
GHK-Cu is a copper-binding peptide your body makes less of every year after your twenties. Here's what the real research says about it, and how a structured protocol is typically built.
Introduction
By the time you're 60, your body is running on less than half the GHK-Cu it had in your twenties. That decline tracks closely with when skin starts looking different and cuts take longer to close over — because GHK-Cu is one of the small signalling molecules your body leans on to keep that maintenance work moving. A structured research protocol is built around replacing some of what your body stopped making on its own.
This article is published for research purposes only, so treat it as a map of what the science says rather than a set of medical instructions. GHK-Cu is a tiny copper-binding peptide — three amino acids linked together, with a copper ion attached, like a tiny key with a copper tooth cut into the end. Your liver and skin produce it naturally, just less of it with every passing decade.
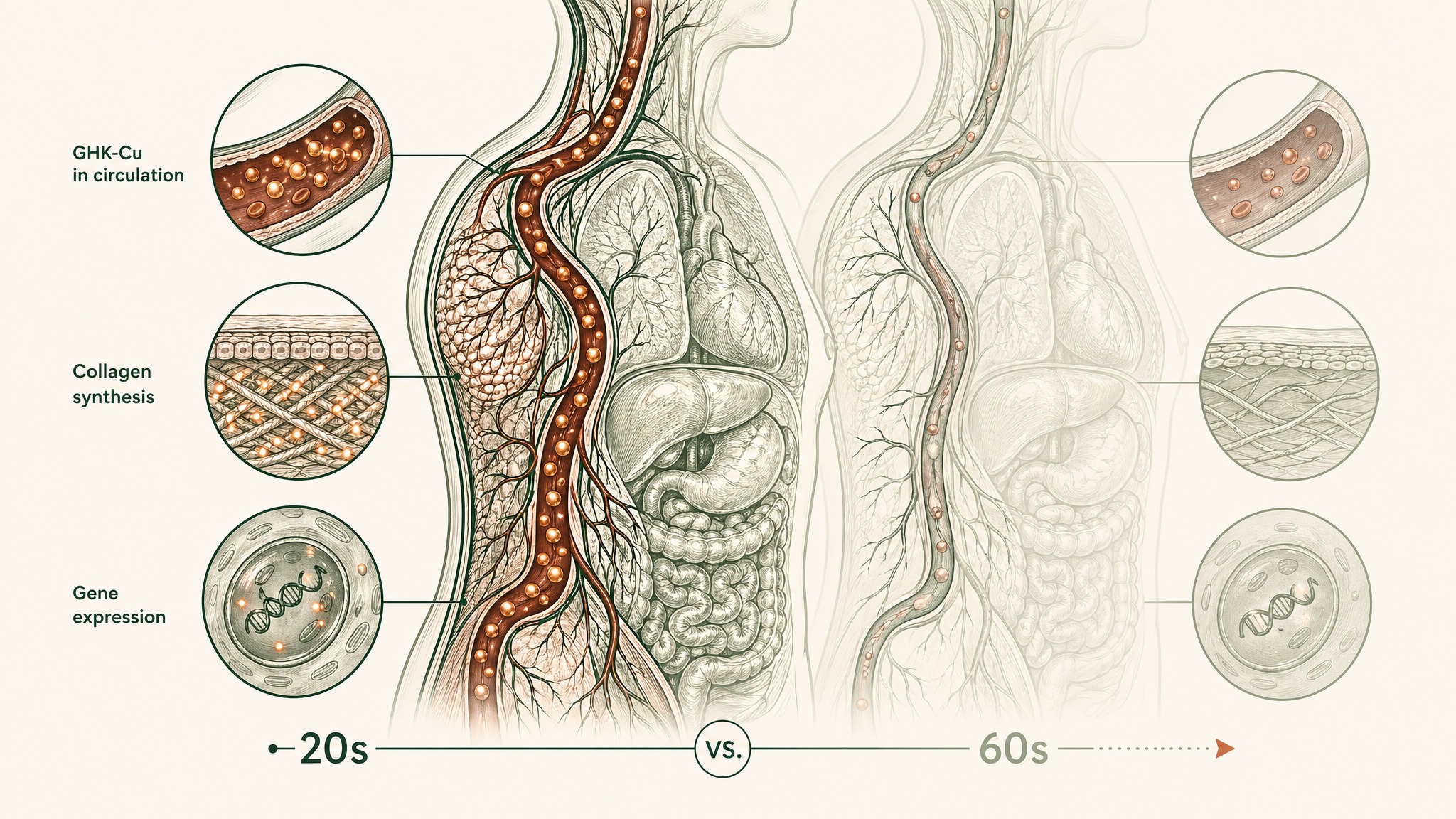
GHK-Cu levels in your liver and skin drop by more than half between your twenties and sixties.
Key Takeaways
- GHK-Cu was first identified in human blood serum back in 1973, and plasma levels drop by roughly 60% between your twenties and sixties — from about 200 nanograms per millilitre down to around 80 (Pickart & Margolina, 2018).
- Genomic analysis tied to the Broad Institute's Connectivity Map found GHK nudges expression on close to a third of all human genes by at least 50% — an unusually wide reach for one small molecule (Pickart et al., 2014).
- In a human skin study, women who applied a GHK-Cu cream for one month saw collagen increases in 70% of cases, versus 50% for vitamin C and 40% for retinoic acid under the same conditions (Pickart, Vasquez-Soltero & Margolina, 2015).
- In mouse models, liposome-packaged GHK-Cu shortened wound closure time to roughly 14 days and ramped up the growth factors that build new blood vessels (Wang et al., 2017).
- Delivery format decides almost everything: nearly every finding above came from an engineered carrier — injection, liposomes, or a specialised microemulsion — not a plain capsule.
This content is published for research and educational purposes only. It is not intended to diagnose, treat, cure, or prevent any disease, and it does not constitute medical advice. Readers should consult a qualified healthcare professional before making any decisions about their own health. Statements on this page have not been evaluated by the FDA. VERO's peptide products are supplied for research purposes only.
What GHK-Cu Is, and Why Your Body Makes Less of It Every Year
Think of GHK-Cu as a maintenance signal your body slowly turns down the volume on. In your twenties it's circulating at a level high enough to keep collagen production, tissue upkeep, and antioxidant defence ticking over at a decent baseline. By your thirties and forties that level is already sliding, quietly, with nothing dramatic to notice day to day.
Researchers Loren Pickart and M.M. Thaler first isolated the peptide from human blood serum in 1973 (PMID 4349963). Decades of follow-up work have tracked what happens as levels fall: plasma GHK runs at roughly 200 nanograms per millilitre in your twenties and drops to around 80 by the time you're 60 — a decline of almost 60% across four decades (Pickart & Margolina, 2018).
GHK-Cu levels drop nearly 60% from your twenties to your sixties.
That drop isn't a minor rounding error on a lab chart. A gene-expression analysis run against the Broad Institute's Connectivity Map found GHK shifts expression by at least 50% in roughly 31% of human genes it was tested against, split between genes turned up and genes turned down (Pickart & Margolina, 2018). A separate 2014 analysis using the same underlying dataset put the figure at 32.1% across more than 13,000 genes (Pickart, Vasquez-Soltero & Margolina, 2014).
Almost a third of your genome, nudged by one small molecule your body already recognises as its own.
That's the biological case for why a GHK-Cu protocol looks at more than one thing at once. You're not picking a single lane — skin, repair, or antioxidant defence. Research suggests all three sit downstream of the same signalling molecule, so a protocol built around it tends to track more than one outcome at a time rather than just one.
Three Things Researchers Actually Study When They Study GHK-Cu
Most of what gets said about GHK-Cu online collapses three separate research threads into one vague claim. It's worth pulling them apart, because the strength of evidence — and the type of study behind each — is different for each thread.
- Skin and collagen — the most human-study-backed thread, tested directly on skin
- Tissue repair — mostly animal and cell-culture research using engineered carriers
- Antioxidant and gene activity — largely laboratory and tissue-sample research
Three separate research threads behind GHK-Cu: skin collagen, tissue repair, and gene-silencing enzymes.
GHK-Cu and Skin: The Human Study Behind the Claim
Skin is where GHK-Cu has the clearest human research to point to, because it's also the easiest tissue to biopsy and measure directly.
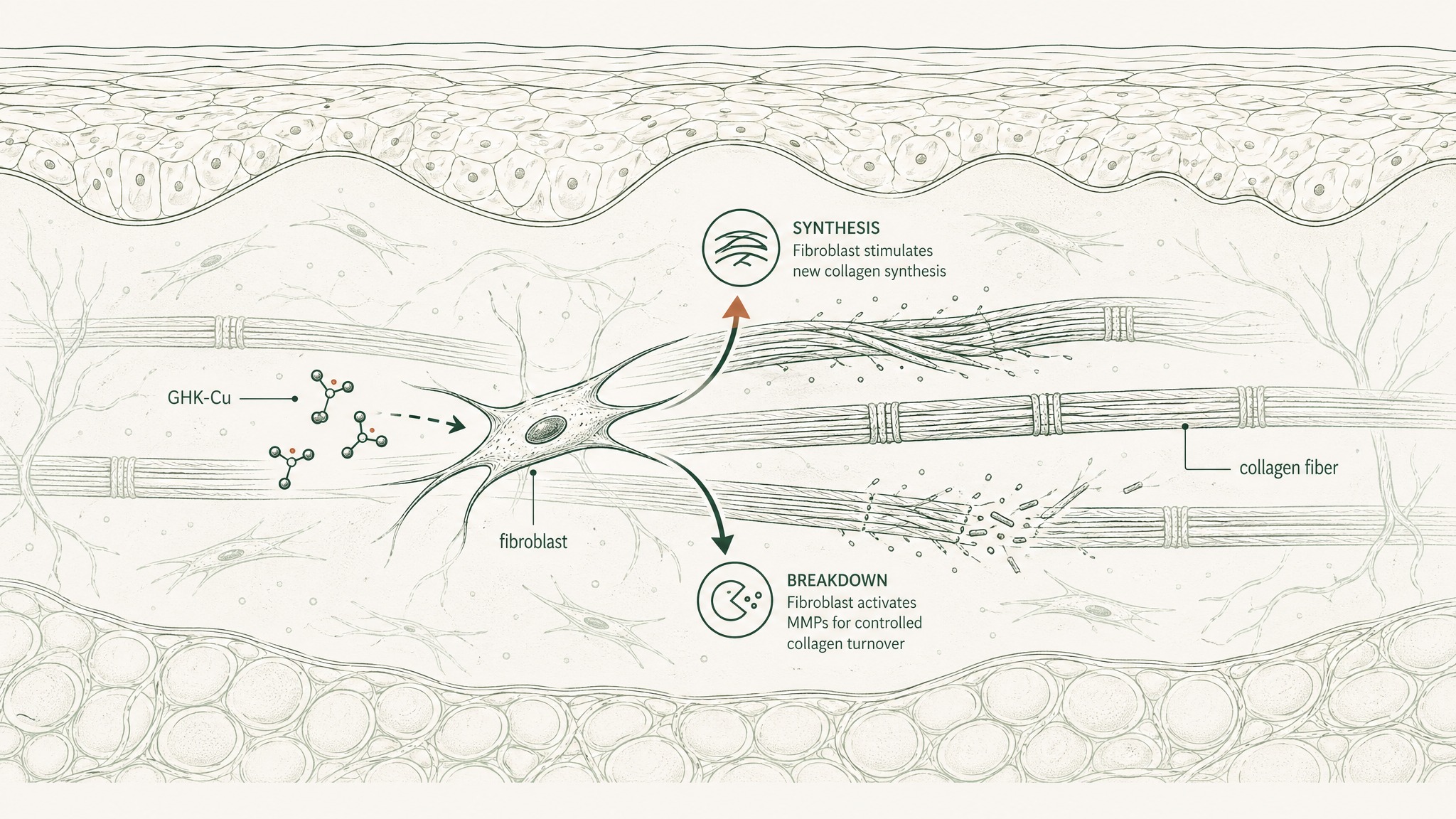
In a placebo-controlled study, Pickart, Vasquez-Soltero, and Margolina had women apply GHK-containing cream to their thighs for one month, then checked collagen production with skin biopsies and lab-based tissue analysis. Collagen increases showed up in 70% of the GHK-Cu group. That beat vitamin C cream, which came in at 50%, and retinoic acid (a vitamin A derivative commonly used in anti-aging skincare) at 40%, under the same study conditions (PMC4508379).
What's easy to miss in that number: the cream was doing this at concentrations as low as 1 to 10 nanomolar, a dose so small it's hard to picture — think a few drops in an Olympic swimming pool. At that dose, researchers found the peptide wasn't just switching collagen production on. It also appeared to regulate the enzymes that control collagen turnover, which is what keeps new tissue organised instead of just piling up.
Members experience the most noticeable skin changes in the four-to-eight-week range of a protocol, typically texture first, with density and elasticity building more slowly behind it.
GHK-Cu and Tissue Repair: What the Animal Research Found
Tissue repair research on GHK-Cu almost always uses an engineered carrier rather than the raw peptide, because unprotected peptide breaks down before it reaches the tissue that needs it. That detail matters for reading the studies honestly: the carrier is the reason the biology showed up at all.
In a 2017 study, Wang and colleagues packaged GHK-Cu inside liposomes (tiny fat-based bubbles that work like a protective shell around the peptide) and tested it in a mouse burn-wound model. In those animal models, researchers observed a 33.1% jump in the proliferation rate of the cells that build new blood vessels, wound closure shortened to roughly 14 days, and higher levels of two growth factors (VEGF and FGF-2) that drive new blood vessel growth and tissue rebuilding (PMID 28370978).
A separate 2023 study took a different engineering approach: Liu and colleagues built a stable ionic liquid microemulsion (a specially engineered delivery fluid) to push GHK-Cu into hair follicles in mouse models. Compared to unformulated controls, it delivered roughly three times more peptide to the target tissue and activated a signalling pathway involved in hair follicle cycling, alongside increases in VEGF and another growth factor called HGF (PMID 38026438).
Two research teams, two different tissues, and in both cases the carrier system was doing as much work as the peptide itself.
GHK-Cu and Antioxidant Activity: The Laboratory Findings
The antioxidant side of GHK-Cu research gets the least attention online, which is a little strange given how directly it connects to longevity-focused protocols.
A 2012 review by Pickart, Vasquez-Soltero, and Margolina pulled together laboratory findings on GHK-Cu's antioxidant and anti-inflammatory activity. Using gastric tissue samples, researchers recorded a 75% reduction in lipid peroxidation — the process by which free radicals damage the fats that make up cell membranes. The same review documented lower levels of two inflammation-driving proteins, TGF-beta and TNF-alpha, in the tissue samples tested (PMC3359723).
That review also flagged GHK as a strong inhibitor of HDAC enzymes. Here's the plain-English version: HDACs are enzymes that physically compress DNA, switching genes off in the process. As cells age, HDACs tend to get more active, silencing genes that would otherwise still be useful.
Laboratory data suggests GHK-Cu blocks some of that silencing — which is the mechanistic reason it keeps coming up in longevity-stack conversations alongside NAD+ precursors and sirtuin activators.
Why Delivery Format Decides Whether Any of This Applies to You
Here's the part that gets skipped in most write-ups: almost every finding above depended on how the peptide got into the tissue, not just what the peptide is.
Picture GHK-Cu like a delivery driver with a package that dissolves if it's left out in the rain. Injection, liposomal packaging, and specialised microemulsions are the "covered van" — they get the package to the door intact. A plain capsule swallowed on an empty stomach is the same driver, no van, walking through a downpour.
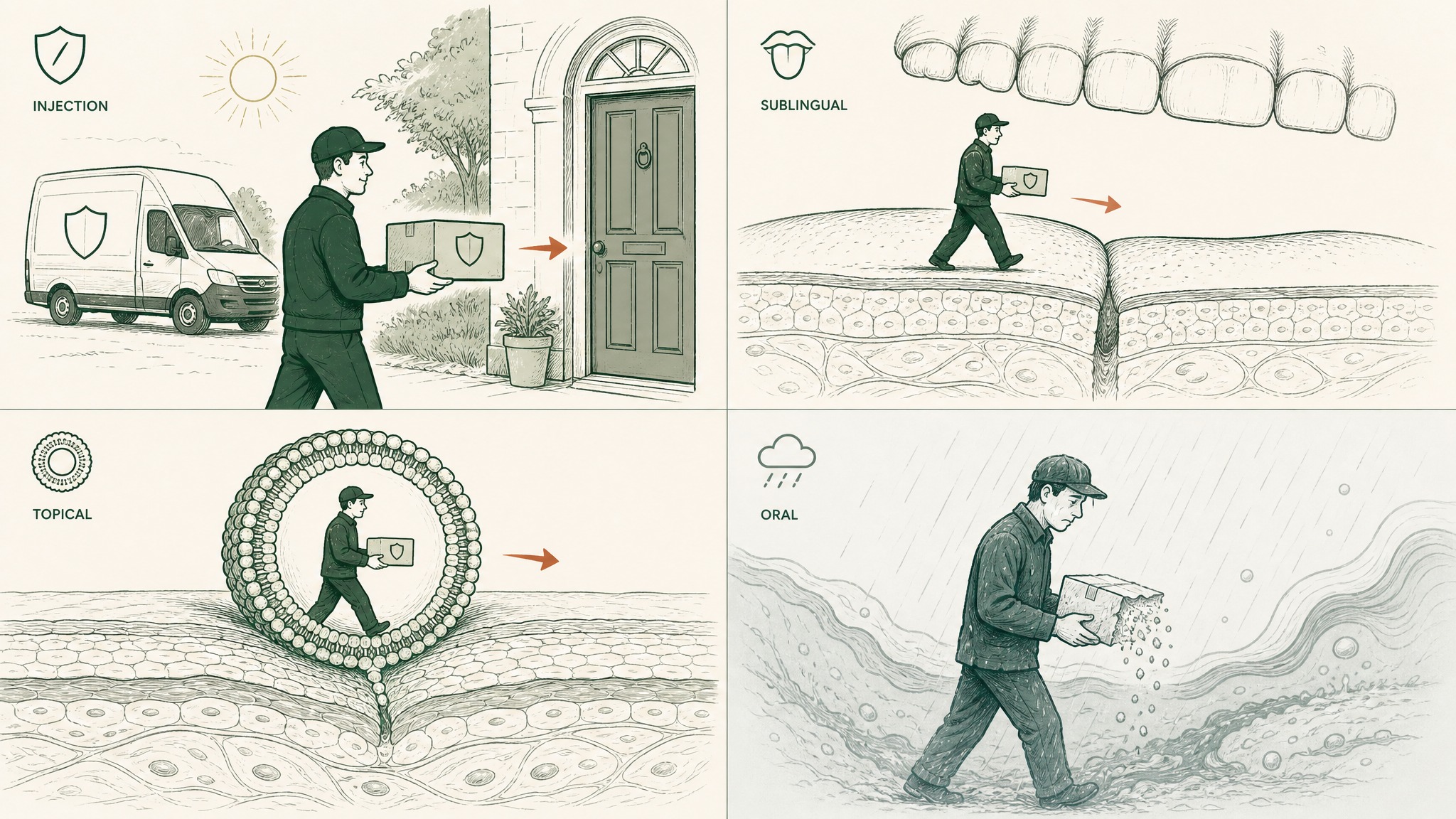
How four delivery routes determine whether GHK-Cu reaches its target intact or breaks down unused.
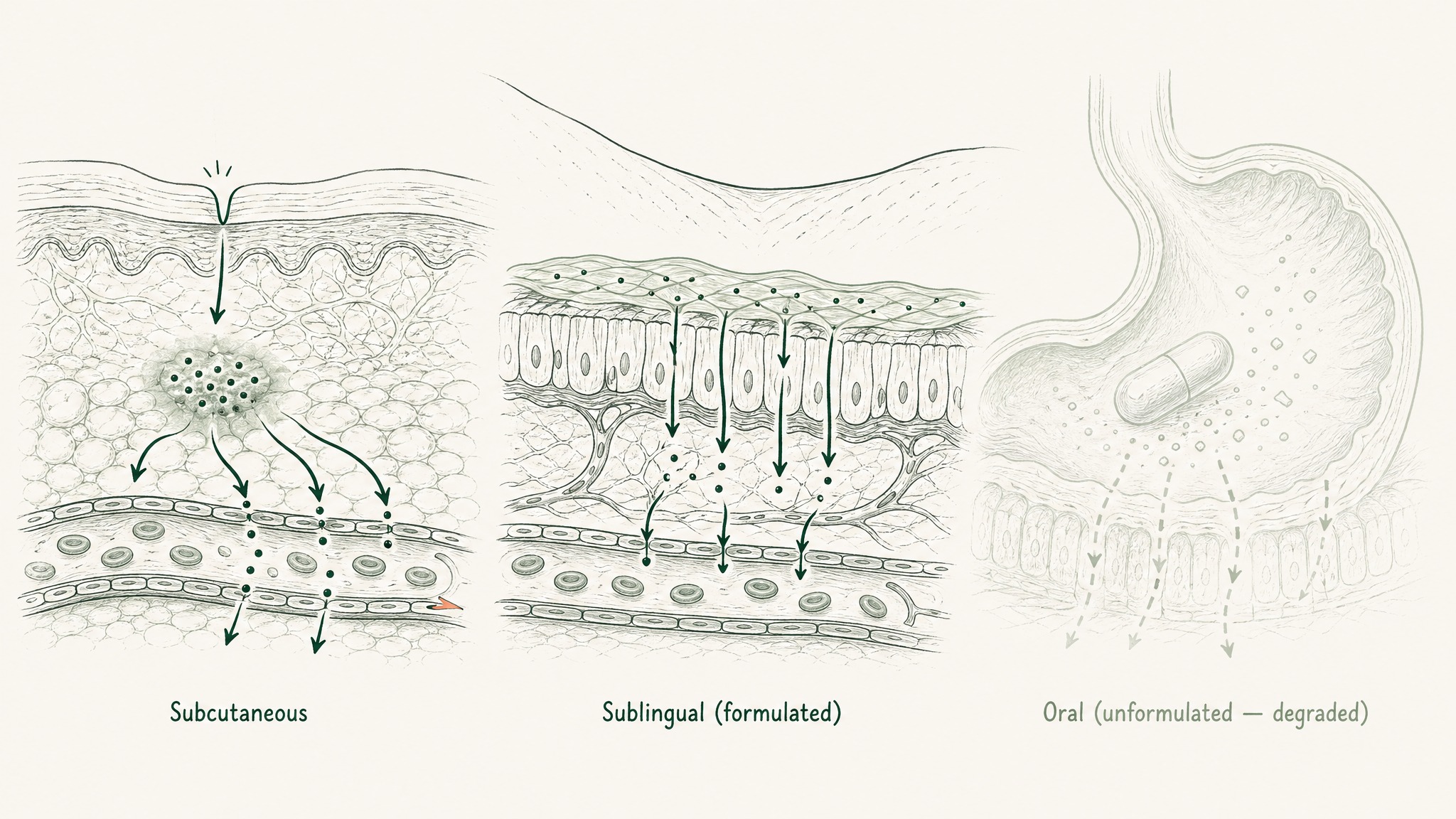
- Subcutaneous injection — direct systemic exposure, the route most research studies rely on
- Formulated sublingual — designed to cross the mucous membrane under the tongue rather than survive digestion
- Liposomal or microemulsion topical — engineered to push the peptide past the skin barrier for local effect
- Plain oral capsule — the peptide is broken down in digestion before it can do much of anything
Every VEGF finding, every HDAC result, every collagen number above came from a route in the first three categories, never the fourth. That's the single most practical takeaway from the research: the format matters as much as the peptide itself.
How a GHK-Cu Protocol Is Typically Structured
A protocol built around this research tends to follow the timelines the studies themselves used, because that's the only data anyone actually has to work from.
- Weeks 1–3 — early tissue-repair signals, based on the acute timeframes used in animal wound studies
- Weeks 4–8 — the window where the human skin study recorded measurable collagen change
- Beyond 8 weeks — longer cycles for antioxidant and gene-expression-linked outcomes, which build more slowly
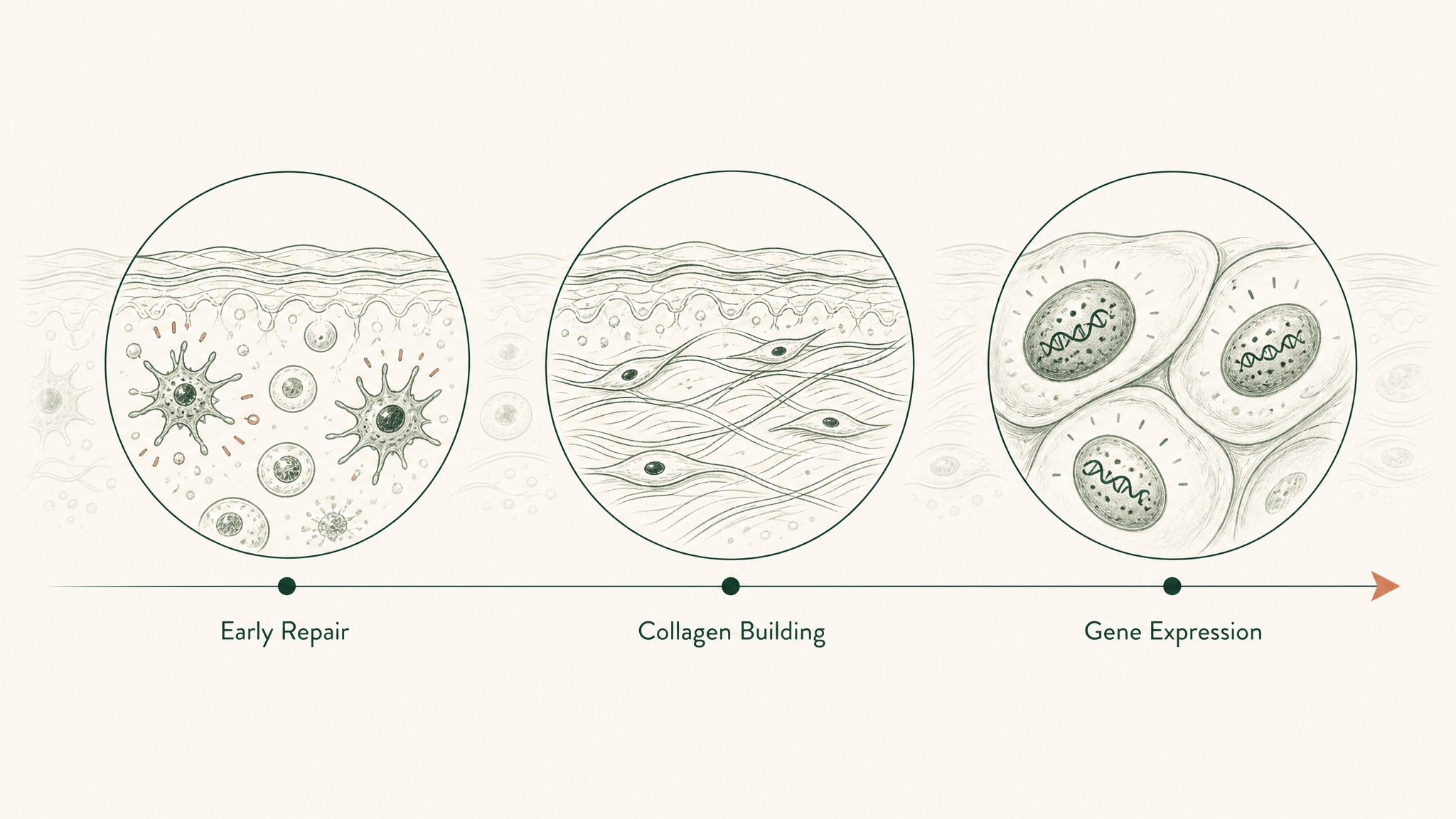
GHK-Cu's three-phase timeline: fast tissue signals, then collagen growth, then slower antioxidant and gene effects.
A common structure runs 8 to 12 weeks on, followed by a rest period before reassessing. No single study mandates that exact window — it's a practical compromise that gives both the fast repair signals and the slower skin and antioxidant signals enough runway to show up.
Stacking GHK-Cu With Other Research Peptides
GHK-Cu's spread across three biological domains is exactly why it tends to show up as a stack component rather than a standalone protocol.
- GHK-Cu + BPC-157 — BPC-157 research centres on gut and connective-tissue repair through separate signalling pathways; together they cover structural repair and matrix remodelling from two different angles
- GHK-Cu + TB-500 — TB-500 (thymosin beta-4) research points to cell migration and new blood vessel growth through actin-related mechanisms, which lines up with GHK-Cu's VEGF findings in the Wang et al. study above
- GHK-Cu + NAD+ precursors — NAD+ research runs through the sirtuin pathway, a separate route to a related goal: keeping gene expression patterns associated with younger cells running longer
Users report the NAD+ combination feels most noticeable at the energy and focus level over a full cycle, though the two compounds work through entirely distinct mechanisms and that combined effect hasn't been formally studied together.
What to Track During a Protocol
The research above translates into a short list of things worth watching if you're following a structured protocol.
- Skin texture and density — weekly photos in consistent lighting give you a rough proxy for the biopsy-measured collagen changes in the human study above
- Recovery from physical stress — how quickly soreness and minor strain resolve after training, loosely tied to the growth-factor findings from the animal wound research
- Inflammatory markers on bloodwork — TGF-beta and TNF-alpha are standard on most longevity panels and are the exact markers the 2012 laboratory review measured
- Sleep depth and mental clarity — subjective, but frequently reported by members alongside the gene-expression research above
None of these are diagnostic tools. They're just the same categories the underlying research actually measured, translated into things you can observe without a lab.
Frequently Asked Questions
What is GHK-Cu?
GHK-Cu is a small, naturally occurring peptide — three amino acids linked together with a copper ion attached — first identified in human blood serum in 1973. Your liver and skin produce it throughout life, though the amount your body makes tends to drop with age.
How much does GHK-Cu decline with age?
Research tracking plasma levels found GHK-Cu runs at roughly 200 nanograms per millilitre in your twenties and falls to around 80 by age 60 — close to a 60% drop across four decades (Pickart & Margolina, 2018).
Does GHK-Cu outperform vitamin C or retinoic acid for skin collagen?
In one placebo-controlled human study, a GHK-Cu cream produced collagen increases in 70% of the women tested over one month, compared with 50% for a vitamin C cream and 40% for retinoic acid, under matching conditions (PMC4508379). That's a single study, not a settled comparison across the wider skincare literature.
Why does delivery format matter so much?
Because nearly every notable finding in GHK-Cu research — the growth-factor changes, the gene-expression shifts, the wound-healing timelines — came from an engineered delivery route: injection, liposomal packaging, or a specialised microemulsion. A plain oral capsule isn't the same product as what the studies actually tested.
Can GHK-Cu be combined with other research peptides?
It's commonly stacked with BPC-157 for structural repair research, with TB-500 for angiogenic research given the overlapping VEGF pathway, and with NAD+ precursors for longevity-focused protocols. Each pairing works through a distinct mechanism rather than doubling up on the same one.
Who tends to look into a GHK-Cu protocol?
Mostly adults tracking the kind of age-related decline in skin, tissue repair, or antioxidant capacity described above, since the underlying decline becomes more noticeable from the thirties onward. This is published for research purposes only — anyone considering a protocol should talk to a qualified healthcare professional first.
Ready to look into a structured GHK-Cu research protocol? Start RADIANCE →
RADIANCE™
Coming SoonEngineered around 5mg GHK-Cu. Increases dermal thickness and systemic collagen synthesis
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.