A catalogue of the actual TB-500 doses used across rodent studies, the human pharmacokinetic trial, and practitioner protocols. For research purposes only.
If you've spent any time looking at TB-500 research, you've probably noticed the dose numbers don't sit still. One paper uses 100 micrograms. Another uses 6 milligrams. A community protocol talks about 10 mg weekly. The same compound, the same general idea, three numbers separated by two orders of magnitude.
This article is the catalogue. Not the framework (that lives in the TB-500 single-dose guide), not the weekly schedule (covered here), and not the standard range with reconstitution math (here). Just the actual TB-500 doses used across published research and reported practitioner protocols, organised by what the researchers were studying and why those particular numbers were chosen. All content is published for research purposes only.
Why are there so many different TB-500 doses?
Three things drive the spread.
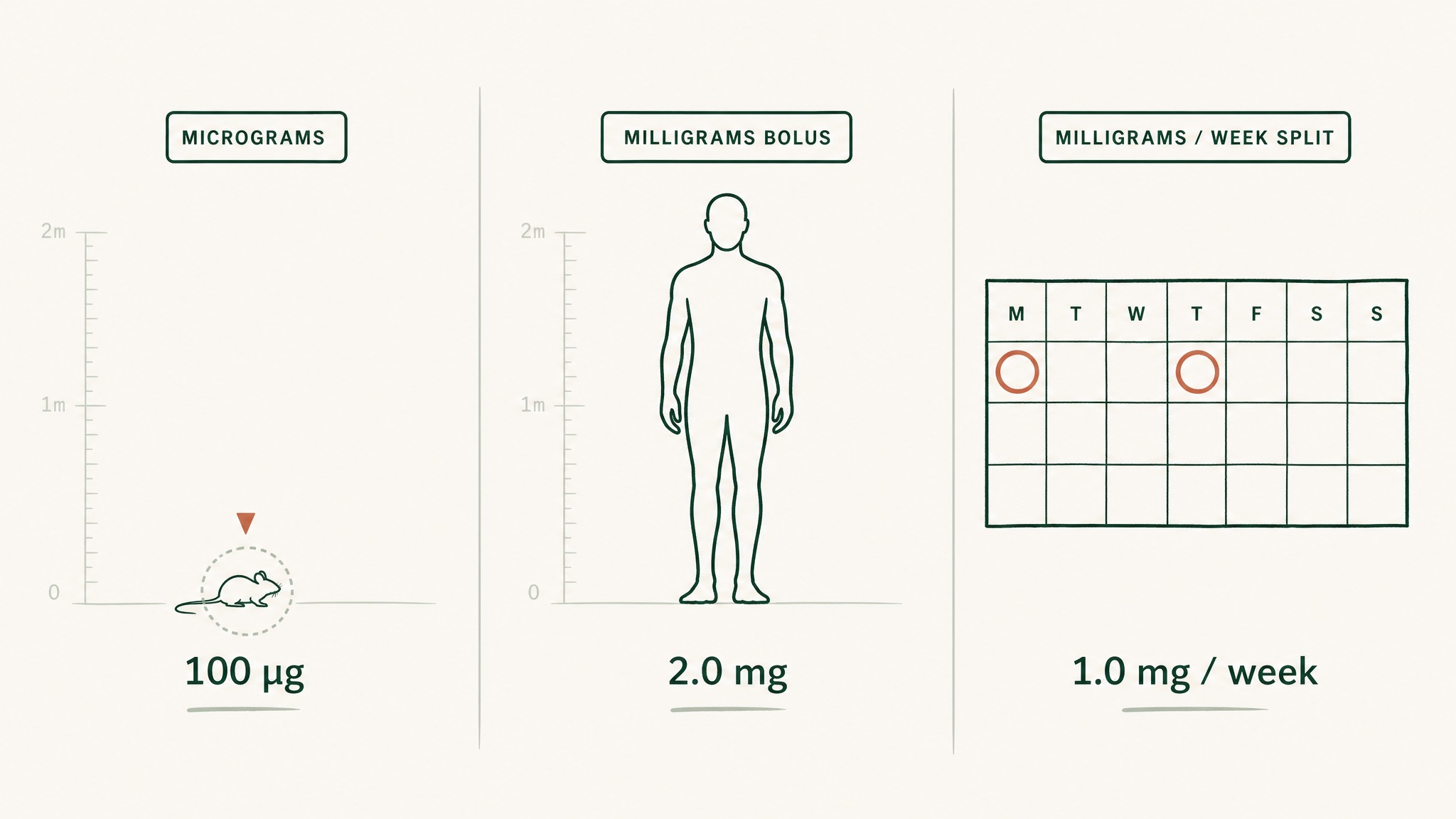
The first is species. Most TB-500 research lives in rodents, and rodent doses look small in absolute terms but huge in body-weight terms. A 250-microgram dose in a 25-gram mouse is the same relative exposure as roughly 5 mg in a 70 kg adult, before you apply any of the interspecies scaling adjustments the FDA recommends.
Why the same TB-500 dose looks different in mice, clinical trials, and weekly practitioner protocols.
The second is the molecule itself. Some papers use full-length Thymosin Beta-4 (the parent protein, 43 amino acids). Others use the TB-500 fragment that includes the actin-binding region. The doses don't always translate one-for-one because the molecular weights are different, so the same milligram number means different molar amounts.
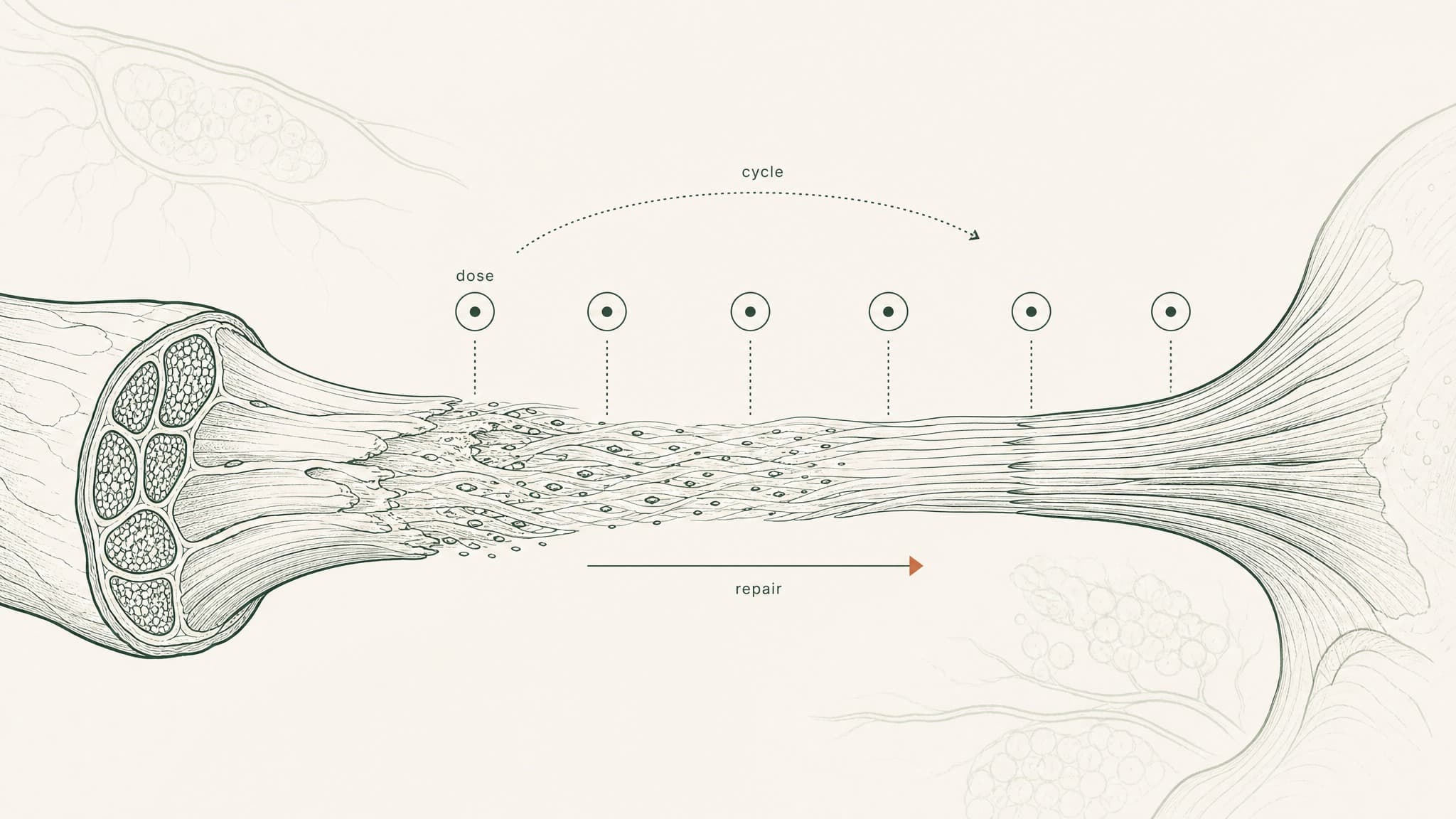
The third is the question being asked. A cardiac-injury study and a dermal-wound study aren't looking for the same effect, so they don't always use the same dose. Researchers studying acute repair tend to load higher; researchers studying maintenance signalling tend to dose lower and longer.
Here's what those differences look like in practice:
- Rodent doses: usually quoted in micrograms per administration
- Human PK trial doses: quoted in milligrams as a single bolus
- Practitioner-reported protocols: quoted in milligrams per week, split across two injections
Three different framings, three different scales. The catalogue below holds them side by side so you can see why the numbers cluster the way they do.
What TB-500 doses are used in rodent injury research?
The rodent literature is where most of the TB-500 dose evidence lives. Cardiac, dermal, neural, corneal, and tendon repair models all show up in the published work, and each one tends to anchor on its own characteristic dose range.
In our protocol design work at VERO, the rodent doses are the starting point we use to think about how the molecule signals in tissue, not the numbers we extrapolate from directly. The interspecies math gets you to the standard 5 to 10 mg per week human range, but the rodent studies are useful for a different reason: they tell you which dose corresponds to which mechanism, because every study reports the dose alongside the tissue outcome being measured.
Here are the doses that recur most often in the rodent literature:
| Injury model | Typical rodent dose per injection | Frequency | Source family |
|---|---|---|---|
| Cardiac repair (post-MI mouse) | Microgram-range bolus | Intraperitoneal, every 3 days | Bock-Marquette et al., Nature, 2004 |
| Dermal wound healing | Microgram-range topical | Daily | Malinda et al., dermal wound healing series |
| Corneal repair | Dilute drops at the application site | Multiple per day | Sosne et al., corneal repair series |
| Neural / stroke recovery | Milligram-per-kilogram range | Every 3 days | Morris et al., rat stroke-model series |
| Tendon and ligament repair | Sub-milligram per kg | Twice weekly | Practitioner-oriented preclinical reports |
A few things to call out. In preclinical research, full-length thymosin beta-4 has been observed to support cardiac repair signalling in mice at microgram-range doses per injection, with the Bock-Marquette group reporting effects within days of induced infarction. That paper is the most-cited starting point for the entire field, and it's where the early dose anchors come from.
The dermal and corneal doses look tiny in comparison, and they should: topical and ocular applications act at the site directly, so the dose your tissue sees is roughly the dose you applied. Injectable rodent doses have to clear the bloodstream, distribute through the body, and reach the target tissue, which is why they're orders of magnitude higher per administration.
What TB-500 doses are used in the human pharmacokinetic study?
There is exactly one published human pharmacokinetic study of thymosin beta-4 worth knowing about, and it gets cited in almost every discussion of TB-500 dosing.
Ruff et al. (2010), published in the Annals of the New York Academy of Sciences, ran a Phase 1 trial in healthy volunteers using single intravenous infusions of full-length thymosin beta-4. The trial tested a wide milligram-range dose ladder, from tens of milligrams at the bottom of the scale up to gram-range doses at the top, all delivered as a single IV bolus.
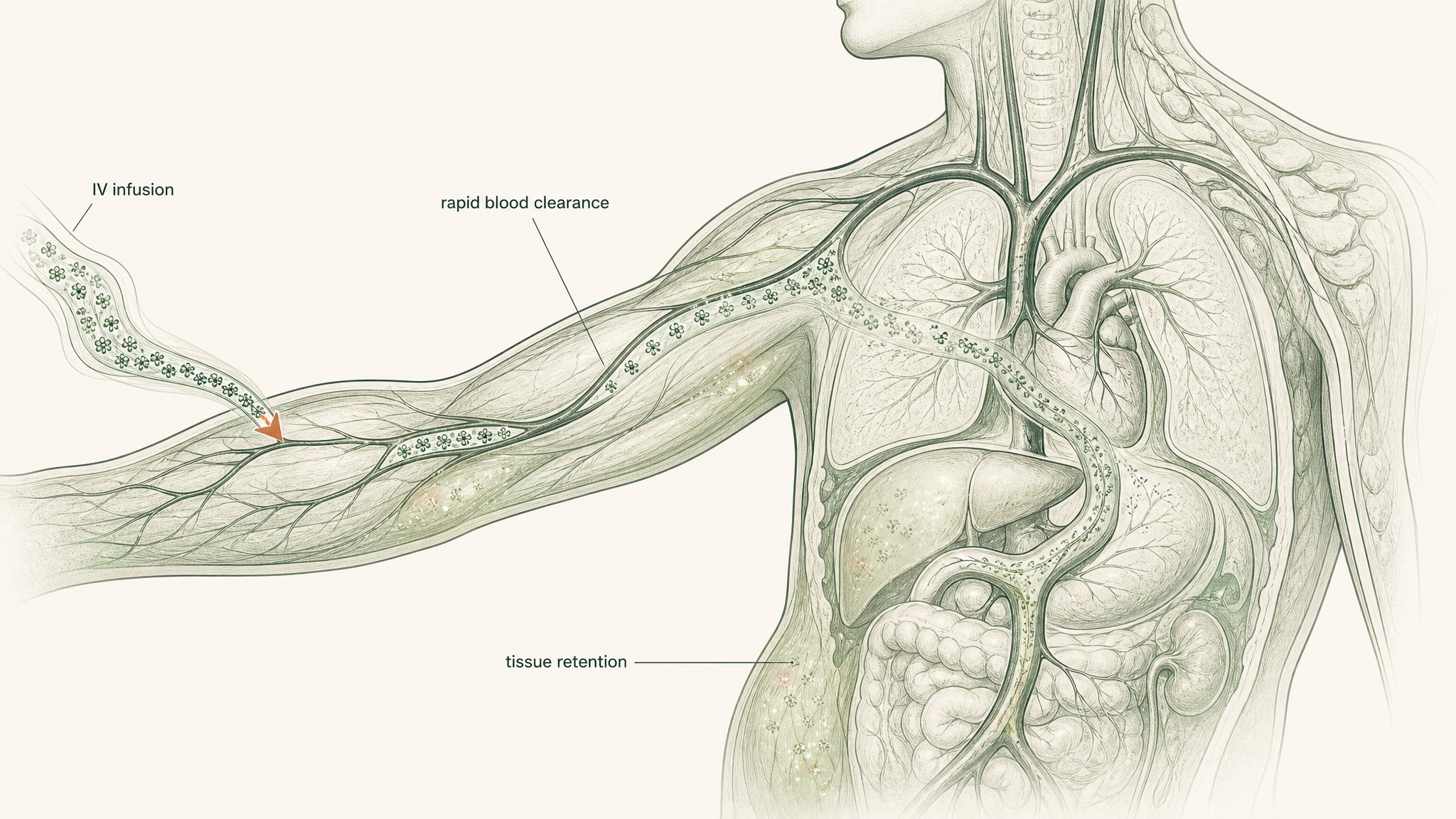
Thymosin beta-4 clears quickly from blood but lingers in tissue much longer.
These are single-dose, intravenous numbers. They are not the doses anyone uses in a research peptide protocol. They were chosen to map the molecule's pharmacokinetics across a wide range, not to mirror what self-experimenting researchers actually inject.
The trial reported good tolerability across the dose range and a short blood half-life after IV infusion. That short blood half-life is part of the reason the standard practitioner protocols converge on twice-weekly dosing rather than daily: the molecule clears quickly from circulation, but its signalling effects on tissue persist far longer than the bloodstream measurement suggests.
The Ruff trial used the parent molecule, not the TB-500 fragment. Researchers extrapolate from it cautiously, because the molecules aren't identical.
What practitioners take from this trial isn't the dose number. It's the safety signal and the half-life data. Both are used to argue that small subcutaneous doses, dosed twice weekly, are biologically reasonable, but neither validates the specific milligrams researchers actually use.
What TB-500 doses are reported in practitioner protocols?
This is the dose family most people are looking for when they search for TB-500 doses. None of it is FDA-approved. All of it is extrapolated from animal work and the Ruff PK trial. Users report a fairly narrow cluster of weekly numbers, with the exact dose chosen based on the research target and the loading window.
The numbers that recur most often in community-published protocols and practitioner-oriented sources:
- Maintenance research dose: about 2 to 2.5 mg per week, split across two subcutaneous injections
- Standard research dose: about 5 mg per week, split across two injections
- Higher research band: about 7.5 to 10 mg per week, split across two injections
- Loading window: about 10 to 20 mg per week for 4 to 6 weeks, often used in early acute-injury research before stepping down
Users report the 5 mg weekly band as the most common starting point. The maintenance band tends to be what researchers cycle into after a loading window has run its course, and the higher band shows up most often in research on connective-tissue repair.
A practical note from the protocol-design work we've done: the variance inside this range matters less than the variance across delivery routes. A 5 mg weekly subcutaneous dose and a 5 mg weekly sublingual dose deliver wildly different amounts to your bloodstream, and the dose-on-the-label conversation almost always skips that. The TB-500 dosing strategy guide covers the route-by-route adjustment in more detail.
How do TB-500 doses change for different research targets?
The dose number is rarely chosen in a vacuum. Researchers pick a number inside the standard band based on what they're actually studying.
Acute injury research
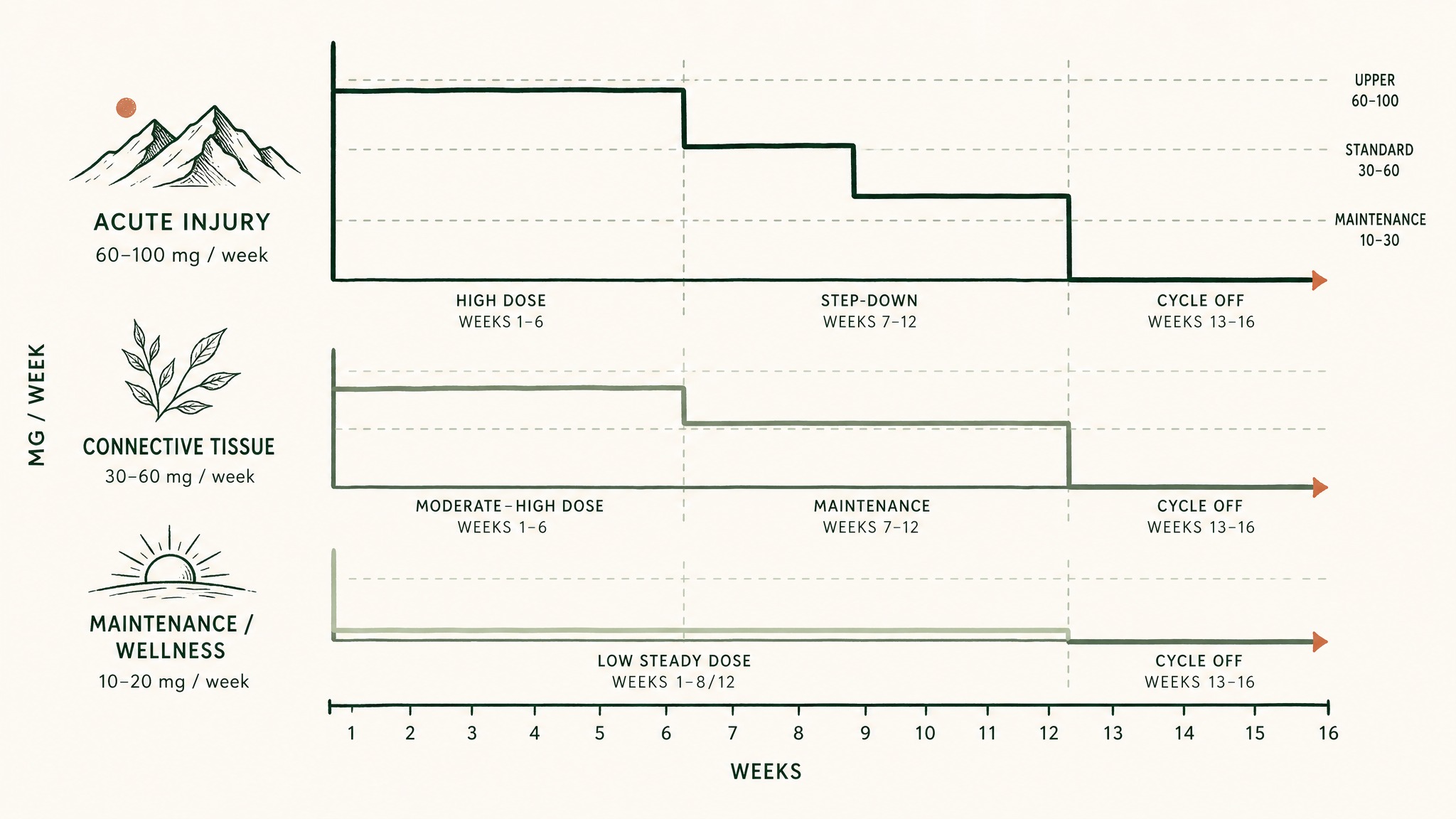
Three TB-500 dosing protocols: acute injury front-loads high, connective tissue sustains moderate-high longer, wellness maintains low steady.
Acute work usually loads. The pattern looks roughly like this:
- Run the upper band (10 to 20 mg weekly) for 4 to 6 weeks
- Step down to a standard band (5 mg weekly) once the acute window closes
- Cycle off for several weeks before reassessing
The loading rationale comes from the rodent cardiac and stroke work, where higher doses produced clearer tissue-level effects in the first weeks post-injury. Research suggests the acute window is when the signalling demand is highest in tissue-repair models, which is why practitioner protocols front-load.
Connective tissue research (tendon, ligament, muscle)
This is the research target most associated with TB-500 in the practitioner community. Doses cluster toward the upper end of the standard band, with longer loading windows because connective-tissue turnover is slower than muscle or vascular tissue.
A typical pattern looks like:
- Week 1 to 6: 7.5 to 10 mg weekly, split across two injections
- Week 7 to 12: 5 mg weekly maintenance
- Week 13+: cycle off, reassess
Maintenance / wellness research
The maintenance band (2 to 2.5 mg weekly) shows up in long-running research where the target isn't an acute injury but rather a continuous signalling effect. Members experience this as the typical post-loading band, often run in 8 to 12 week blocks with rest periods in between.
Connective and dermal combinations
Some protocols stack a low subcutaneous dose with topical applications for combined research on systemic and local repair signalling. The doses don't sum: the systemic dose still anchors on the standard band, and the topical use is layered separately.
What are the most common mistakes when comparing TB-500 doses?
Three errors show up over and over when people compare published TB-500 doses across studies.
Treating "dose" as one thing. A "dose" can mean what you draw up, what reaches your bloodstream after route loss, or what adds up over a week. Each is a different number, and they can differ by an order of magnitude depending on the route. The single-dose framework article walks through all three framings.
Comparing full-length thymosin beta-4 doses to TB-500 fragment doses one-for-one. They aren't the same molecule, and even when the milligram numbers look similar, the molar amounts differ. The Ruff PK trial used the parent protein; most rodent injury work also used the parent. Practitioner protocols use the fragment. Translating between them takes more than a unit conversion.
Reading rodent doses literally. A 6 mg/kg rodent dose does not mean a 6 mg/kg human dose. The FDA's body-surface-area scaling reduces the human-equivalent dose by roughly 12-fold for mice and 6-fold for rats, which is why the human extrapolated range lands at around 5 to 10 mg per week, not the hundreds of milligrams a literal mg/kg conversion would suggest.
The dose on the label is a starting assumption, not a guarantee of what your tissue sees.
How does delivery route change the TB-500 dose conversation?
The same TB-500 dose delivered three different ways produces three different blood and tissue exposures. This isn't a detail; it's the single most important variable nobody adjusts for when comparing protocols.
Here's what changes:
How TB-500 absorption changes dramatically depending on whether it's injected, placed under the tongue, or swallowed.
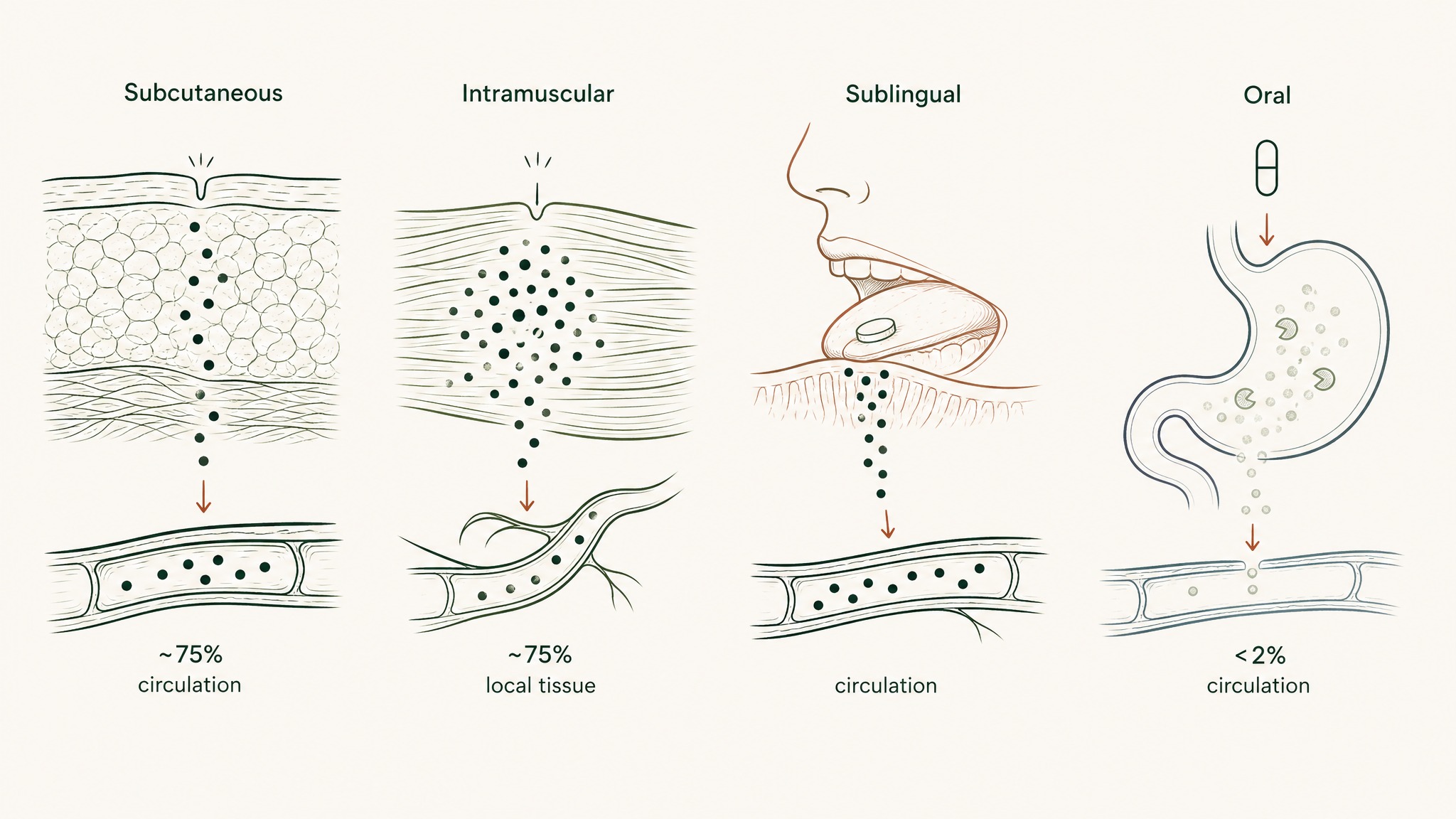
- Subcutaneous injection: roughly 70 to 80% of the dose enters circulation, though peak time is slower than IV
- Intramuscular injection: similar bioavailability to subcutaneous, faster peak in the local tissue
- Sublingual delivery (the route VERO research uses for RESTORE): bypasses the gut entirely, with absorption profiles that depend heavily on the formulation
- Oral capsules: typically less than 2% reaches circulation because peptides are destroyed by stomach acid and gut enzymes before they ever get a chance to absorb
This is the part of the dose conversation that gets skipped most often. A 5 mg weekly subcutaneous protocol and a 5 mg weekly oral capsule protocol are not the same protocol. Different bioavailability profiles change the dose conversation entirely.
For delivery formats that protect peptide structure during absorption, VERISORB is the sublingual platform VERO uses to keep more of the peptide intact through delivery. The standard dose comparison numbers in the literature assume injectable administration unless explicitly stated otherwise.
How long should a TB-500 dose cycle run?
The cycle length is part of the dose conversation, because the total exposure over time is what shapes outcomes more than any single injection.
Research convention clusters around these cycle structures:
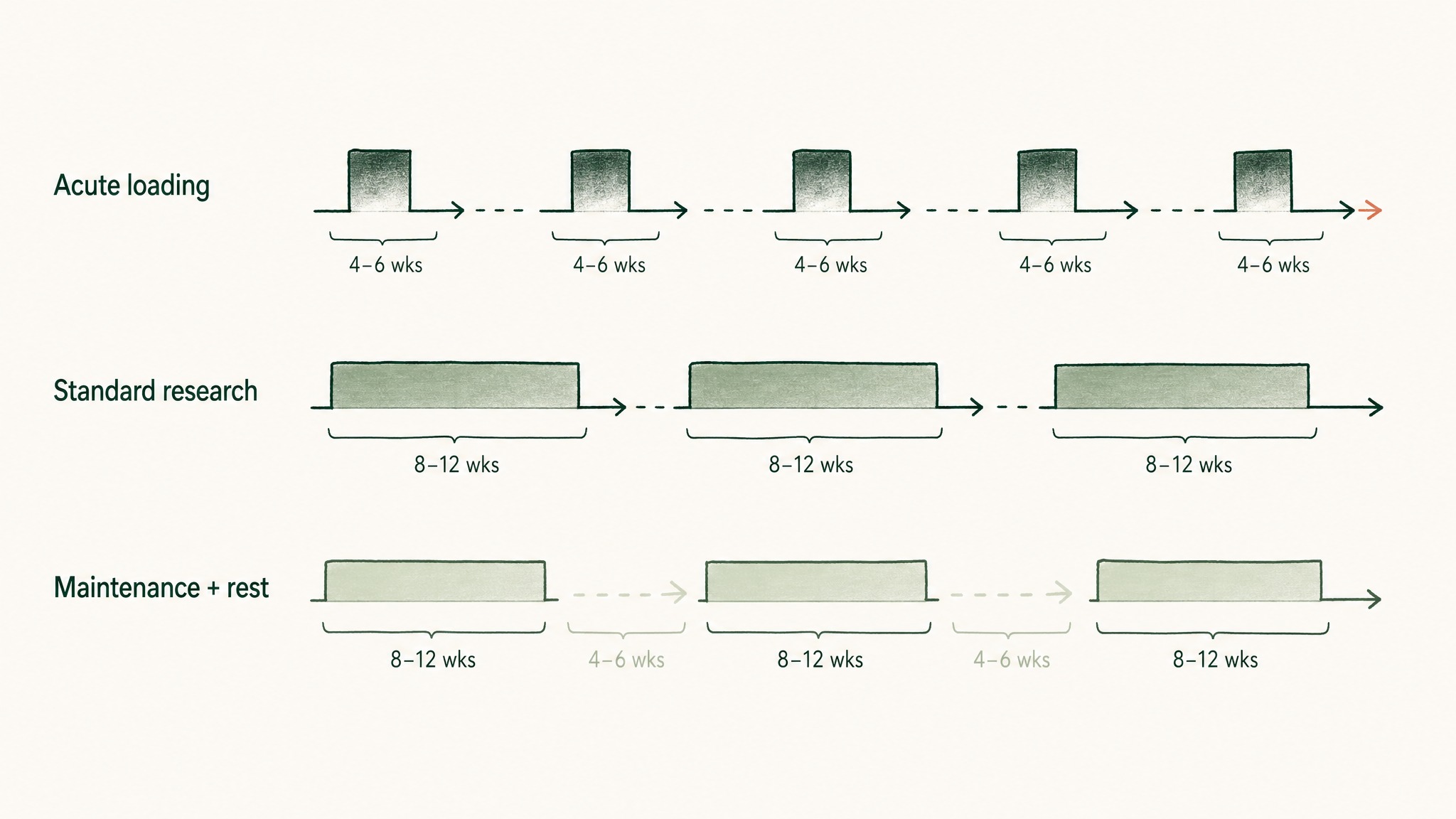
Three common TB-500 cycle structures: loading, standard, and maintenance with built-in rest periods.
- Acute loading cycle: 4 to 6 weeks at the upper band
- Standard research cycle: 8 to 12 weeks at the standard band
- Maintenance research cycle: continuous blocks of 8 to 12 weeks at the lower band, with 4 to 6 weeks off between blocks
The off-cycle is part of the protocol, not an afterthought. The rationale is straightforward: continuous high-dose signalling research is rare in the published literature, and most practitioner protocols build in rest periods to mirror the natural pulsatile signalling of the parent molecule.
A cycle that runs too long without rest tends to flatten observed effects. Users report that the most consistent observations come from cycled protocols with clear loading, maintenance, and rest phases, rather than from continuous high-dose research.
Key Takeaways
- TB-500 doses vary across two orders of magnitude in published research, driven by species, molecule (parent vs fragment), and research target
- Rodent injury studies typically use 100 to 500 mcg per injection, scaled to body weight, in models from cardiac repair to corneal healing
- The one published human PK trial (Ruff et al., 2010) tested IV doses from 42 mg to 2,520 mg single bolus, but those numbers are not what practitioner protocols use
- Practitioner-reported TB-500 doses cluster around 2 to 20 mg per week subcutaneously, split across two injections, with the 5 mg weekly band as the most common starting point
- Research target shapes dose choice: acute loading sits high (10 to 20 mg/week), standard research mid (5 mg/week), maintenance low (2 to 2.5 mg/week)
- Delivery route changes the dose conversation entirely; sublingual and oral protocols are not directly comparable to injectable doses at the same milligram label
- Cycle length and off-cycle rest periods matter as much as the single-injection dose number
- All TB-500 dosing in research peptide use is extrapolated, not FDA-approved; all content here is published for research purposes only
References
- Bock-Marquette et al. (2004). Thymosin beta-4 in cardiac cell migration, survival, and repair signalling: mouse infarct model. Nature 432, 466-472. https://pubmed.ncbi.nlm.nih.gov/?term=Bock-Marquette+thymosin+beta-4+nature+2004. Retrieved 2026-06-10.
- Malinda et al. Thymosin beta-4 in dermal wound repair: rodent-model evidence series. Journal of Investigative Dermatology / FASEB Journal. https://pubmed.ncbi.nlm.nih.gov/?term=Malinda+thymosin+beta+wound+healing. Retrieved 2026-06-10.
- Sosne et al. Thymosin beta-4 in corneal wound repair: rabbit-eye model evidence series. Experimental Eye Research / Annals NY Acad Sci. https://pubmed.ncbi.nlm.nih.gov/?term=Sosne+thymosin+beta-4+corneal. Retrieved 2026-06-10.
- Morris et al. Thymosin beta-4 in neural recovery: rat stroke-model evidence series. Neurorehabilitation and Neural Repair / Annals NY Acad Sci. https://pubmed.ncbi.nlm.nih.gov/?term=Morris+thymosin+beta-4+stroke. Retrieved 2026-06-10.
- Ruff et al. Phase 1 single-dose intravenous thymosin beta-4 in healthy volunteers: pharmacokinetic and tolerability evaluation. Annals of the New York Academy of Sciences, 2010. https://pubmed.ncbi.nlm.nih.gov/?term=Ruff+thymosin+beta-4+pharmacokinetics. Retrieved 2026-06-10.
- Goldstein et al. Thymosin beta-4: regenerative-peptide biological roles and basic findings review. Expert Opinion on Biological Therapy. https://pubmed.ncbi.nlm.nih.gov/?term=Goldstein+thymosin+beta-4+regenerative+review. Retrieved 2026-06-10.
- FDA Center for Drug Evaluation and Research. Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers (guidance document, body-surface-area scaling tables). https://www.fda.gov/regulatory-information/search-fda-guidance-documents/estimating-maximum-safe-starting-dose-initial-clinical-trials-therapeutics-adult-healthy-volunteers. Retrieved 2026-06-10.
Working through a TB-500 research protocol? VERO's RESTORE protocol uses the VERISORB sublingual delivery system, published for research purposes only.
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.