
Research-based BPC-157 dosing guide: standard ranges by route, cycle structure, reconstitution steps, and sublingual vs injection dose equivalence.
There's no FDA-approved dose for BPC-157. That's the honest starting point, and every guide that skips it is setting you up for confusion later. If you want to see how these numbers translate into a structured regimen, our RESTORE recovery protocol is built on the same research base this guide walks through.
What does exist is a body of animal research, primarily in rat models, built up over more than two decades. Researchers working with BPC-157 today extrapolate from that data using established interspecies scaling methods, then adjust based on the delivery route they're using. BPC-157's regulatory and research status is one of the better-documented grey zones in peptide science, and understanding it matters before you interpret any dosing number. This content is published for research purposes only.
The dosing picture gets more complicated than most guides admit once you factor in how BPC-157 actually reaches your bloodstream. Subcutaneous injection, sublingual delivery, and standard oral capsules all behave differently, and that difference isn't minor. The route you choose changes how much of what you take actually reaches circulation, which means two guides quoting the same number in micrograms can be describing very different systemic exposures. This guide covers all three routes, along with the research extrapolation methodology, tissue-type applications, protocol cycles, and reconstitution for injectable protocols.
Key Takeaways
- No FDA-approved human dose for BPC-157 exists. Dosing ranges are extrapolated from animal literature using interspecies scaling, with 250–500 mcg/day as the conventional research range.
- Route of administration is the most important variable. Subcutaneous injection and validated VERISORB sublingual delivery achieve comparable systemic exposure at the same 250–500 mcg range; standard oral capsules require 500–1,500 mcg to compensate for lower GI absorption.
- Body weight doesn't significantly affect dosing in published animal protocols. Flat dosing is the convention.
- Titration, starting at 200–250 mcg for the first two weeks before increasing, produces cleaner baseline observations than opening directly at 500 mcg.
- Cycle structure matters: 4–12 weeks on, 2–4 weeks off, depending on the application. Continuous use makes response data harder to interpret.
- For injectable protocols, standard reconstitution is 2 mL bacteriostatic water into a 5 mg vial (2,500 mcg/mL). Store at 2–8°C; use within 28 days; never freeze reconstituted solution.
- VERISORB sublingual delivery removes the reconstitution requirement and achieves injection-comparable bioavailability, which changes the practical case for injectable-only BPC-157 protocols.
BPC-157 Dose: Standard Research Ranges
Think of the dosing picture like a two-step translation. First, you convert from rats to humans. Then you adjust for how the compound actually gets into your body.
The animal studies most commonly cited use roughly 10 micrograms per kilogram of body weight in rats. The FDA's published interspecies scaling guidance, used in what's called a human equivalent dose (HED) calculation, applies a conversion factor of approximately 6.2 between rats and humans, based on differences in body surface area relative to weight. Run that maths for an 80-kilogram person: roughly 130 mcg per day as the raw human equivalent.
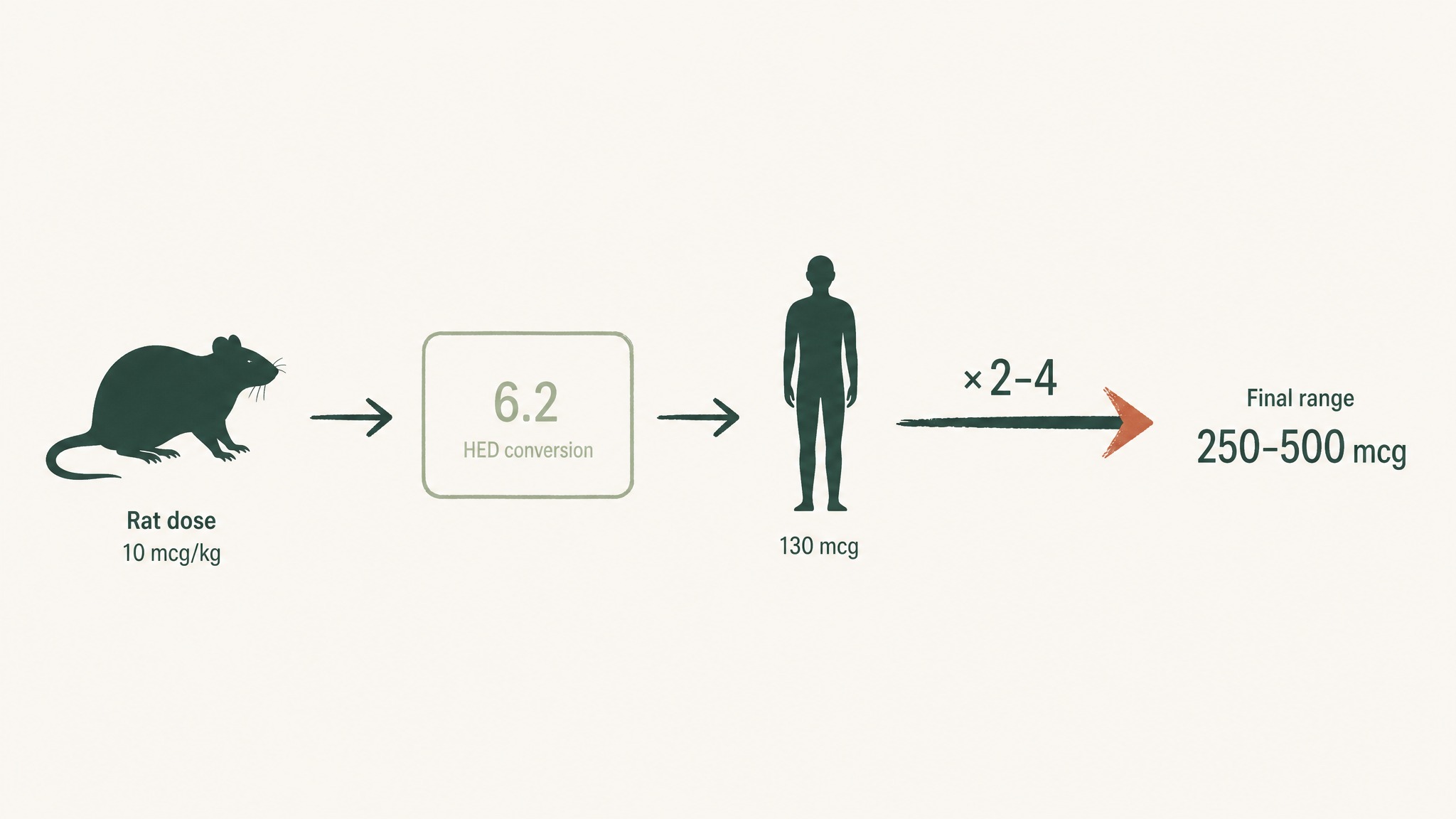
How rat study doses convert to human ranges through body-surface scaling and research-based multipliers.
Researchers typically dose higher than that raw HED number, often 2 to 4 times higher, based on observed response patterns in the research community and the fact that the rat studies themselves use a range rather than a single point. That's how the commonly cited 250–500 mcg window emerged.
| Range | Dose | Typical Research Context |
|---|---|---|
| Low | 200–250 mcg/day | Introduction phase; general systemic research |
| Standard | 250–500 mcg/day | Active tissue recovery, gut support protocols |
| High | 500–1,000 mcg/day | Intensive research windows; severe acute applications |
Body weight doesn't meaningfully shift the dose in most published animal protocols. Flat dosing, the same amount regardless of whether you're 65 kg or 100 kg, is the convention across the literature, including the long-running Sikiric et al. research programme (PMID 30915550). Some guides claim weight-based dosing is standard; the animal research mostly doesn't support that framing.
One thing the range table doesn't show: that 250–500 mcg number assumes injection-level bioavailability. Change the delivery route, and the effective dose changes too.
BPC-157 Dose by Administration Route
How much BPC-157 you absorb depends entirely on how it gets into your body. Think of your bloodstream as the destination, and your gut lining, oral mucosa, or injection site as three different roads to get there. Some roads have checkpoints and detours. Others are a clear run.
The same 500 mcg in a capsule doesn't deliver 500 mcg to your bloodstream. With subcutaneous injection, it does. That gap, bioavailability, is the single most important variable in BPC-157 dosing, and most guides collapse it into a single number without saying why.
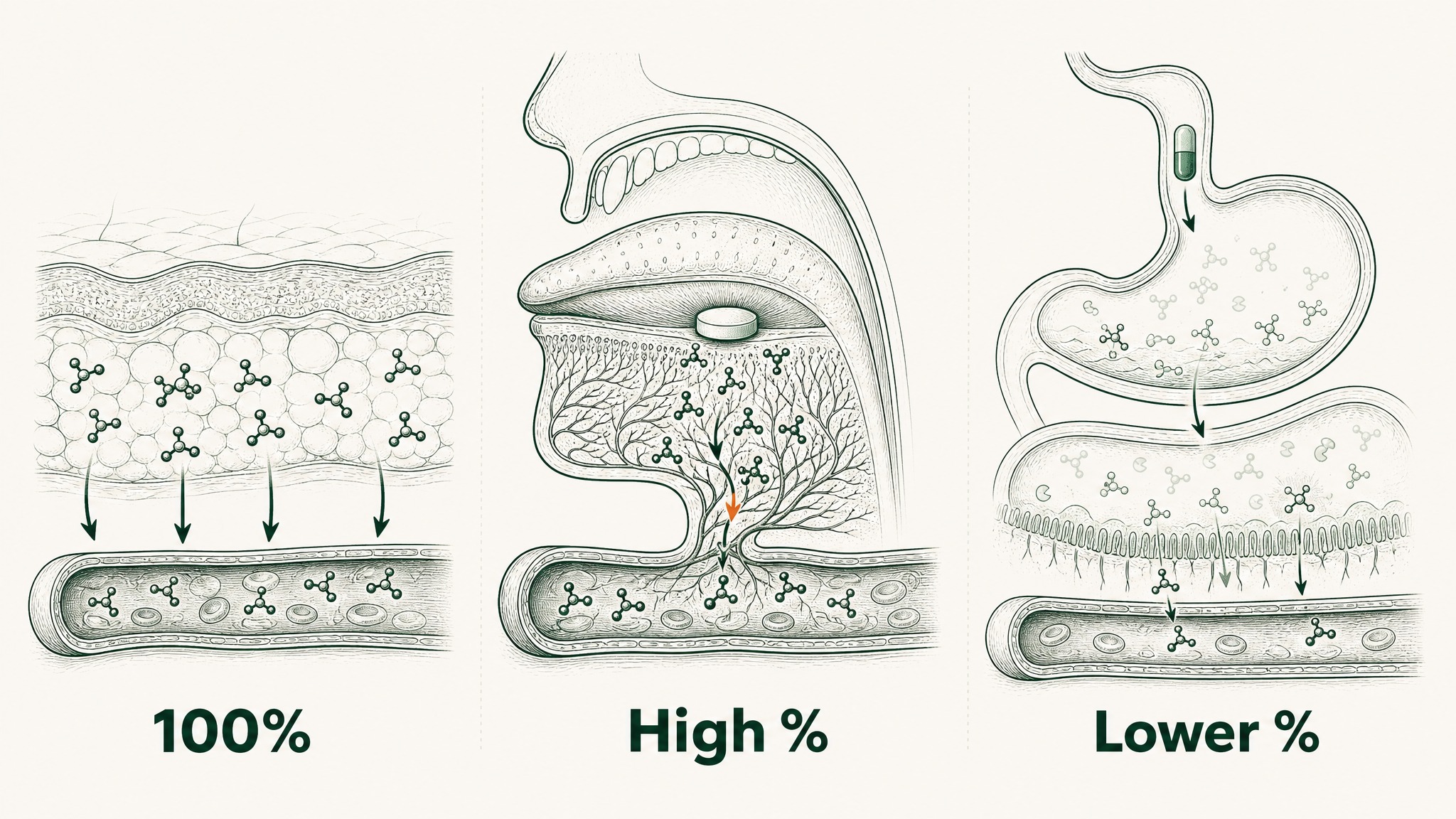
How BPC-157 reaches your bloodstream differently by injection, sublingual, or oral capsule.
Detailed breakdowns of how each route affects systemic exposure are covered in the oral vs injectable peptide bioavailability comparison.
Subcutaneous Injection
Standard BPC-157 injection dose: 250–500 mcg/day.
Subcutaneous injection, into the fat layer just under the skin, is the reference standard in BPC-157 animal research. Nearly all the published tendon, muscle, bone, and gut protection data comes from sub-Q or intraperitoneal injection protocols. Bioavailability is effectively complete: the full dose enters systemic circulation with minimal loss.
One distinct advantage of injection: you can administer it close to the site you're researching, near a specific tendon, joint, or affected area. Some researchers use this for localised protocols alongside the systemic dose.
Sublingual Delivery
Standard BPC-157 sublingual dose: 250–500 mcg/day, the same range as injection.
Sublingual absorption, dissolving a compound under your tongue, is the delivery method that most changes the BPC-157 dosing conversation. The underside of your tongue has a dense network of capillaries and a highly permeable mucosal membrane that allows compounds to pass directly into your bloodstream, bypassing your digestive system and liver entirely.
Standard oral capsules lose most of the peptide to stomach acid and digestive enzymes before it can absorb. Sublingual absorption sidesteps that problem. The key detail: VERISORB sublingual technology has been specifically validated for peptide delivery across the oral mucosa, with bioavailability comparable to subcutaneous injection.
That equivalence means the dose you need for VERISORB sublingual delivery is the same as the dose you'd use for injection, 250–500 mcg. You're not compensating for a bioavailability penalty.
Practical mechanics matter here: hold the dose under your tongue for 60 to 90 seconds. A fasted state improves mucosal absorption, the membrane is less occupied when you haven't just eaten, which is why morning protocols are common.
Standard Oral (Capsule or Powder)
Standard oral BPC-157 dose: 500–1,500 mcg/day, higher to compensate for reduced absorption.
BPC-157 is unusual among peptides in one respect: it's genuinely stable in gastric acid at very low pH levels. Most peptides get destroyed by your stomach. BPC-157 survives that acid environment, which means at least some of it reaches your intestines intact.
The problem is intestinal peptidase enzymes, the gut equivalent of scissors that cut peptide bonds, which further reduce how much ultimately absorbs into circulation. Researchers compensate by increasing the dose significantly. The working range for plain oral capsule protocols sits at 500–1,500 mcg per day, though exact absorption is variable and harder to predict than injection or validated sublingual delivery.
Route comparison:
| Route | Typical Research Dose | Relative Bioavailability | Notes |
|---|---|---|---|
| Subcutaneous injection | 250–500 mcg/day | High (reference standard) | Localised application possible |
| Sublingual (VERISORB) | 250–500 mcg/day | High (comparable to injection) | No needles; no reconstitution |
| Standard oral capsule | 500–1,500 mcg/day | Lower | Higher dose required; variable absorption |
For needle-averse researchers, the sublingual vs oral peptide absorption comparison matters more than the dose table alone. The delivery format determines whether the dose you take and the dose that actually reaches circulation are anywhere near the same number.
BPC-157 Dosing by Research Application
The standard 250–500 mcg range applies broadly, but the specific context shapes how researchers structure the protocol around it.
Tissue Repair and Recovery Research
BPC-157 dose: 250–500 mcg/day, injection or sublingual.
The tissue repair research base is the deepest area of the BPC-157 literature. A 2021 review in Frontiers in Pharmacology (PMID 34267654) documented consistent findings across tendon, ligament, muscle, and bone in animal models, all at doses within the standard range. A 2011 Journal of Applied Physiology study (PMID 21030672) showed significantly accelerated tendon outgrowth and cell migration in rat models through the FAK-paxillin pathway, a signalling chain that tells repair cells to divide and move toward damaged tissue.
Key protocol notes for this application:
- Duration: 4–8 weeks for active injury research
- Timing: Once daily, typically morning
- Route: Sub-Q injection or validated sublingual at equivalent dose; systemic delivery addresses multiple tissue sites without localized targeting
Gut Health and Intestinal Research
BPC-157 dose: 250–500 mcg/day.
The gut protection research is where BPC-157's origin matters. It was first isolated from a protein in human gastric juice, which is part of why the Sikiric et al. research group has spent decades studying its effects on ulcer models, intestinal barrier integrity, and NSAID-induced stomach damage. Their 2019 narrative review in Cell and Tissue Research (PMID 30915550) remains the most comprehensive summary of the evidence across gut-related endpoints.
Research suggests BPC-157 has cytoprotective effects, meaning it appears to preserve the stomach lining's structural integrity, particularly against damage caused by anti-inflammatories like ibuprofen and aspirin. A 2020 review in Current Pharmaceutical Design (PMID 32445447) documented these effects across multiple preclinical models.
One nuance for sublingual delivery in gut research: sublingual delivers the compound systemically through circulation rather than exposing the GI tract directly. That's a different exposure pattern from intraperitoneal injection, and worth factoring into how you interpret any response.
General Systemic and Longevity Research
BPC-157 dose: 200–300 mcg/day, lower-end, maintenance-style cycling.
Some researchers approach BPC-157 as a long-horizon maintenance protocol rather than an acute intervention: lower daily dose over an extended window, with a planned break, then repeat. This is less formally studied than injury-specific protocols, but it reflects how longevity-oriented researchers tend to approach compounds with broad systemic effects.
Members experience this as a lower-intensity approach that doesn't reset every 4–6 weeks. The 200–300 mcg range fits conveniently into once-daily sublingual protocols without reconstitution or injection logistics.
Sports Recovery Research
BPC-157 dose: 250–500 mcg/day.
Research suggests BPC-157's tissue repair mechanisms are relevant to recovery from intense training, specifically around tendon-bone junctions and muscle tissue. There are no human randomised controlled trials on this; the framing is mechanistic, grounded in the same animal data that underlies the tissue repair literature.
Timing within the day is debated among researchers: some dose post-exercise to coincide with the natural inflammation and repair window; others prefer fasted morning. Users report that neither timing approach appears clearly superior in available community data, so practical convenience usually drives the decision.
One consistent note: this is recovery-mechanism research, not performance enhancement research. There's no data on BPC-157's effects on strength, speed, or athletic output, only on tissue integrity and repair signals.
BPC-157 Protocol Structure: Cycle Length and Timing
Cycling, running the compound for a set period, then stopping, then starting again, is standard practice in BPC-157 research. The rationale isn't primarily toxicity concerns; it's about maintaining a clean observation window. Running a compound continuously makes it harder to distinguish its effects from baseline variation, and creates the possibility of receptor adaptation over time.
Think of it like tracking a variable in an experiment. If you're always adding the variable, you can't clearly see what changes when it's absent.
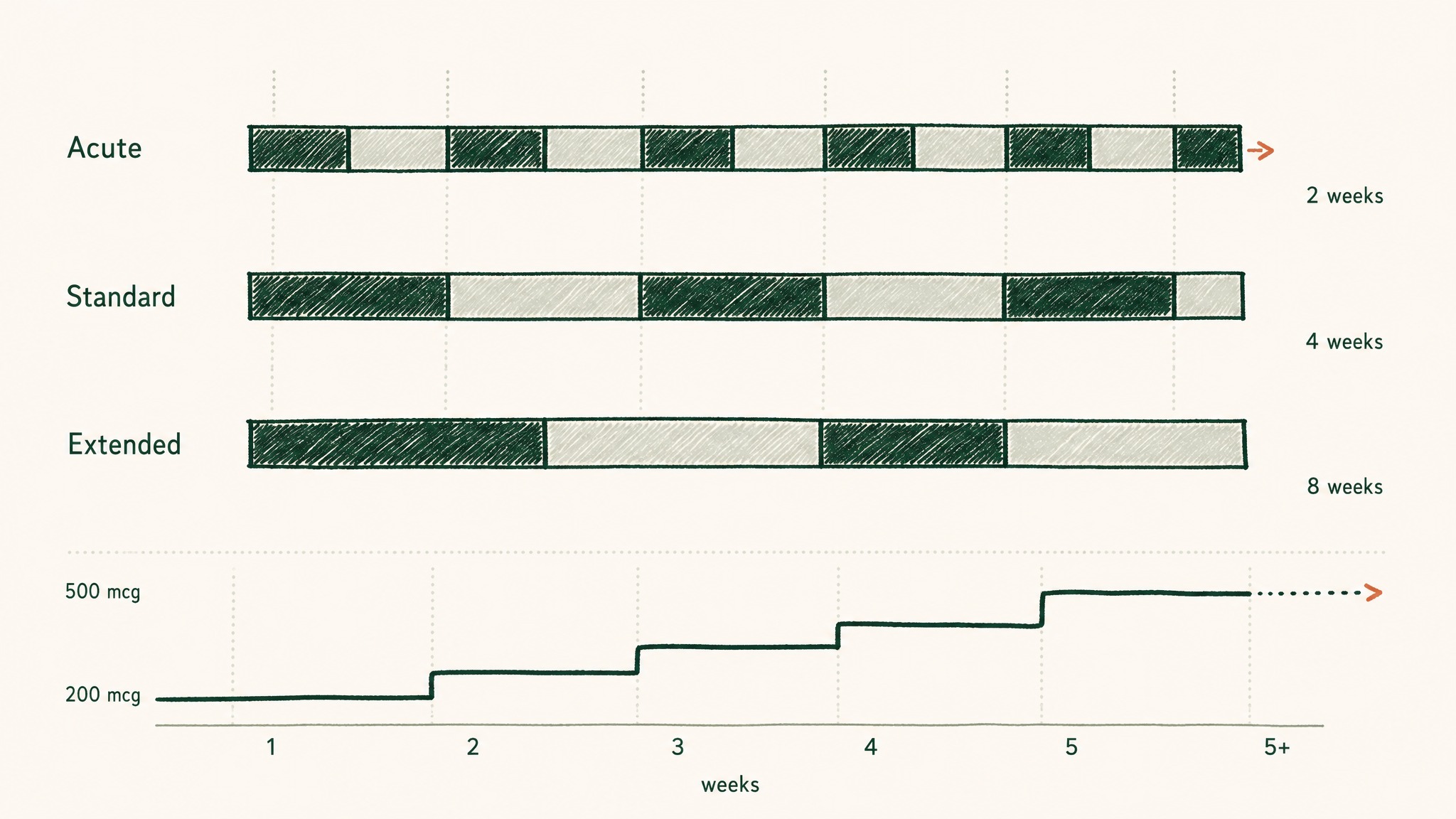
How BPC-157 cycles work: periods on and off, with dose ramping up over the first month.
Cycle structure by application type:
| Protocol Type | On Period | Off Period | Typical Application |
|---|---|---|---|
| Acute | 4–6 weeks | 2–3 weeks | Single injury or acute gut episode |
| Standard | 6–8 weeks | 2–4 weeks | General tissue recovery |
| Extended | 10–12 weeks | 4 weeks | Chronic or complex applications |
Daily timing: once vs twice daily
Once-daily dosing is simpler and produces consistent trough levels, a relatively steady low point between doses. Twice-daily split dosing produces smaller peaks and is sometimes used in intensive protocols to smooth the exposure curve. Neither approach has been clearly shown in animal data to produce superior outcomes. Most researchers default to once daily, and that's what most BPC-157 protocols are structured around.
Titration, starting low before reaching target dose:
Most competing guides open directly at 250–500 mcg with no ramp-up. For researchers new to BPC-157, a graduated start allows cleaner baseline observation and a more interpretable early window.
| Week | Dose | Rationale |
|---|---|---|
| 1–2 | 200–250 mcg/day | Establish baseline; observe initial response |
| 3–4 | 250–350 mcg/day | Incremental increase |
| 5+ | Up to 500 mcg/day | Full research dose if well tolerated |
Observation windows: Based on the animal literature, tissue-level effects appear in roughly the 2–4 week range. Systemic effects, gut, inflammation markers, more diffuse tissue patterns, show up in the 4–8 week window. No human RCT data confirms these timelines in people, but they're the reference frame most researchers use when planning their observation schedule.
Reconstitution Reference (Injectable Protocols Only)
This section is for researchers using the subcutaneous injection route. If you're using a pre-formulated sublingual protocol like RESTORE, you can skip this entirely, no reconstitution required.
BPC-157 for injection is typically supplied as a lyophilised powder (freeze-dried into a solid cake) in a sealed glass vial. You reconstitute it with bacteriostatic water, water with a small amount of benzyl alcohol added as a preservative, which prevents bacterial growth once the vial is opened.
Reconstitution steps:
- Allow the vial to reach room temperature before opening, cold reconstitution reduces peptide solubility
- Draw 2 mL of bacteriostatic water into a syringe
- Inject the water slowly into the BPC-157 vial along the inside wall, don't aim directly at the powder cake
- Swirl gently to dissolve; do not shake (agitation can degrade the peptide structure)
- The solution should be fully clear, if it remains cloudy or has visible particles, don't use it
Concentration reference:
| Water Volume | Vial Size | Concentration | 0.1 mL delivers |
|---|---|---|---|
| 2 mL | 5 mg (5,000 mcg) | 2,500 mcg/mL | 250 mcg |
| 1 mL | 5 mg (5,000 mcg) | 5,000 mcg/mL | 500 mcg |
The 2 mL reconstitution is the standard starting point. At 2,500 mcg/mL, you're drawing 0.1 mL for a 250 mcg dose, which is standard for peptide injection but requires accurate insulin syringes (typically 1 mL with 0.01 mL graduations).
Storage after reconstitution: Refrigerate at 2–8°C. Use within 28 days. Don't freeze reconstituted solution, freeze-thaw cycles degrade the peptide.
RESTORE™: BPC-157 via VERISORB Sublingual Delivery
Most BPC-157 protocols on the market are either injection-only (which requires sourcing bacteriostatic water, syringes, and doing your own reconstitution at exact concentrations) or plain oral capsules (which absorb poorly and require inflated doses to compensate).
VERO's RESTORE Protocol delivers 500 mcg BPC-157 per dose using VERISORB sublingual technology. The dose sits at the upper end of the standard research range for a specific reason: VERISORB's validated bioavailability means 500 mcg achieves injection-comparable systemic exposure without needles or reconstitution.

RESTORE delivers 500 mcg BPC-157 sublingually no needles, no mixing required.
Here's what that means practically:
- No syringes. No bacteriostatic water. No mixing.
- 500 mcg aligns with the standard research range for tissue repair and gut health protocols
- Hold under the tongue for 60–90 seconds in a fasted state for optimal mucosal absorption
- Pharmaceutical-grade sourcing, third-party tested
The VERISORB difference isn't a branding claim, it's the bioavailability gap that the route comparison table above makes visible. A plain oral capsule at 500 mcg doesn't deliver 500 mcg to your bloodstream. RESTORE does.
All VERO protocols are for research purposes only.
Frequently Asked Questions
What is the standard BPC-157 dose?
Based on animal research extrapolation, researchers typically work with 250–500 mcg per day. No standardised human dose exists, any source presenting a specific BPC-157 dose as clinically validated is misrepresenting the state of the evidence. Route of administration is critical: subcutaneous injection and validated sublingual delivery both work within this same range; standard oral capsules typically require 500–1,500 mcg to compensate for reduced GI absorption.
Is the BPC-157 dose the same for sublingual and injection?
With VERISORB-class sublingual delivery, yes. The key variable is bioavailability, how much of the dose actually reaches your bloodstream. A properly formulated sublingual protocol achieves systemic exposure comparable to subcutaneous injection at the same 250–500 mcg range. Standard oral capsules don't have that equivalence; they need roughly 2–3 times the dose to approach the same systemic exposure.
How long should a BPC-157 research protocol last?
Most structured protocols run 4–12 weeks depending on the application, followed by a 2–4 week off period. Acute applications, injury or gut focus, typically run 4–6 weeks. General systemic protocols often run 6–8 weeks. Extended protocols for chronic applications can reach 10–12 weeks with a longer break before the next cycle.
What's the difference between 250 mcg and 500 mcg of BPC-157?
250 mcg is the lower end of the standard research range, typically used for general systemic research, introduction phases, or maintenance-style cycling. 500 mcg is the upper standard dose, used in protocols targeting active tissue recovery and more intensive research windows. Many researchers titrate from 250 to 500 over the first four weeks rather than opening at the higher amount.
Can you take too much BPC-157?
Animal safety studies have not identified a toxic dose up to 10 mg/kg, dramatically higher than any research protocol. The 2021 Frontiers in Pharmacology review (PMID 34267654) noted that the lethal dose threshold (LD1) was never reached in preclinical safety testing. No human safety threshold data exists. This is a research peptide; all use should sit within a defined research context.
Does body weight affect BPC-157 dosing?
Mostly no, based on published animal protocols. The research literature overwhelmingly uses flat dosing rather than weight-adjusted amounts. An 80 kg researcher and a 65 kg researcher are typically working with the same 250–500 mcg protocol. The weight-based interspecies calculation is used to contextualise the animal-to-human translation, not to fine-tune individual doses.
References
- Sikiric P, et al. BPC-157 gastrointestinal and tissue repair research (narrative review). Cell and Tissue Research. 2019. https://pubmed.ncbi.nlm.nih.gov/30915550/. Retrieved 2026-05-17.
- Chang CH, et al. BPC-157 effects on tendon outgrowth and cell migration in rat models. Journal of Applied Physiology. 2011. https://pubmed.ncbi.nlm.nih.gov/21030672/. Retrieved 2026-05-17.
- Sikiric P, Seiwerth S, et al. BPC-157 cytoprotective and gastrointestinal protective effects (review). Current Pharmaceutical Design. 2020. https://pubmed.ncbi.nlm.nih.gov/32445447/. Retrieved 2026-05-17.
- BPC-157 wound healing and musculoskeletal tissue review. Frontiers in Pharmacology. 2021. https://pubmed.ncbi.nlm.nih.gov/34267654/. Retrieved 2026-05-17.
- Vukojevic J, et al. BPC-157 pharmacology and therapeutic applications review. Pharmaceuticals. 2025. https://pubmed.ncbi.nlm.nih.gov/40005999/. Retrieved 2026-05-17.
- U.S. FDA, Center for Drug Evaluation and Research. Guidance for Industry: Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers. July 2005. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/estimating-maximum-safe-starting-dose-initial-clinical-trials-therapeutics-adult-healthy-volunteers. Retrieved 2026-05-17.
Ready to start a structured BPC-157 research protocol without needles or reconstitution? Explore RESTORE →
RESTORE™
BPC-157Engineered around 0.5mg BPC-157 (arginate salt). Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.