What NAD supplement side effects do human trials actually report? Flushing, GI upset, sleep, methylation, and who should avoid them. For research purposes only.
If you've spent any time on NAD supplements, you've probably noticed the side-effects conversation is weirdly missing. Most product pages skim past it. Most longevity podcasts skip it entirely. This guide pulls together what human trials actually report, what's been raised in regulatory notices, and what to watch for if you choose to experiment, all for research purposes only.
The honest summary, before you scroll: published trials on nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) at typical doses tend to look very clean. Most users report nothing. A small minority report flushing, mild gut upset, or sleep changes. The bigger questions sit one layer down: methylation strain over time, regulatory limbo around NMN, and a few preclinical signals around cancer biology that nobody in the supplement aisle is talking about.
The short version:
- At the doses tested in human trials, NAD precursors look well tolerated overall.
- Reported side effects cluster around flushing, nausea, headache, and sleep disturbance at the higher end of dosing.
- Methylation strain is the slow-burn concern most products ignore.
- The US FDA pulled NMN out of the dietary supplement category in 2022, and the regulatory dust hasn't fully settled.
- Some groups (pregnancy, active cancer, certain medications) sit outside the research base entirely, and the cautious move is to opt out.
Are NAD supplements actually safe?
The first thing to get straight: "NAD supplement" is a category, not a single molecule. Most bottles contain a precursor your body rebuilds into NAD+: usually NR (nicotinamide riboside) or NMN (nicotinamide mononucleotide). A few contain nicotinamide or niacin. Direct NAD+ is rare and behaves differently still.
That matters for safety because each form has its own side-effect profile. Niacin is the famous flusher. Nicotinamide can cause GI upset at higher doses. NR and NMN both look gentler in the short-term trials we have. Lumping them together is the first thing that confuses readers.
Here's what the published human trials look like at a glance:
- NR at 100 to 1000 mg/day: No serious adverse events across the major safety trials. Mild events (flushing, nausea, headache) showed up but at rates similar to placebo.
- NMN at 250 to 900 mg/day: No serious adverse events in the published trials so far. Reported effects were generally mild and short-lived.
- Nicotinamide at gram-range doses: Better characterised because it has decades of use in dermatology and broader metabolic research, with a recognisable list of side effects at high doses.
- Niacin (nicotinic acid): Best known for the flushing reaction, which is mechanistically different from anything NR/NMN produce.
For VERO members researching the LEGACY protocol, the relevant comparison is between NR/NMN at the doses people actually use and the regulatory and biological flags that show up at higher exposures.
What side effects do people report on NAD supplements?
Across the human trials and the broader user-report literature, four patterns come up again and again. None are common at sensible doses. All are worth knowing.
The most frequently mentioned are:
- Flushing: warmth, redness, sometimes itching across the face and neck.
- Gastrointestinal upset: mild nausea, soft stools, or stomach discomfort.
- Headache: usually within the first few days, tapering off.
- Sleep disturbance: vivid dreams or shallow sleep when dosed later in the day.
In the Conze et al. NIAGEN trial, healthy overweight adults received NR at 100, 300, or 1000 mg per day for eight weeks, and the rate of reported adverse events was statistically indistinguishable from placebo (Conze et al., 2019). In the Martens et al. study, six weeks of 1000 mg/day NR in middle-aged and older adults was reported as well tolerated, with no serious adverse events (Martens et al., 2018). The Dollerup et al. trial in obese men, at 2000 mg/day NR for 12 weeks, also reported good overall tolerability (Dollerup et al., 2018).
On the NMN side, Yi et al. ran a multicentre, double-blind, placebo-controlled trial in healthy middle-aged adults at 300, 600, and 900 mg/day for 60 days. No serious adverse events were reported, and overall tolerability was described as good across all doses (Yi et al., 2023).
The Yoshino et al. trial in postmenopausal women with prediabetes used 250 mg/day NMN for ten weeks and reported it as well tolerated (Yoshino et al., 2021).
That's the formal picture. The informal one, in user reports and clinic conversations, is broadly compatible: most people feel nothing in particular, a minority notice something mild, and a much smaller group find a specific symptom (often sleep or flushing) that pushes them to lower the dose or move it to morning.
Why does NAD flushing happen and who gets it?
Flushing is the side effect most people associate with the NAD family, but the cause depends on which form you're taking.
Think of your skin as a thermostat with blood vessels as the dial. When certain signalling molecules wash through, the dial turns up. Blood rushes closer to the surface, you feel warm, your face goes red.
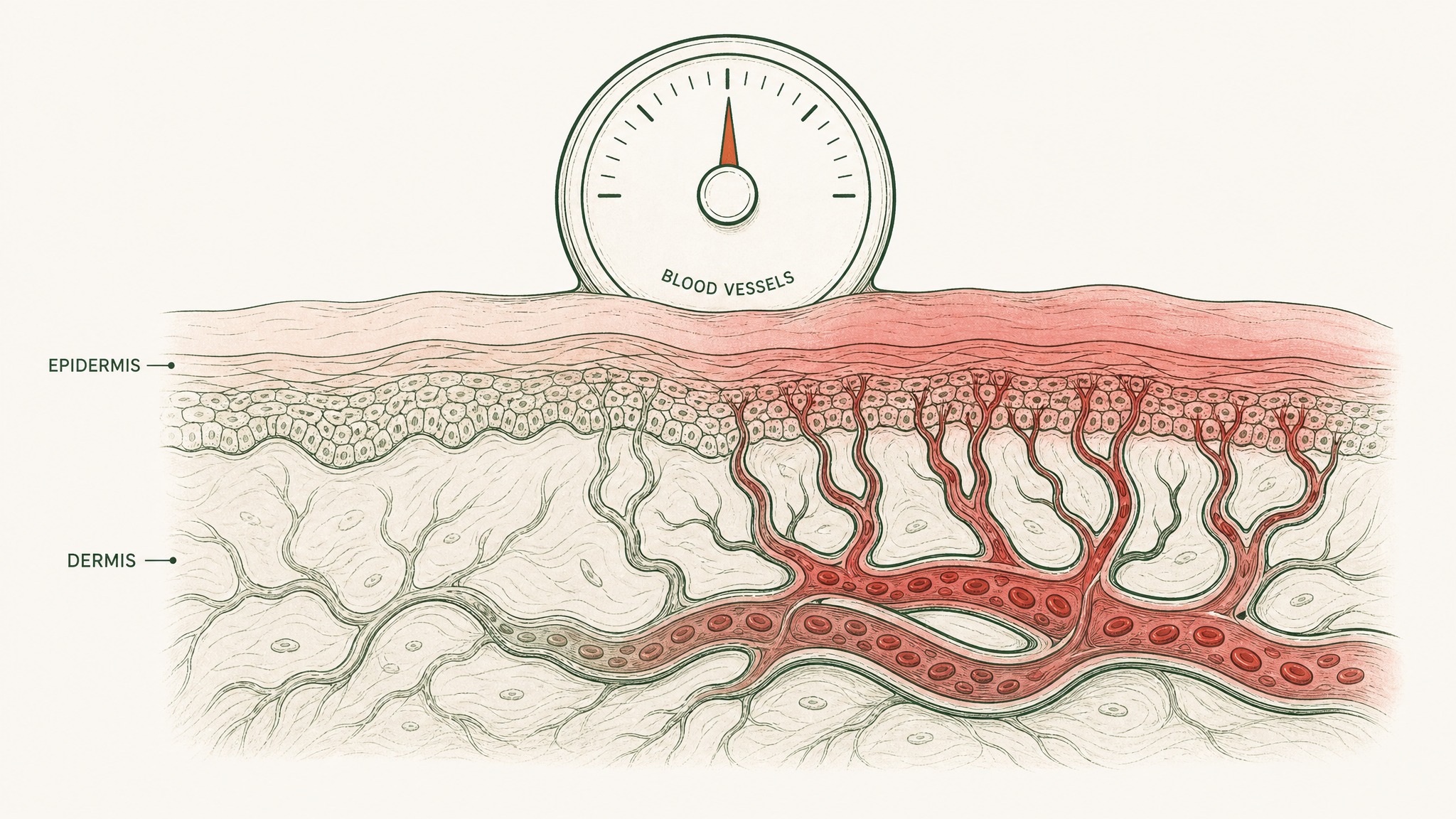
Blood vessels dilate near the skin surface, causing the face to flush red and warm.
That reaction is the defining feature of niacin (nicotinic acid). It's not really a "side effect" in the usual sense, it's the predictable result of niacin binding a receptor (GPR109A) on immune cells in the skin and triggering prostaglandin release (Benyó et al., 2005). At gram-range niacin doses, almost everyone gets it.
Here's the part most people miss:
- Niacin (nicotinic acid): Flushing is a feature, not a bug. Mechanism is well characterised.
- Nicotinamide (NAM): Doesn't bind GPR109A in the same way and doesn't typically cause flushing.
- NR and NMN: Aren't typical flush triggers either; flushing reports in NR/NMN trials are rare and not clearly above placebo.
If you're flushing on what's labelled an "NAD supplement", the first thing to check is whether the active ingredient is niacin (often dressed up as "vitamin B3" on the label). Several budget NAD blends use it because it's cheap.
What about long-term safety: does NAD feed cancer?
This is the question that comes up most often once people read beyond the marketing, and it deserves a careful answer rather than a confident one in either direction.
The biology is real. NAD+ is fuel for the maintenance crews inside your cells, including some that healthy cells and cancer cells both rely on. Preclinical work has looked at whether boosting NAD+ in animal models with established tumours could change tumour behaviour. The signals so far have been mixed: some preclinical models suggest higher NAD+ availability supports tumour metabolism, others suggest it supports immune surveillance against tumours (see review by Chini et al., 2017).
What we don't have is a long-term human cancer-incidence trial of NR or NMN. The longest published human safety follow-ups so far run roughly a year. That's the data limit, full stop. Research suggests this gap matters more for older adults with a higher baseline cancer risk than for healthy thirty-somethings, but the honest answer is we don't have the trial that would settle it.
In our protocol design, we approach this gap honestly. When members ask about NAD precursors during active oncology care or in a recent-cancer window, we point to the absence of long-term human data and the preclinical mixed signals, and recommend they speak with their oncologist before adding anything from the NAD family. This isn't a clinical claim, it's a "we don't have enough evidence to be casual" call.
For people without a cancer history, the human safety trials at typical doses look reassuring inside their study window. Just don't confuse "no serious AEs in a six-month trial" with "guaranteed safe for ten years". The honest position is: we don't know yet.
Why do NAD supplements sometimes cause sleep problems?
This one shows up in user reports more often than in trials, and it has a plausible mechanism even if it isn't formally documented at low doses.
NAD+ swings with your circadian rhythm. It rises during the active part of your day and falls during sleep, partly because sirtuins (the NAD-fuelled repair enzymes) interact with the same molecular clock that runs your sleep-wake cycle (Asher et al., 2008; Nakahata et al., 2009).

NAD+ peaks during the day and drops at night, so evening doses can interfere with sleep timing.
A short cheat sheet:
- Morning dosing: generally fine. Matches the natural rise of NAD+ on an active day.
- Late-afternoon dosing: usually fine for most people.
- Evening dosing: anecdotally the highest-report window for vivid dreams, lighter sleep, or trouble falling asleep.
- At-bedtime dosing: the most common pattern in user reports of disturbed sleep.
If sleep changes show up after starting an NAD precursor, the first move most people make is to shift the dose earlier in the day. In practice, that resolves it for the majority who report it. Members experience this most often when they're stacking NAD support with an evening protocol; moving the NAD dose to morning is usually enough to clean it up.
This isn't formally proven in trials. Sleep tracking isn't a standard endpoint in NAD precursor studies, so the published literature is quiet on it. But the mechanism is plausible enough that timing-first is the cheapest experiment.
How does methylation depletion fit into the picture?
This is the slow-burn concern that almost no NAD product page mentions, and it's the one your biochemistry teacher would care about most.
Picture methyl groups (small chemical tags) as a shared pool of currency your body uses for hundreds of jobs: DNA regulation, neurotransmitter balance, detox pathways, the works. When your body clears nicotinamide (the breakdown product of all NAD precursors), it does so by sticking a methyl group on it. That methylated nicotinamide gets peed out (Komatsu et al., 2018).
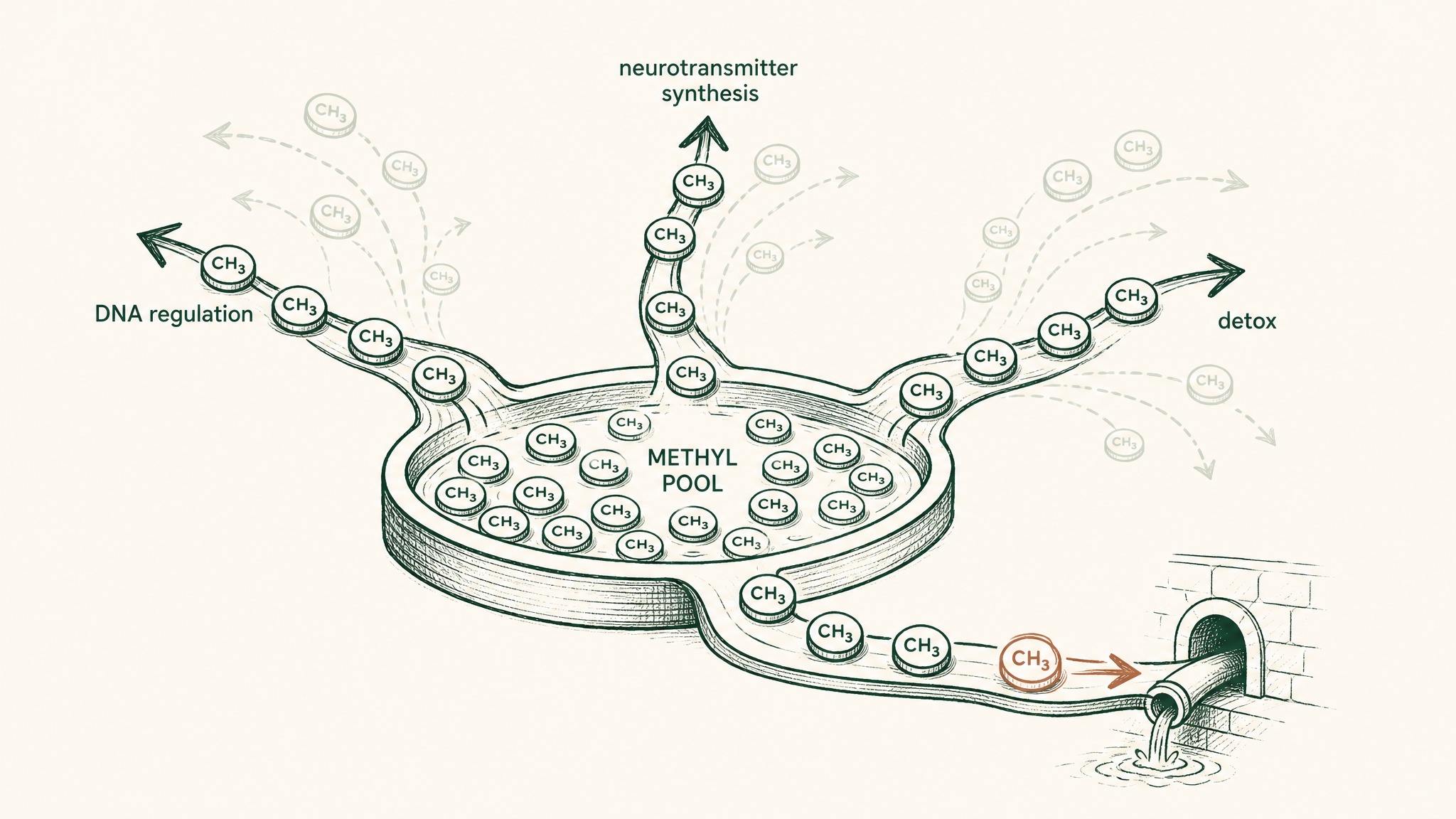
How NAD supplement metabolism drains the body's shared pool of methyl groups used for dozens of vital functions.
Take enough nicotinamide-yielding supplement, and you spend methyl currency. The concern raised by methylation researchers is that chronic high-dose NAD precursor intake might quietly draw down the methylation pool, with downstream effects on homocysteine, mood-related neurotransmitters, and other methyl-dependent systems.
What we know:
- Trials at moderate doses haven't reported obvious methylation problems on the timescales studied.
- Higher chronic doses are a known driver of urinary methylated metabolites, which is the marker of methyl spend.
- Some clinicians pair NAD precursors with methyl donors (methylated B vitamins, betaine) on a "cover the cost" logic, though the evidence that this is required is mostly theoretical.
The pragmatic read: at typical research doses of NR or NMN, this is more of a "good to know" than a "you must mitigate". At gram-range nicotinamide use (closer to the dermatology dosing range), it's worth real attention.
What's the FDA saying about NMN right now?
Regulatory side effects are still side effects, in a different sense, and NMN's status has changed twice in two years.
In late 2022, the US FDA concluded that NMN had been authorised for investigation as a new drug (under 21 U.S.C. 350b(a)(2)) before being marketed as a dietary supplement. That finding effectively pulled NMN out of the dietary supplement category in the US (FDA, 2022). Several brands restructured product lines or labels in response.
A short timeline:
- NMN sold widely as a supplement through 2021 and most of 2022.
- FDA letter and category change late 2022.
- Industry petitions and ongoing legal/regulatory discussion through 2024 to 2026.
- As of writing, NR remains in the supplement category in the US; NMN remains in regulatory limbo.
What this means for buyers: NMN you buy today may sit in a grey zone depending on the brand's interpretation of the rule and the route to market. It is not the same as "NMN has been found unsafe". Users report continuing to use NMN; researchers continue to study it. But the legal floor under it is genuinely different from NR, and a careful buyer reads labels and brand statements with that context.
This is one reason the VERO LEGACY protocol approaches NAD support through sublingual delivery and VERISORB-formulated direct NAD+, rather than building the entire protocol on a precursor whose regulatory status is moving.
Who should avoid NAD supplements?
A short, plain list of "outside the research base":
- Pregnancy and breastfeeding: no human safety data, opt out.
- Active cancer or recent cancer: preclinical mixed signals, talk to oncology.
- Children and adolescents: no human dosing or safety base, opt out.
- People on chemotherapy or immunotherapy: interactions are unstudied here. Coordinate with the prescribing team.
- People with significant kidney impairment: clearance pathways aren't fully characterised in this group.
- People on multiple methylation-relevant medications (some psychiatric medications, methotrexate, certain antiepileptics): flag with your prescriber.
This isn't a comprehensive contraindication list. It's the conservative-default version. The general principle is the same one that applies to every research-stage compound: if you sit outside the population the trials enrolled, the published safety data doesn't fully cover you.
How does delivery route change the side-effect picture?
Same molecule, different routes, different side-effect profiles. This is where the sublingual conversation comes in.
Oral capsule NAD precursors deliver a single bolus that hits the gut and liver first. Most of the dose gets processed before it ever reaches systemic circulation. That's why side-effect reports cluster around the gut (nausea, soft stools): the gut sees a lot of the dose.
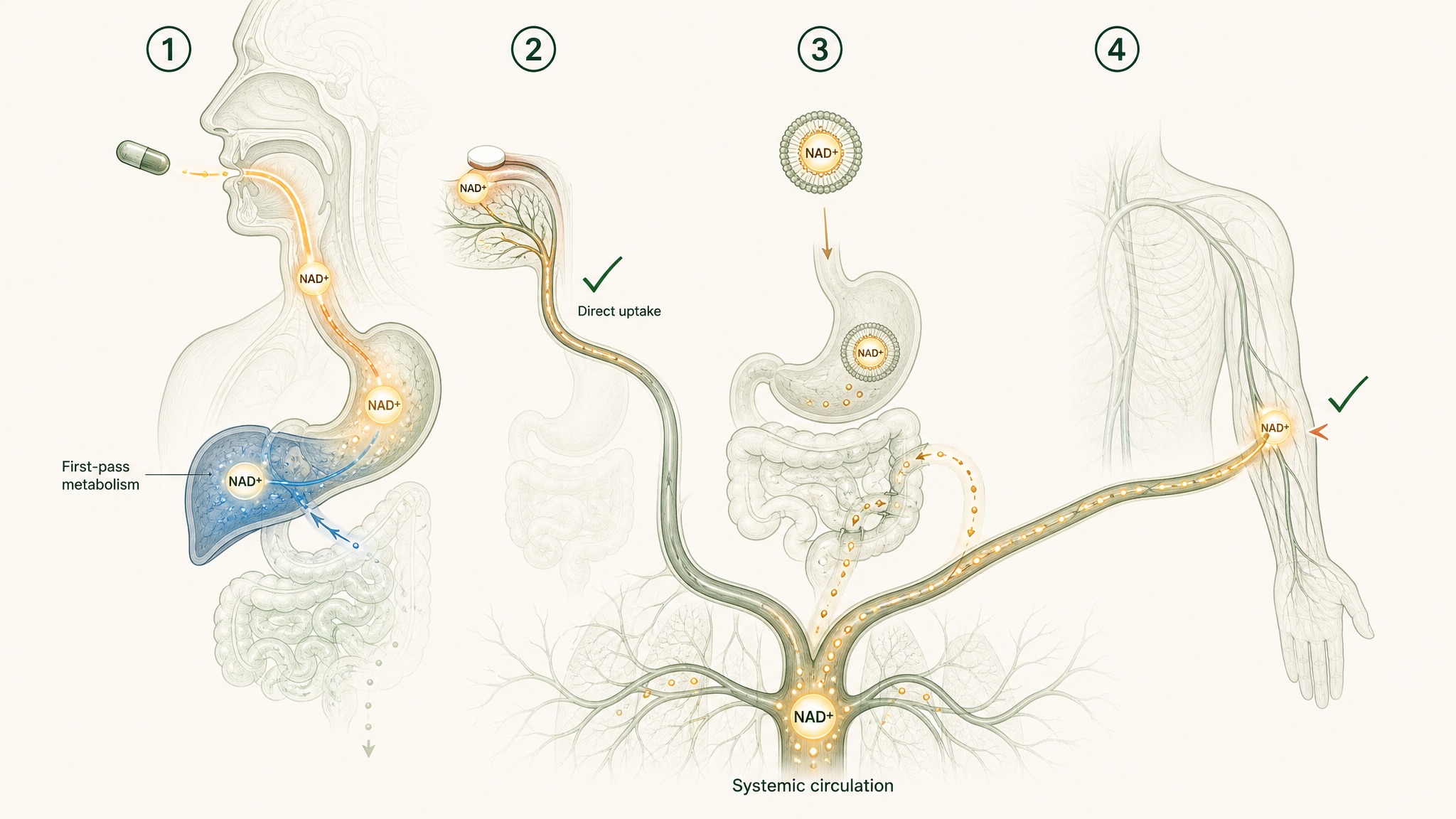
How four delivery routes send NAD+ through your body differently, from gut-first to bloodstream-direct.
A quick comparison:
- Oral capsule: Full first-pass through the gut and liver. GI side effects most common. Most of the dose is metabolised before reaching blood.
- Sublingual: Absorbed through tissues under the tongue, bypassing first-pass metabolism. Less gut exposure, more direct uptake into circulation.
- Liposomal: Designed to survive the gut, with mixed evidence on how much actually clears first-pass.
- IV NAD+: Rapid systemic delivery, occasionally associated with chest pressure and nausea during infusion. Done in clinic, not at home.
VERO uses VERISORB sublingual delivery for the LEGACY protocol partly for absorption reasons (covered in detail in our bioavailability guide and the VERISORB sublingual technology explainer), and partly because the gut-side side-effect picture changes when you skip the gut.
Key Takeaways
- At the doses tested in human trials, NR and NMN look well tolerated, with adverse-event rates similar to placebo.
- The most commonly reported side effects are flushing (mostly tied to niacin not NR/NMN), mild GI upset, headache, and sleep disturbance.
- Long-term human safety data beyond about a year doesn't exist yet for NR or NMN. Don't read "no AEs in a six-month trial" as a multi-year guarantee.
- Methylation strain is a real biochemical consideration at higher chronic doses, even if trials at typical doses haven't flagged it as an obvious problem.
- The FDA's 2022 decision pulled NMN out of the US dietary supplement category. NR remains in. Regulatory status is part of the side-effect picture in a wider sense.
- Pregnancy, breastfeeding, active cancer, paediatric use, chemotherapy, and severe kidney impairment sit outside the research base. Default to opting out.
- Delivery route affects which side effects show up. Oral capsules concentrate exposure in the gut. Sublingual and other routes shift the profile.
- Members researching the LEGACY protocol should read this article as background context, not protocol guidance. Speak to your clinician before adding anything new.
References
- Conze D, Brenner C, Kruger CL. Safety and metabolism of long-term administration of NIAGEN (nicotinamide riboside chloride) in a randomized, double-blind, placebo-controlled clinical trial of healthy overweight adults. Scientific Reports, 9, 9772 (2019). https://www.nature.com/articles/s41598-019-46120-z. Retrieved 2026-06-13.
- Martens CR, Denman BA, Mazzo MR, et al. Chronic nicotinamide riboside supplementation in healthy middle-aged and older adults: tolerability and NAD+ data. Nature Communications, 9, 1286 (2018). https://www.nature.com/articles/s41467-018-03421-7. Retrieved 2026-06-13.
- Dollerup OL, Christensen B, Svart M, et al. Randomized placebo-controlled clinical trial of nicotinamide riboside in obese men: safety and metabolic outcomes. American Journal of Clinical Nutrition, 108(2), 343–353 (2018). https://academic.oup.com/ajcn/article/108/2/343/5095055. Retrieved 2026-06-13.
- Yi X, Li J, Xu Y, et al. The efficacy and safety of β-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience (2023). https://pubmed.ncbi.nlm.nih.gov/36482258/. Retrieved 2026-06-13.
- Yoshino M, Yoshino J, Kayser BD, et al. Nicotinamide mononucleotide and muscle insulin sensitivity in prediabetic postmenopausal women: clinical-trial data. Science, 372(6547), 1224–1229 (2021). https://www.science.org/doi/10.1126/science.abe9985. Retrieved 2026-06-13.
- Benyó Z, Gille A, Kero J, et al. GPR109A receptor and nicotinic-acid–induced flushing: mechanistic evidence. Journal of Clinical Investigation, 115(12), 3634–3640 (2005). https://www.jci.org/articles/view/23626. Retrieved 2026-06-13.
- Asher G, Gatfield D, Stratmann M, et al. SIRT1 and circadian clock gene expression via PER2 deacetylation. Cell, 134(2), 317–328 (2008). https://www.cell.com/cell/fulltext/S0092-8674(08)00679-7. Retrieved 2026-06-13.
- Nakahata Y, Sahar S, Astarita G, et al. Circadian control of the NAD+ salvage pathway by CLOCK-SIRT1. Science, 324(5927), 654–657 (2009). https://www.science.org/doi/10.1126/science.1170803. Retrieved 2026-06-13.
- Komatsu M, Kanda T, Urai H, et al. NNMT activation and fatty liver disease: a role for NAD+ metabolism. Scientific Reports, 8, 8637 (2018). https://www.nature.com/articles/s41598-018-26882-8. Retrieved 2026-06-13.
- Chini CCS, Tarragó MG, Chini EN. NAD and the aging process: role in life, death and everything in between. Molecular and Cellular Endocrinology, 455, 62–74 (2017). https://www.sciencedirect.com/science/article/abs/pii/S0303720716305093. Retrieved 2026-06-13.
- US Food and Drug Administration. Response to NDI notification regarding NMN; statement on NMN dietary supplement status. FDA (2022). https://www.fda.gov/food/dietary-supplements. Retrieved 2026-06-13.
For research purposes only. Curious about how VERO formulates NAD+ for sublingual uptake? Explore the LEGACY protocol →
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.