The fix is one pill, not a rebuild.
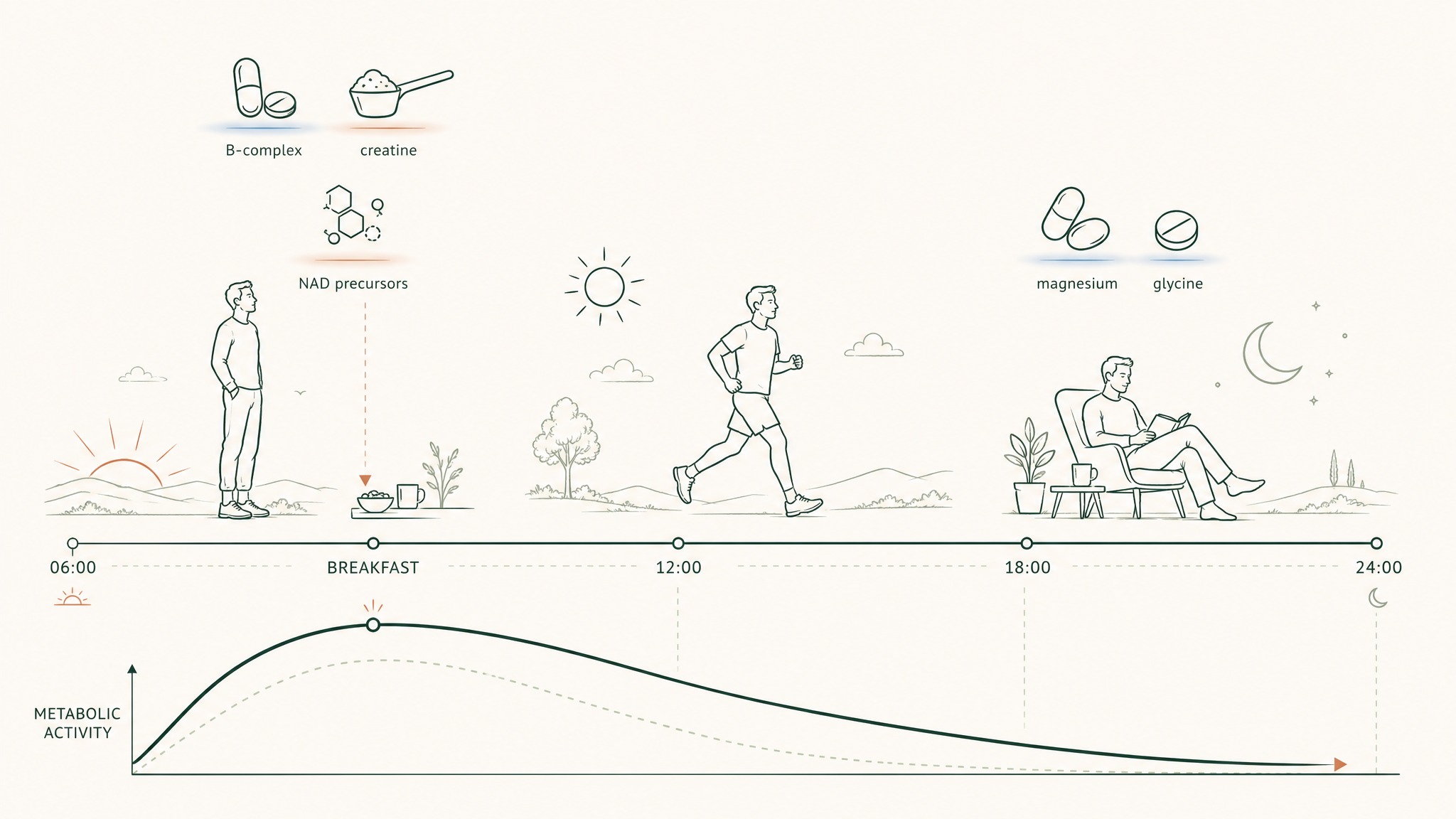
Why taking NAD+ at breakfast works better than taking it at bedtime.
In our protocol design work at Peak Human Labs, the single most common mistake I see in supplement stacks is people running expensive compounds at the wrong time of day. A great NAD precursor taken at 10pm undoes most of why you bought it, because you have asked the cell's energy machinery to wake up when it should be powering down. Move it to breakfast and the same bottle starts behaving like its label promised.
Sequencing rules aside, the boring truth is that consistency outranks complexity. A four-compound stack you actually take is worth more than a ten-compound stack you remember twice a week.
What goes in tier one of every honest stack?
The foundation is the part most longevity influencers skip because it is too cheap to sell. It is also the part with the cleanest human evidence. Four compounds, in this order of importance.
- Omega-3 EPA + DHA. Around 2 g daily total. Bhatt and colleagues' 2019 REDUCE-IT trial in NEJM randomised over 8,000 high-risk patients to icosapent ethyl versus placebo and the primary cardiovascular endpoint dropped by 25%. That is the kind of effect size most longevity compounds would envy. Third-party tested matters here because oxidised fish oil is worse than no fish oil.
- Vitamin D3 with K2. Dose to a blood level of 30 to 50 ng/mL, not to a fixed number on the bottle. Manson 2019 VITAL in NEJM showed correcting a deficiency matters far more than topping up an adequate level. Pair with K2 if you are running this long-term.
- Magnesium glycinate or threonate. 200 to 400 mg of elemental magnesium in the evening. Veronese 2020 published an umbrella review across 16 meta-analyses and the strongest signals were on sleep, blood pressure, and migraine frequency.
- Creatine monohydrate. 3 to 5 g daily, indefinitely. Avgerinos 2018 reviewed six RCTs in healthy individuals and found short-term memory and reasoning signals on top of the older muscle case. Sarcopenia, the loss of muscle with age, is one of the strongest predictors of late-life decline, and creatine is the cheapest molecule that pushes against it.
The whole tier costs under $50 per month. Most people who add this and remove half their other bottles will feel no different and will be objectively better off, which is the honest description of a working foundation.
Users report this is the layer where the biggest gains hide because it is unglamorous enough to skip.
When should you add a NAD precursor?
NAD+ is a cofactor your cells use to convert food into energy. Levels fall as you age, which is why NMN and NR became the headline supplements of the longevity decade.
The harder question is when and how to take one. Timing and route decide how much of the bottle reaches the cell; the choice of whether is the easy half.
Add a NAD precursor only after tier one is in place and you have run it for at least eight weeks. Layering precursors onto a sleep-deprived, magnesium-deficient body is a way to waste a $90 bottle.
The cleanest human evidence is the Yoshino 2021 trial in Science. Postmenopausal women with prediabetes took 250 mg of NMN orally for ten weeks and muscle insulin sensitivity improved versus placebo.
The dose was modest. The endpoint was real.
A few practical sequencing notes:
- Morning is the right window. NAD precursors nudge metabolism in a direction you do not want at night.
- Pair with TMG (trimethylglycine) if you are running long-term, to offset the methyl drain.
- The oral-versus-sublingual debate is real. Capsule NMN works for some endpoints; sublingual NAD+ delivery puts the molecule directly into circulation, bypassing the liver's first-pass filter. Our deep dive on the NAD cascade and sirtuins covers the trade-off; the NAD supplement comparison piece handles the brand-level decision.
The LEGACY NAD+ Protocol is VERO's sublingual answer to the absorption side of this question for research purposes only. The wider point applies to any NAD product you choose: the dose that reaches the cell decides the effect, not the dose printed on the bottle.
Where do peptides fit your protocol?
This is the layer almost every other supplements longevity guide pretends does not exist. Peptides are short chains of amino acids your body already uses as signalling molecules. As you age, you make less of several of them, and that decline maps onto multiple Hallmarks of Aging at once.
They are not on standard supplement lists for one reason: they sit outside the FDA's dietary-supplement framework. That is a regulatory category line, not a biology one. The mechanism work on the peptides discussed in research literature compares favourably with several Tier B and Tier C supplements that everyone happily lists.
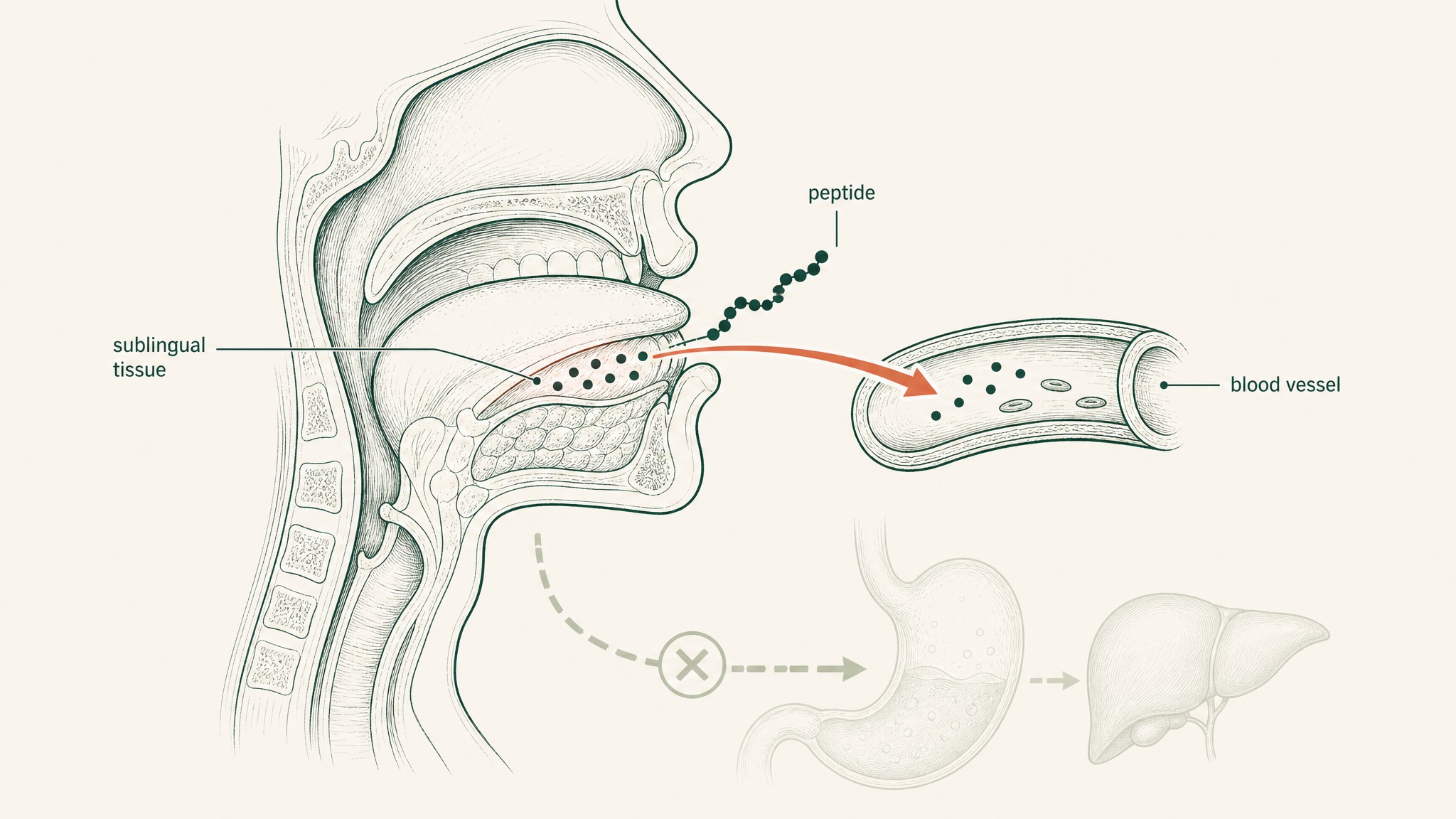
Peptides absorbed under the tongue enter the bloodstream directly, skipping stomach acid and liver processing.
A short tour of the peptides most often researched in a longevity context:
- GHK-Cu. A tiny three-amino-acid copper peptide your liver and skin already make. By age 60, your body produces less than half of what it made in your twenties. Pickart and Margolina's 2018 review in Int J Mol Sci catalogues a wide preclinical reach: research suggests collagen and elastin signalling, anti-inflammatory effects, and DNA-repair gene activation, mostly in animal and cell models. Maps to altered intercellular communication and stem-cell exhaustion in the Hallmarks framework.
- MOTS-c. A mitochondrially-encoded peptide. Lee and colleagues' 2015 paper in Cell Metabolism characterised MOTS-c as a signal that, in research models, has been observed to regulate insulin sensitivity and metabolic homeostasis by acting on skeletal muscle. Maps to mitochondrial dysfunction and deregulated nutrient sensing.
- Epitalon. A short peptide bioregulator with a long Russian research history, summarised in Khavinson 2012. The human work is observational and outside the Western RCT framework, so the field reads it as hypothesis-generating, not definitive. Members experience varied responses in research settings.
- BPC-157. A 15-amino-acid pentadecapeptide reviewed by Seiwerth and colleagues in 2021 in Frontiers in Pharmacology. In animal models, research suggests it supports tissue repair across multiple organ systems. Human RCT data is sparse.
The single biggest practical problem with peptides is delivery. Almost every peptide in this list is destroyed by stomach acid, which is why most research uses injection. Sublingual delivery (the route built into the VERISORB sublingual delivery system) places the molecule under the tongue, where the thin tissue lets it slip directly into circulation, skipping the gut and the liver's first-pass filter. The trade-offs are walked through in our sublingual versus oral peptide piece.
For a fuller read on the science specific to age-supportive peptides, the companion piece is age-supportive peptides: what the research shows. The honest framing is that peptides are a layer on top of tier one, never a replacement for it.
What undermines the stack you already have?
A clean stack will quietly self-sabotage if you do not watch a handful of interactions. The classics, in order of how often they ruin otherwise good protocols.
- Coffee plus iron. Tannins in coffee and tea sharply reduce iron absorption when taken within thirty minutes. If you take iron, take it on an empty stomach with vitamin C, two hours from coffee.
- Calcium plus iron. Same direction, same fix: two-hour gap.
- Resveratrol plus curcumin. Both fight for the same hepatic glucuronidation pathway. Stacked at the same dose, each one's bioavailability drops.
- Fat-soluble vitamins on an empty stomach. A, D, E, and K need dietary fat to absorb. Bottled olives, almonds, or a normal meal does the job. A fasted morning capsule does not.
- High-dose zinc without copper. Long-term zinc supplementation can drive copper down. If you are running zinc above 30 mg daily for months, pair it with a small copper dose.
- NAD precursor without methyl support. As above. TMG is the cheap fix.
There is a wider absorption story behind most of these. The number on the bottle is the number that went into the capsule. It is almost never the number your body ends up with.
Anything that destroys, blocks, or competes with absorption is a tax on the dose you paid for. Our oral peptide bioavailability deep dive covers why this matters most for peptide-class molecules, but the principle is the same across the stack.
The cheapest performance gain in your stack is fixing the interactions, not buying another bottle.
How does an age-based protocol actually progress?
The same stack does not fit every decade. Here is how the protocol pattern usually evolves, with the foundation never going anywhere.
Twenties and thirties. Foundation only, in most cases. Omega-3, vitamin D3 with K2, magnesium, creatine.
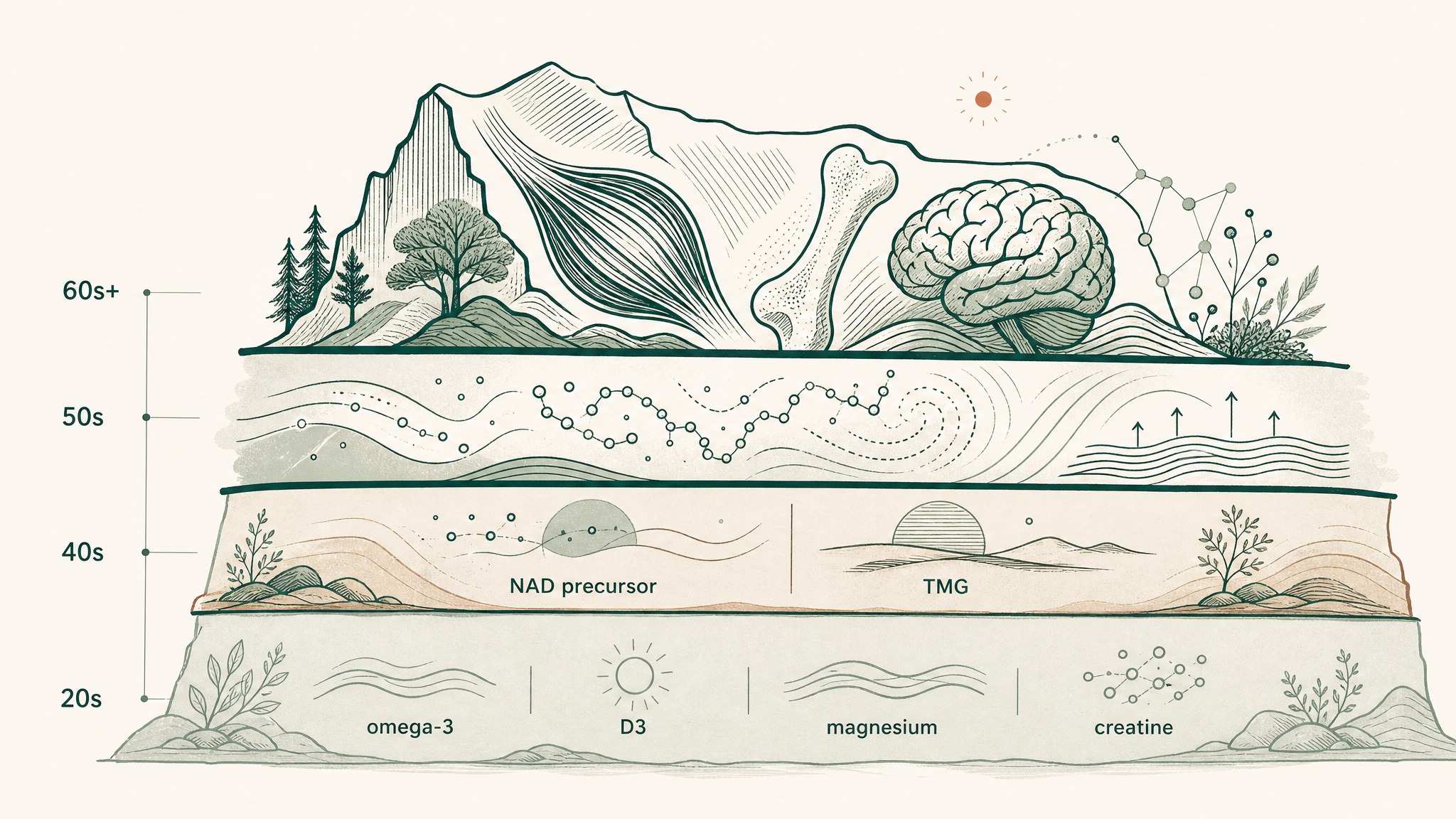
How your supplement stack builds with each decade, keeping the foundation steady underneath.
Layer in B-complex if your diet is patchy. Anchor sleep, training, and food quality as the upstream stack; supplements are downstream of those.
Forties. Foundation plus a NAD precursor, dosed in the morning, paired with TMG if running long-term. Consider taurine at 1 to 3 g daily based on the Singh 2023 paper in Science. Start running annual blood panels (vitamin D, ferritin, B12, homocysteine, fasting insulin, lipid panel including ApoB) so the stack is steered by data, not by trend.
Fifties. Foundation plus NAD plus targeted peptide research as appropriate. This is the decade where members experience the biggest gap between calendar age and how they feel, which is often where the peptide-class research layer first becomes worth the complexity. Sublingual delivery becomes important because gut and liver capacity start to drift.
Sixties and beyond. Same foundation, with a heavier focus on muscle (protein intake, creatine, resistance training), bone (vitamin D and K2 dosed by blood level), cognition (omega-3, possibly creatine for cognitive endpoints), and any peptide-class research layer you and your doctor decide to run.
The pattern is layering, not replacing. The tier-one stack does not go anywhere; the layers above it are what changes.
Frequently asked questions
What is the single most important supplement for longevity?
There is not one. The closest thing to a universal recommendation is omega-3 EPA + DHA at around 2 g daily, because cardiovascular disease is the largest single cause of premature death and the RCT data here is cleaner than for anything else on a longevity shelf. Creatine is a close second on cost-per-evidence-unit.
How many longevity supplements should I take?
Fewer than you think. A working tier-one stack is four compounds. Adding a NAD precursor brings it to five. Most people are better served by running five compounds well than ten compounds half-heartedly.
Are sublingual supplements really better than capsules?
For the right molecules, yes. Sublingual absorption places the compound directly into circulation, skipping both the stomach acid and the liver's first-pass metabolism.
That matters most for peptides, NAD+, glutathione, and B12. For stable small molecules like creatine or vitamin D3, the route makes little difference.
Can I take all my longevity supplements at once?
No. Group fat-soluble vitamins with a meal that has fat. Move NAD precursors to morning.
Move magnesium and glycine to evening. Separate iron and calcium by at least two hours. Keep resveratrol and curcumin out of the same dose.
The pillbox is a sequencing tool, not a basket.
Where do peptides fit a longevity stack?
On top of tier one, in research contexts. Peptides like GHK-Cu, MOTS-c and Epitalon sit outside the FDA's dietary-supplement framework, but the mechanism work behind them is at least as serious as several supplements that are happily on standard lists. Delivery (sublingual or injectable) is the deciding variable.
How do I know if my stack is working?
Track three things: how you sleep, how you recover, and an annual blood panel. If those three are improving year over year and your subjective energy is up, the stack is doing its job. If you have added six bottles and you cannot tell what changed, the stack is too noisy to read.
Key Takeaways
- A longevity stack lives or dies on sequence, timing, and route, not on the impressive label on the latest bottle.
- The honest foundation is four compounds: omega-3, vitamin D3 with K2, magnesium, and creatine. Most people would get better outcomes from running this four-stack cleanly than from running their current ten-stack chaotically.
- NAD precursors are a tier-two addition, taken in the morning, paired with TMG long-term, with sublingual delivery worth considering for absorption.
- Peptides sit on top of the foundation, not instead of it. The biology is serious; the regulatory category is the only reason they are not on standard supplement lists.
- Watch the interactions that quietly tax your absorption: coffee with iron, calcium with iron, resveratrol with curcumin, fat-soluble vitamins on an empty stomach, high-dose zinc without copper. The cheapest performance gain in your stack is closing these leaks.
- Layer the stack by decade. The foundation does not change; what sits above it does.
References
- López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G (2023). Hallmarks of aging: an expanding universe. Cell, 186(2):243-278. https://pubmed.ncbi.nlm.nih.gov/36599349/. Retrieved 2026-06-07.
- Bhatt DL, Steg PG, Miller M, et al.; REDUCE-IT Investigators (2019). Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. New England Journal of Medicine, 380(1):11-22. https://pubmed.ncbi.nlm.nih.gov/30415628/. Retrieved 2026-06-07.
- Manson JE, Cook NR, Lee IM, et al.; VITAL Research Group (2019). Vitamin D supplementation trial: cancer and cardiovascular endpoint data (VITAL). New England Journal of Medicine, 380(1):33-44. https://pubmed.ncbi.nlm.nih.gov/30415629/. Retrieved 2026-06-07.
- Veronese N, Demurtas J, Pesolillo G, et al. (2020). Magnesium and health outcomes: an umbrella review of systematic reviews and meta-analyses of observational and intervention studies. European Journal of Nutrition, 59(1):263-272. https://pubmed.ncbi.nlm.nih.gov/30684032/. Retrieved 2026-06-07.
- Avgerinos KI, Spyrou N, Bougioukas KI, Kapogiannis D (2018). Effects of creatine supplementation on cognitive function of healthy individuals: a systematic review of randomized controlled trials. Experimental Gerontology, 108:166-173. https://pubmed.ncbi.nlm.nih.gov/29704637/. Retrieved 2026-06-07.
- Yoshino M, Yoshino J, Kayser BD, et al. (2021). Nicotinamide mononucleotide and muscle insulin sensitivity in prediabetic women: a randomized trial. Science, 372(6547):1224-1229. https://pubmed.ncbi.nlm.nih.gov/33888596/. Retrieved 2026-06-07.
- Singh P, Gollapalli K, Mangiola S, et al. (2023). Taurine deficiency as a driver of aging. Science, 380(6649):eabn9257. https://pubmed.ncbi.nlm.nih.gov/37289866/. Retrieved 2026-06-07.
- Lee C, Zeng J, Drew BG, et al. (2015). The mitochondrial-derived peptide MOTS-c in metabolic homeostasis: animal-model evidence. Cell Metabolism, 21(3):443-454. https://pubmed.ncbi.nlm.nih.gov/25738459/. Retrieved 2026-06-07.
- Pickart L, Margolina A (2018). Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. International Journal of Molecular Sciences, 19(7):1987. https://pubmed.ncbi.nlm.nih.gov/29986520/. Retrieved 2026-06-07.
- Seiwerth S, Milavic M, Vukojevic J, et al. (2021). Stable gastric pentadecapeptide BPC-157 in wound repair: preclinical review. Frontiers in Pharmacology, 12:627533. https://pubmed.ncbi.nlm.nih.gov/34267654/. Retrieved 2026-06-07.
- Khavinson VKh, Kuznik BI, Ryzhak GA (2012). Peptide bioregulators as a class of geroprotectors: experimental study results. Advances in Gerontology, 25(4):696-708. https://pubmed.ncbi.nlm.nih.gov/23734519/. Retrieved 2026-06-07.
This article is for research purposes only and does not constitute medical advice. Talk to your doctor before starting any supplement protocol, especially if you are on medication or managing a chronic condition.
Ready to layer the peptide research tier on top of a solid foundation? Explore the LEGACY NAD+ Protocol →
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.