
Peptides signal your skin to produce collagen and elastin, but type and delivery method determine whether they work. Here's what the research actually shows.
Skin care with peptides is one of the most-cited anti-aging categories in the industry, and also one of the most misunderstood. Peptides for skin appear on serum labels, moisturiser tubs, and eye-cream packaging, often with bold claims about firmness and collagen. What those labels rarely explain is which type of peptide you're actually getting, whether it can physically reach the part of your skin that matters, or what the evidence actually shows when you go looking for it.
This guide cuts through that. You'll come away knowing the five functional categories of skin-care peptides, which ones have meaningful clinical evidence, why most topical formulations hit a biological ceiling, and what that ceiling means for how you build a routine. This content is published for research purposes only.
What Peptides Do for Skin
Skin care with peptides works because peptides are biological messengers, short chains of amino acids (the building blocks your body uses to make every protein, including collagen) that bind to receptors on skin cells and trigger specific responses. In plain terms: your skin already runs on peptide signals. Collagen production declines roughly 1% per year from your mid-20s (Rittié & Fisher, Am J Clin Nutr 2002), and topical peptides are designed to compensate for the signals your body is producing less of.
The four-step mechanism, in plain English:
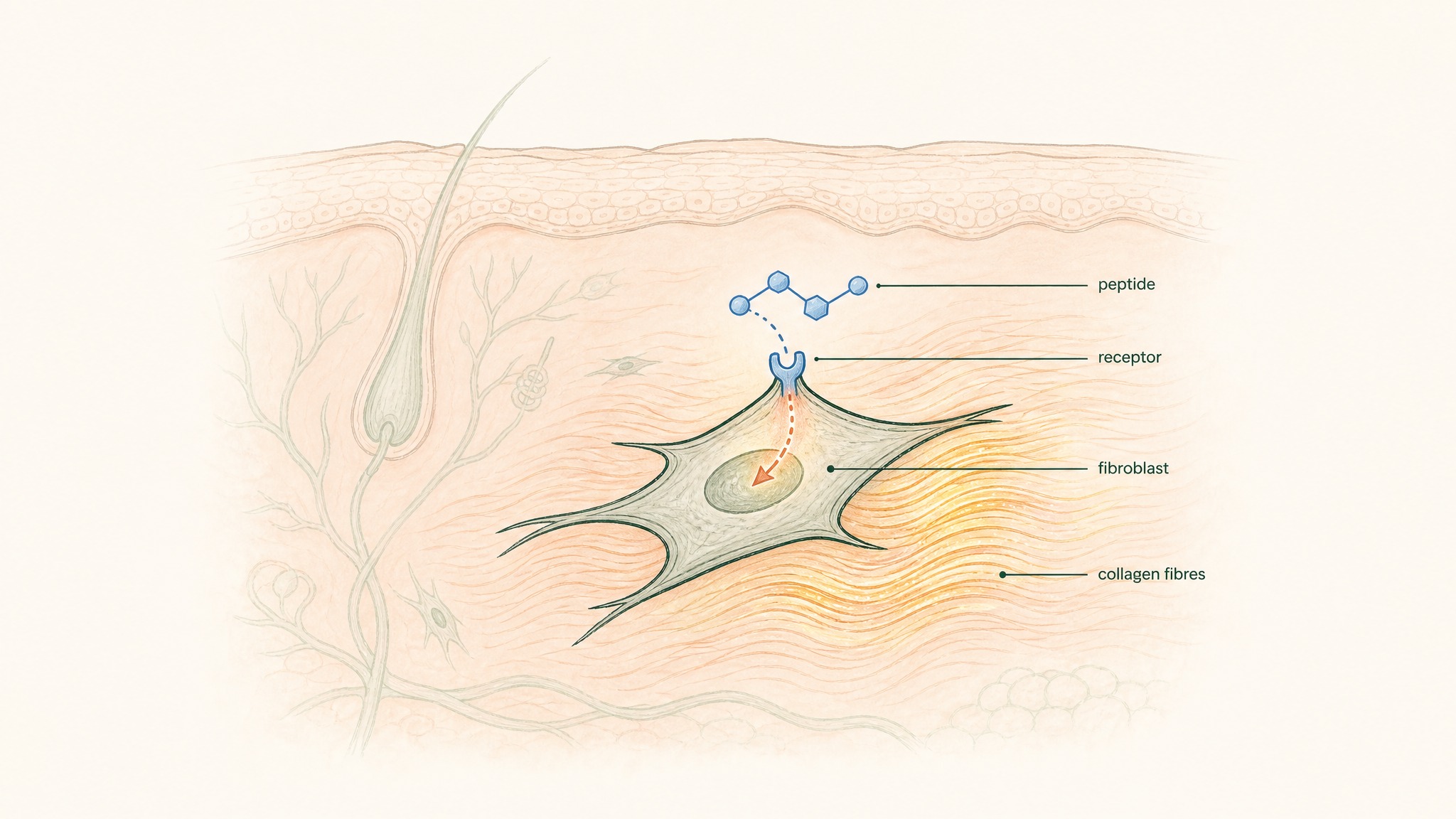
How a peptide binds a skin cell receptor and signals it to produce more collagen.
- Peptide binds receptor, the peptide molecule fits a receptor on a fibroblast (your skin's structural maintenance cell) like a key into a lock
- Gene expression is triggered, the binding event activates the relevant gene inside the cell, telling it to start producing a specific protein
- Fibroblast increases output, the cell begins manufacturing collagen, elastin, or hyaluronic acid at a higher rate
- Structural protein accumulates, with consistent signalling over weeks, new collagen fibres build up in the dermis (the deeper structural layer of your skin, below the surface you can see and touch)
What makes this mechanism worth taking seriously isn't the theory, it's that the decline it's compensating for is measurable. By the time you're 45, your dermis has visibly less collagen density than it did at 25. The biology isn't subtle.
After menopause, collagen loss accelerates to roughly 2% per year as estrogen levels fall (Thornton, Dermatoendocrinology 2013, PMC3772914). So across a single decade in your early post-menopausal years, you can lose 20% of remaining dermal collagen, the same amount that took 20 years to accumulate and lose in the previous stage.
Citation capsule: Collagen production in human skin declines approximately 1% per year from the mid-20s under normal aging conditions, with post-menopausal acceleration to roughly 2% per year tied to estrogen decline (Rittié & Fisher, Am J Clin Nutr 2002; Thornton, Dermatoendocrinology 2013, PMC3772914). Signal peptides target the fibroblast signalling pathways responsible for this production.
What Are the Five Types of Peptides in Skin Care?
The label "peptide" covers a wide range of molecules doing very different things. Knowing the five types means you can read an ingredient list and understand what a formula is actually trying to do, instead of trusting marketing language to tell you.
Signal Peptides
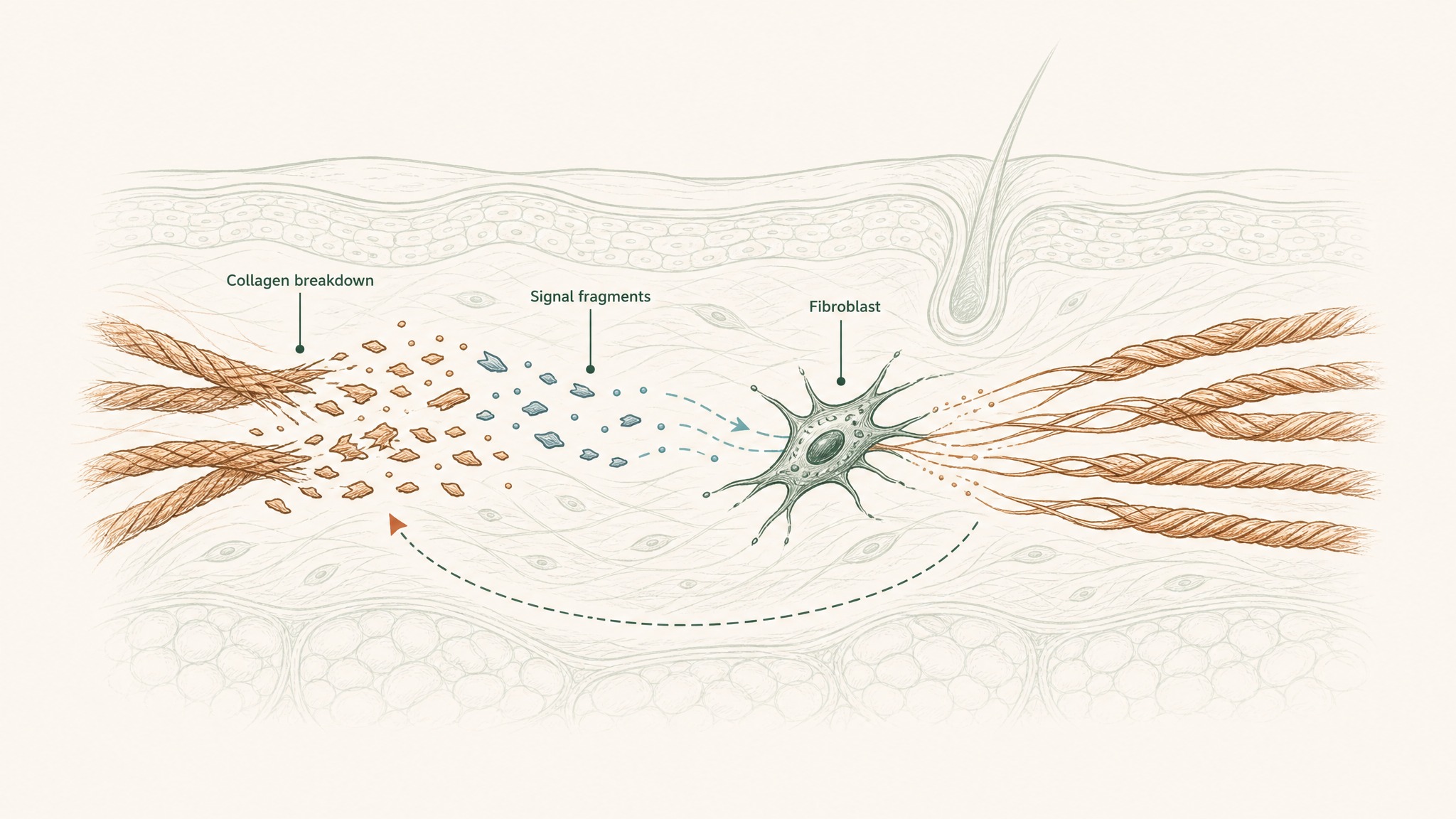
How collagen fragments from natural breakdown signal fibroblasts to make more collagen.
Your skin naturally loses collagen when it breaks down old fibres during routine cell turnover. The fragments released from that breakdown act as a feedback signal: your fibroblasts detect them and ramp production back up. Signal peptides for skin mimic those collagen-fragment signals, triggering the same fibroblast response without requiring actual breakdown to happen first.
The two most-researched signal peptides are Matrixyl (Palmitoyl Pentapeptide-4) and Matrixyl 3000 (Palmitoyl Tripeptide-1 + Palmitoyl Tetrapeptide-7). A key study by Robinson et al. (2005) found that topical Palmitoyl Pentapeptide-4 improved the appearance of photoaged facial skin versus a vehicle-only control in a split-face, randomised, double-blind design (Robinson et al., Int J Cosmet Sci 2005). They're the most commercially widespread peptide category for a reason: the signal-and-respond mechanism has a solid biological basis.
Carrier Peptides
Think of carrier peptides as delivery vehicles for trace minerals your skin needs to finish what signal peptides start. The primary example is GHK-Cu (copper tripeptide-1), a molecule your body naturally produces that carries copper ions to the dermis.
Here's why copper matters: once your fibroblasts have produced new collagen proteins, an enzyme called lysyl oxidase has to cross-link those fibres together, giving them the tensile strength to actually function as structural tissue. Lysyl oxidase is copper-dependent. Without adequate copper at the right location, new collagen fibres lack the cross-linking strength they need. GHK-Cu delivers the copper while also acting as a signal peptide in its own right, making it one of the most functionally versatile compounds in this entire category.
The full research profile on GHK-Cu is covered in the GHK-Cu copper peptide protocol guide, it's a long read, and worth it.
Neurotransmitter-Inhibiting Peptides
Expression lines, the ones driven by repeated muscle movement like squinting and frowning, form through a different mechanism than age-related skin thinning. Neurotransmitter-inhibiting peptides address this specifically.
Argireline (Acetyl Hexapeptide-3) is the most commercially common example. It interferes with the SNARE complex, a set of proteins that regulate muscle contraction signalling at the neuromuscular junction. Less contraction signal means less repetitive creasing of the skin. A 2002 study by Blanes-Mira et al. documented this mechanism in a synthetic hexapeptide and demonstrated wrinkle reduction versus a placebo control (Blanes-Mira et al., Int J Cosmet Sci 2002). SNAP-8 (Acetyl Octapeptide-3) works through a similar route. Worth noting: this class addresses muscle-driven lines specifically. It's not the right tool for lines formed from sun damage or general skin thinning.
Enzyme-Inhibitor Peptides
Your skin constantly remodels itself, building new collagen and breaking down old fibres at the same time. The enzymes responsible for breaking down collagen are called matrix metalloproteinases, or MMPs. They're a necessary part of healthy skin turnover, but their activity increases with age and UV exposure, gradually tipping the balance toward net collagen loss.
Enzyme-inhibitor peptides, including soy peptides and Leuphasyl, work by slowing MMP activity, shifting the net balance back toward more total collagen. They tend to play a supporting role in a well-formulated stack rather than carrying results on their own.
Antimicrobial Peptides (AMPs)
Antimicrobial peptides are the newest category in topical skin care and the one with the least cosmetic evidence. They're part of your skin's innate immune system, short peptides that support the microbiome (the community of bacteria, fungi, and other microorganisms that live on your skin surface) and help maintain barrier integrity.
Research suggests, the potential for AMPs in acne-associated microbiome imbalance and barrier-compromised skin is growing in clinical interest. But this is a category to watch rather than one that currently carries the evidence weight of the first four.
Which Peptides Have the Strongest Clinical Evidence?
Not every compound on an INCI (International Nomenclature of Cosmetic Ingredients, the standardised naming system for cosmetic ingredients) list has equal research behind it. The table below breaks down the five most clinically relevant peptides, their evidence tier, and the key studies.
Evidence tier definitions:
- Tier 1, multiple independent, replicated human studies including placebo-controlled designs
- Tier 2, human studies with supporting in-vitro data; some independent replication
- Tier 3, primarily in-vitro or manufacturer-funded only; limited independent human data
| Peptide | INCI Name | Primary Mechanism | Evidence Tier | Key Study |
|---|---|---|---|---|
| GHK-Cu | Copper Tripeptide-1 | Collagen synthesis + skin repair | Tier 1 | Pickart & Margolina, Int J Mol Sci, 2018 (>200 peer-reviewed studies; affects ~4,000 gene expressions) |
| Matrixyl (Palmitoyl Pentapeptide-4) | Palmitoyl Pentapeptide-4 | Stimulates collagen I and III synthesis | Tier 1 | Robinson et al., Int J Cosmet Sci, 2005 |
| Argireline | Acetyl Hexapeptide-3 | Reduces muscle contraction signal | Tier 2 | Blanes-Mira et al., Int J Cosmet Sci, 2002 |
| Palmitoyl Tripeptide-1 + 7 | Palmitoyl Tripeptide-1, Palmitoyl Tetrapeptide-7 | Collagen synthesis + anti-inflammatory | Tier 2 | Farwick et al. 2011; PMC11946782 (2025) |
| SNAP-8 | Acetyl Octapeptide-3 | Muscle contraction inhibition | Tier 3 | Limited clinical data; primarily in vitro |
GHK-Cu stands apart from everything else in the Tier 1 category. It's not just that more studies exist, it's that the scope of what those studies measured is qualitatively different. Research suggests GHK-Cu modulates expression by at least 50% in roughly a third of all human genes, affecting pathways far beyond skin collagen (Pickart & Margolina, Int J Mol Sci 2018, PMC6073405). The 2018 Pickart and Margolina analysis found GHK-Cu influences the expression of approximately 4,000 genes across tissue remodelling, antioxidant defence, and anti-inflammatory signalling, each active in the same protocol window.
Tier 3 doesn't mean useless, it means the clinical picture is incomplete. SNAP-8's mechanism is plausible and consistent with the same pathway as Argireline. But when you're buying a product, knowing that a compound's evidence base is manufacturer-funded in vitro data versus independently replicated human placebo-controlled trials is a distinction that matters.
The GHK-Cu copper peptide protocol guide covers the full human study data for GHK-Cu, including the placebo-controlled collagen biopsies and the genomic analysis.
Citation capsule: GHK-Cu (Copper Tripeptide-1) has more than 200 peer-reviewed studies indexed in the literature. A 2018 analysis by Pickart and Margolina found it modulates expression by at least 50% in roughly 31% of human genes, covering tissue remodelling, antioxidant defence, and skin collagen synthesis (Pickart & Margolina, Int J Mol Sci 2018, PMC6073405). No other cosmetic peptide has comparable breadth.
Why Most Topical Peptides Don't Reach the Dermis
Here's the gap the skincare industry almost never explains honestly. Skin care with peptides has a biological ceiling, and that ceiling is your skin's own barrier function.
Your outermost skin layer, the stratum corneum (think of it as a selective security checkpoint: it lets in some things and blocks most things), allows molecules under roughly 500 Daltons in molecular weight to pass through. Anything heavier is effectively blocked. This is the pharmaceutical 500 Dalton rule, a well-established principle in dermatology (Bos & Meinardi, Exp Dermatol 2000, PMID 10839713).
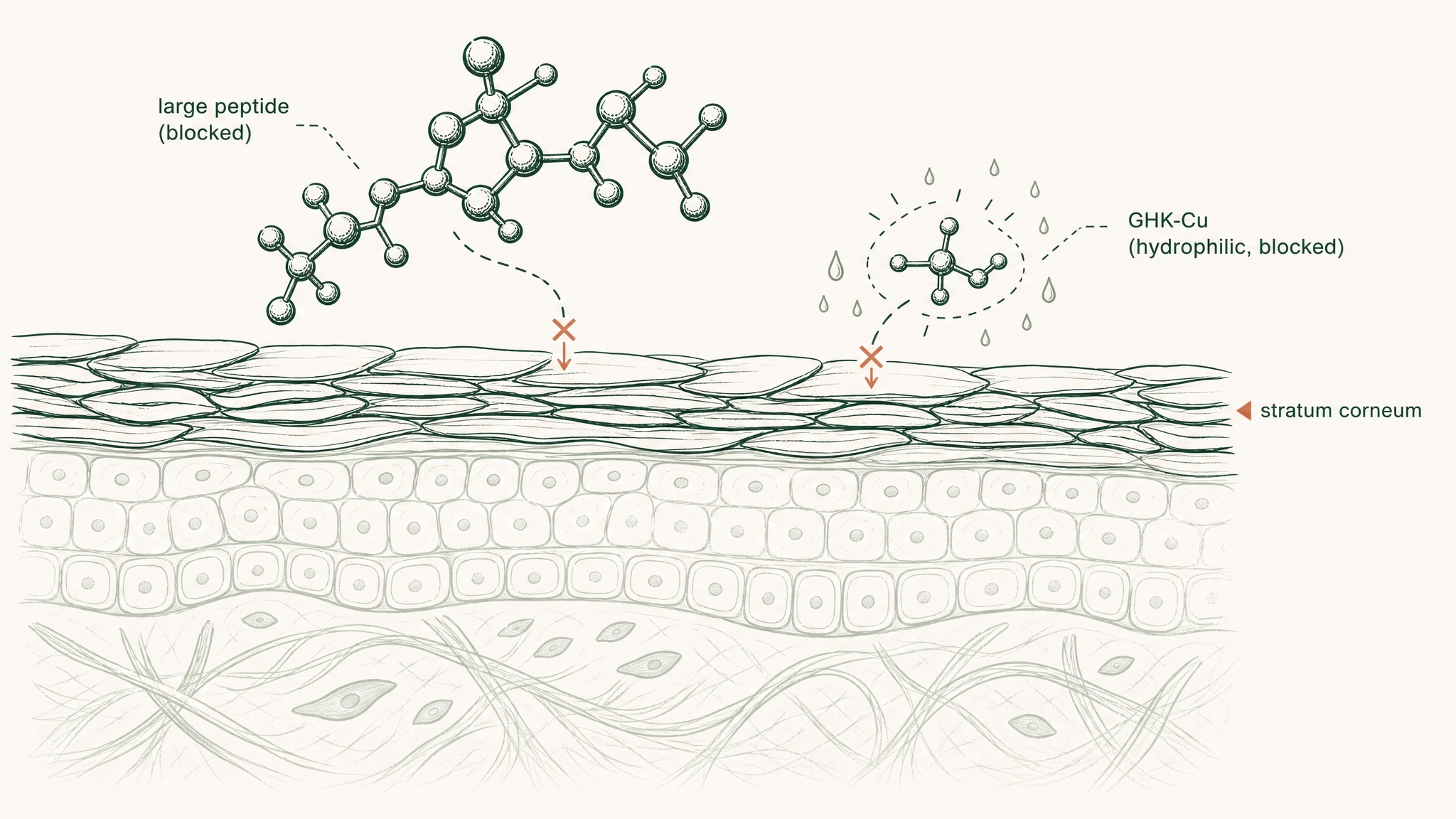
Why most peptides can't cross your skin barrier, even when they're small enough.
The 500 Dalton rule: Molecules under ~500 Daltons can theoretically pass through intact skin. Most therapeutic peptides exceed this threshold, or pass the size test but fail the polarity test (they're water-loving in a fat-based barrier). GHK-Cu weighs ~341 Daltons (within range) but is strongly hydrophilic, meaning it doesn't partition well into the lipid-rich stratum corneum regardless of its size.
Most therapeutic peptides exceed that 500 Dalton threshold. When they do, three things can happen:
- They sit on the skin surface, providing genuine hydration and barrier benefits, but not reaching dermal fibroblasts
- They require specialised delivery vehicles, liposomal encapsulation (spherical lipid carriers that protect the peptide and improve penetration through the lipid barrier) or nano-emulsification, to pass through
- They enter via a completely different route that bypasses the barrier entirely
Liposomal encapsulation does improve penetration, but it adds formulation instability and cost. A well-made liposomal peptide serum is genuinely better than a standard one. But even with the best topical engineering, you're navigating a barrier that evolved specifically to keep molecules out.
The other route is sublingual mucosal absorption, placing a peptide under the tongue, where specialised mucosal membranes absorb it directly into venous circulation. This bypasses the stratum corneum entirely. The peptide doesn't need to cross the skin barrier because it never goes near it, it enters the bloodstream and reaches the dermis from within.
VERISORB sublingual technology is VERO's formulation approach to this route. Rather than engineering around the skin barrier, it bypasses it by design, using mucoadhesive polymers to extend mucosal contact time and permeation enhancers to assist absorption through the membrane. Sublingual bioavailability data for GHK-Cu is covered here.
For a detailed comparison of topical, oral, sublingual, and injectable delivery routes, the oral vs. injectable peptide bioavailability analysis covers the evidence.
Citation capsule: The 500 Dalton rule establishes that molecules above approximately 500 Daltons cannot cross intact skin in clinically meaningful quantities (Bos & Meinardi, Exp Dermatol 2000, PMID 10839713). Most therapeutic peptides either exceed this threshold or face a secondary barrier: hydrophilicity limits their ability to partition into the lipid-rich stratum corneum even when molecular weight is within range.
Peptides for Specific Skin Concerns
Different concerns require different peptide types. Here's how to map your specific goal to the right compound, and what the evidence actually says for each.
Collagen Loss and Skin Laxity
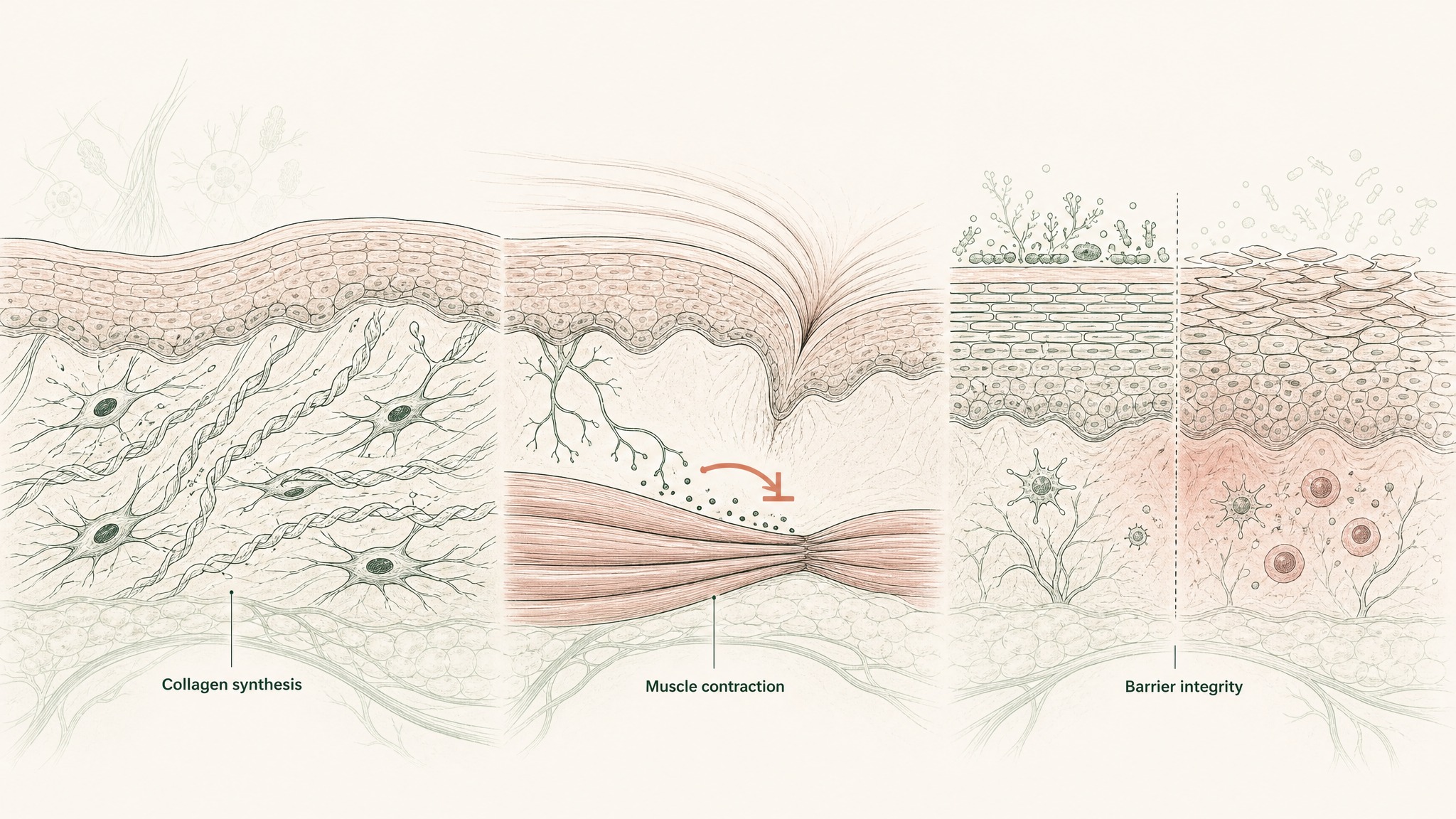
How different peptides target collagen loss, expression lines, and barrier damage through separate biological pathways.
This is the core application for signal peptides, and it's where the strongest human evidence lives. Palmitoyl Tripeptide-1 and Palmitoyl Pentapeptide-4 have both been studied for their ability to stimulate collagen I and collagen III synthesis in fibroblasts. A 2025 study indexed under PMC11946782 documented palmitoyl tripeptide's collagen-stimulating activity, contributing to an already-strong case for this compound class (PMC11946782).
If your primary concern is skin that's lost volume, firmness, or structural density, signal peptides for skin are the most evidence-backed starting point in the topical category.
Expression Lines and Dynamic Wrinkles
Expression lines, the ones that form from repeated muscle movement at the corners of your eyes, between your brows, around your mouth, are a different problem from structural collagen loss. Neurotransmitter-inhibiting peptides like Argireline and SNAP-8 address muscle-driven lines specifically.
The 2002 Blanes-Mira et al. study documented this mechanism with a synthetic hexapeptide in a placebo-controlled design, showing measurable wrinkle reduction (Blanes-Mira et al., Int J Cosmet Sci 2002). Worth knowing: these compounds are designed for expression lines. Sun-damage lines, general skin thinning, and loss of elasticity are a different mechanism requiring a different approach.
Skin Barrier and Hydration
Healthy barrier function, your skin's ability to hold moisture and resist environmental irritants, depends on the integrity of the stratum corneum and the microbiome that lives on it. GHK-Cu supports barrier function through multiple pathways: it increases production of barrier-supporting proteins, reduces inflammation that degrades barrier integrity, and its copper-delivery function supports enzymatic processes involved in skin structure maintenance.
Members experience barrier improvement as one of the earlier signals in a GHK-Cu protocol, typically within the first two to three weeks, because surface barrier response precedes the deeper collagen-synthesis changes that take longer to accumulate.
Hyperpigmentation
GHK-Cu has a distinct and often-overlooked role in pigmentation. Research suggests it modulates melanin synthesis, the process by which melanocytes (pigment-producing cells) generate the brown pigment responsible for uneven skin tone, through a mechanism distinct from vitamin C's tyrosinase inhibition pathway (Pickart & Margolina, Int J Mol Sci 2018, PMC6073405).
This is useful practically: combining GHK-Cu with a stable vitamin C derivative targets hyperpigmentation from two independent angles, which is more effective than either alone.
Menopausal and Hormonally Thinning Skin
Estrogen plays a direct role in skin collagen production. As estrogen declines after menopause, collagen loss accelerates to roughly 2% per year, meaning the first decade post-menopause can account for as much as 30% of total lifetime skin collagen loss (Thornton, Dermatoendocrinology 2013, PMC3772914). That's a steep structural change in a short window.
Signal peptides and GHK-Cu are among the most-studied compounds in the context of post-menopausal collagen support. This is research context only, the goal is to understand the biology and what the evidence base was built around.
Sensitive and Acne-Prone Skin
Peptides are one of the few evidence-supported actives with a consistently low irritation profile. They don't thin the skin barrier the way retinoids can, and they don't cause the sensitivity rebound that some exfoliants produce. Antimicrobial peptides may offer additional benefit for acne-associated microbiome imbalance, a growing area of clinical interest, though the evidence base for this specific application is still developing.
If you've found most actives too reactive, peptides are a rational starting point: effective without the disruption.
Peptides vs. Retinol, A Direct Comparison
The two most-discussed anti-aging actives in skin care are peptides and retinol. They're not competitors, but understanding their differences tells you exactly how to combine them.
| Metric | Peptides | Retinol |
|---|---|---|
| Collagen mechanism | Stimulate collagen synthesis via fibroblast signalling | Accelerate skin cell turnover, which indirectly increases collagen production |
| Irritation risk | Low | Moderate to high, especially when first starting |
| Suitable for sensitive skin | Yes | With a slow acclimation protocol |
| Safe during pregnancy | Generally yes | No, vitamin A is contraindicated during pregnancy |
| Timeline to visible results | 8-12 weeks | 4-8 weeks (epidermal changes visible sooner) |
| Works with other actives | Broad compatibility | Avoid strong acids; don't combine with vitamin A prescriptions |
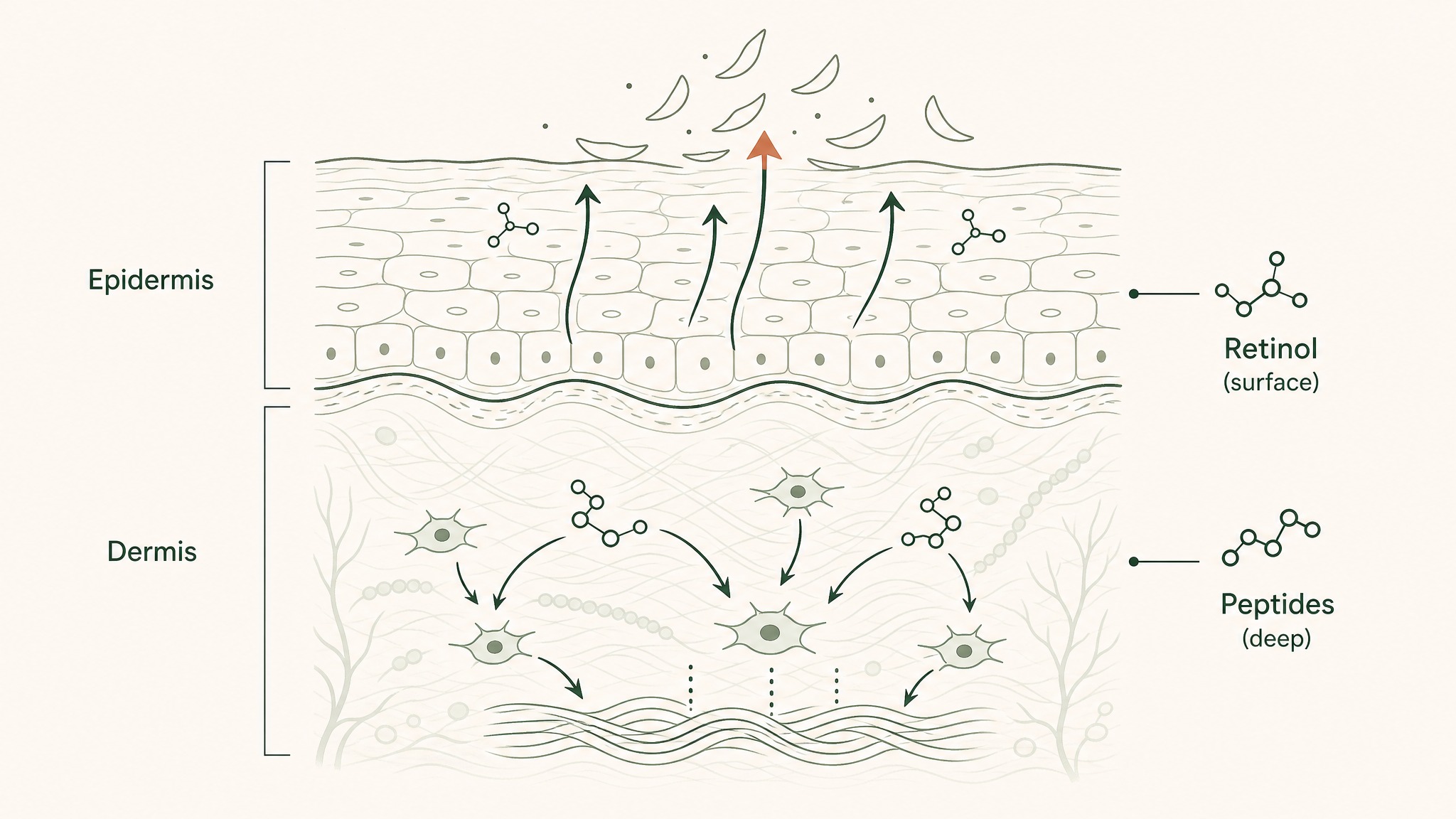
Retinol speeds cell turnover at the skin surface; peptides signal collagen-building deeper in the dermis.
Retinol's faster timeline to visible results reflects epidermal-level changes, surface skin cell turnover speeds up quickly. Peptides work deeper and slower, building structural dermal change that takes longer to become visible but affects the dermis rather than just the surface.
The practical takeaway: use them together. They target different mechanisms at different depths. Retinol does its work at the epidermal level; peptides signal fibroblasts in the dermis. Alternating nights is a good approach for those still acclimating to retinol, peptide serum on retinol-off nights, retinol plus a peptide moisturiser on retinol nights.
One compatibility note worth keeping: don't apply peptides directly after a low-pH AHA or BHA (exfoliating acid) treatment. Peptides can degrade below pH 4. If you use a glycolic or lactic acid product, apply it and allow it to fully absorb before switching to your peptide serum, or use them at different times of day.
How to Build a Peptide-Forward Skin Care Routine
A skin care routine with peptides doesn't need to be complicated. The key principle: peptides work best when applied to a clean, slightly damp face, allowed to absorb before other actives are layered on top.
| Step | AM Routine | PM Routine |
|---|---|---|
| Cleanse | Gentle, non-stripping cleanser | Gentle cleanser (double-cleanse if wearing SPF or makeup) |
| Tone / essence | Hydrating essence or peptide-forward toner | Same, or skip in favour of next step |
| Serum | Peptide serum, primary application step | Peptide serum OR peptide + retinol layering (see note below) |
| Moisturiser | Ceramide-based moisturiser | Richer barrier-support formula |
| SPF | Broad-spectrum SPF 30+ | Not needed |
Ingredient compatibility at a glance:
- Pairs well with: hyaluronic acid, niacinamide, ceramides, SPF, stable vitamin C derivatives (ascorbyl glucoside, sodium ascorbyl phosphate)
- Use with caution: L-ascorbic acid vitamin C at low pH, can degrade certain peptides; use a stable derivative instead, or apply at different times of day
- Avoid in the same step: strong AHAs/BHAs (glycolic, lactic, salicylic), wait until pH normalises before applying peptides
A note on consistency: most peptide research measures outcomes at 8-12 weeks of daily application. This isn't a slow product, it's a system that requires consistent signalling over time. Single-use results are not expected and not the point. Think of it the same way you'd think about strength training: one session doesn't build muscle, but six consistent weeks of training does.
Skin care with peptides is the same principle. The signalling needs time to translate into structural protein accumulation.
In reviewing member progress tracking across a 12-week RADIANCE research preview, the clearest pattern is that texture and hydration improve in weeks one to three, while firmness and fine-line changes become documentable in weeks eight to twelve.
What to Look for When Choosing Skin Care with Peptides
The best peptides for skin care don't help you if the product is formulated poorly or the concentration is too low to do anything. Here's a practical five-point checklist before you buy.
Named peptide in the first five INCI ingredients. INCI ingredients are listed in descending order of concentration. If the peptide sits near the bottom, it's present at a cosmetic trace level, likely included for label appeal rather than biological effect. Look for Palmitoyl Pentapeptide-4, Copper Tripeptide-1, Acetyl Hexapeptide-3, or Palmitoyl Tripeptide-1 in the top half of the list.
Stable delivery vehicle. Look for liposomal, nano-encapsulated, or oil-in-water emulsion formats. These aren't marketing buzzwords, they're the engineering difference between a peptide that reaches the dermis and one that sits on the surface. A serum with GHK-Cu in an unformulated water base is doing less than a well-engineered liposomal version of the same concentration.
Appropriate pH range. Peptide formulations should sit between pH 4 and pH 7. Below pH 4, peptide stability drops significantly. If a brand doesn't disclose pH, a buffered serum format (the pH is stabilised by the formulation base) is a better signal than a free-acid-containing serum.
No destabilising co-actives in the same formula. A single product that combines L-ascorbic acid at a low working pH with peptides is likely degrading one or both actives in the bottle. Separate them into different products or rely on stable vitamin C derivatives in peptide-containing formulas.
Transparency on sourcing and batch testing. Peptide purity matters. A provider that publishes certificates of analysis (COAs, independent lab tests confirming ingredient identity and concentration) is giving you something meaningful. One that doesn't is asking you to trust the label.
Most comparison guides focus on which peptide to choose. The more consequential variable is formulation quality. Two serums containing identical peptides at identical concentrations can produce meaningfully different outcomes if one uses an engineered delivery vehicle and the other uses a plain aqueous base.
Frequently Asked Questions
What age should you start using skin care with peptides?
Collagen synthesis begins declining from the mid-20s, roughly 1% per year from around age 25 (Rittié & Fisher, Am J Clin Nutr 2002). There's no minimum age for peptide skin care, but the strongest case for consistent use starts at 25-30, when natural production begins its slow reduction. Earlier use isn't harmful. The evidence base in most peptide studies was built on adult populations, typically 30 and older, so earlier application is extrapolated rather than directly evidenced.
Can you use peptides with retinol?
Yes, and it's a good combination. They target different mechanisms at different skin depths. Apply retinol on cleansed skin, wait until it's fully absorbed, then layer a peptide moisturiser or serum on top. Alternating nights works well if you're still acclimating to retinol. The one thing to avoid: applying both immediately after a low-pH acid exfoliant in the same step, which can degrade both actives.
How long does it take to see results from peptide skin care?
Research studies measure outcomes at 8-12 weeks of consistent daily application. Users report surface hydration and texture changes sooner, sometimes within two to three weeks, because those reflect epidermal and barrier-level responses. Structural changes like improved firmness and reduced fine lines require the full collagen synthesis cycle to accumulate. Expecting visible structural results in a week isn't realistic, and neither is abandoning a protocol after three weeks.
Are peptides safe for sensitive or acne-prone skin?
Peptides are among the best-tolerated active ingredients in skin care. They don't cause the barrier disruption associated with retinoids, and they don't trigger the sensitivity rebound that strong exfoliants can produce. For acne-prone skin specifically, antimicrobial peptides may offer additional benefit by supporting the microbiome balance associated with clearer skin, though this application has less clinical evidence than signal and carrier peptides. If you've reacted to most actives, peptides are a genuinely good starting point.
What's the difference between peptide skin care and peptide therapy?
Topical peptide skin care applies peptides to the skin surface, where penetration depends on molecular size, polarity, and formulation quality. Results are primarily surface-to-mid-dermal. Peptide therapy refers to systemic administration, injectables or sublingual protocols, where peptides enter the bloodstream and act across multiple tissue types, including the dermis from within. Research on systemic delivery is conducted for research purposes only, and results from systemic protocols reflect the biology of a different delivery route entirely.
Do oral or sublingual collagen peptides improve skin?
Multiple randomised controlled trials show that hydrolysed collagen peptides (collagen broken down into short, absorbable fragments) taken orally increase skin hydration and elasticity after eight or more weeks of consistent use. Sublingual delivery is a distinct route from swallowing. Sublingual absorption occurs through mucosal membranes under the tongue, bypassing first-pass liver metabolism (the liver's initial filtering pass, the process that breaks down a large fraction of swallowed compounds before they reach general circulation). This maintains higher peptide concentrations in circulation. Members experience this distinction most clearly in early protocol weeks, where systemic peptide effects are more apparent than with equivalent oral-only approaches. See the oral vs. injectable peptide bioavailability analysis for the research detail. Research is ongoing.
Key Takeaways
- Collagen declines roughly 1% per year from your mid-20s and accelerates to ~2% per year after menopause. Peptides address the signalling side of this decline, not the structural side directly.
- Five functional categories exist: signal peptides (stimulate collagen production), carrier peptides (deliver copper for collagen cross-linking), neurotransmitter-inhibiting peptides (soften expression lines), enzyme-inhibitor peptides (slow collagen breakdown), and antimicrobial peptides (support barrier and microbiome).
- GHK-Cu has over 200 peer-reviewed studies and influences expression of approximately 4,000 genes, making it qualitatively different from other cosmetic peptides in scope (Pickart & Margolina 2018, PMC6073405).
- Most topical peptides hit a biological ceiling set by the stratum corneum and the 500 Dalton rule. Topical delivery is most reliable for surface and barrier effects; structural dermal change requires engineered delivery or a different route.
- Peptides and retinol are complementary, not competitive. They work at different depths and through different mechanisms.
- Look for the named peptide in the first five INCI ingredients, a stable delivery vehicle, and pH 4-7 formulation. Formulation quality matters as much as which peptide is listed.
- Consistent daily application over 8-12 weeks is required to see structural results. Surface improvements come earlier; dermis-level changes take longer.
- Sublingual delivery bypasses the skin barrier entirely by entering the bloodstream via mucosal absorption, a meaningfully different approach to the same biology.
The Bottom Line
Skin care with peptides is built on real biology. The evidence for collagen signalling, fibroblast activation, and structural dermal support is not marketing language, it's reproducible science with five decades of published research behind the leading compounds. But type matters, and delivery mechanism matters more than most brands are willing to explain.
Research suggests the distinction between surface application and systemic delivery is one the industry is only beginning to address publicly. A well-formulated topical serum is a rational tool for surface and barrier outcomes. For structural dermal change, the fibroblast signalling, collagen synthesis, and ECM remodelling outcomes documented in controlled studies, the compound needs to reach the dermis from a route that actually gets it there.
That's the research question VERO is working on. VERISORB sublingual technology is the delivery system we're building around, designed to bypass the barrier rather than negotiate with it. The RADIANCE Protocol is in development, incorporating GHK-Cu, hyaluronic acid, and vitamin C via sublingual delivery, specifically to target the structural skin outcomes the published research was actually measuring. It's not available yet, but you can follow the research as it develops.
The evidence is real. The ceiling on topical delivery is real. And the work of closing the gap between them is what makes this a worthwhile area to follow.
References
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6073405/. Retrieved 2026-05-18.
- Robinson LR, et al. Topical palmitoyl pentapeptide provides improvement in photoaged human facial skin. Int J Cosmet Sci. 2005;27(3):155-160. https://pubmed.ncbi.nlm.nih.gov/18492208/. Retrieved 2026-05-18.
- Blanes-Mira C, et al. A synthetic hexapeptide (Argireline) with antiwrinkle activity. Int J Cosmet Sci. 2002;24(5):303-310. https://pubmed.ncbi.nlm.nih.gov/18494613/. Retrieved 2026-05-18.
- Papadopoulou A, et al. Current Approaches in Cosmeceuticals: Peptides, Biotics and Marine Biopolymers. Polymers (Basel). 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11946782/. Retrieved 2026-05-18.
- Rittié L, Fisher GJ. UV-light-induced signal cascades and skin aging. Ageing Res Rev. 2002;1(4):705-720. https://pubmed.ncbi.nlm.nih.gov/12499343/. Retrieved 2026-05-18.
- Thornton MJ. Estrogens and aging skin. Dermatoendocrinology. 2013;5(2):264-270. https://pmc.ncbi.nlm.nih.gov/articles/PMC3772914/. Retrieved 2026-05-18.
- Bos JD, Meinardi MMHM. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp Dermatol. 2000;9(3):165-169. https://pubmed.ncbi.nlm.nih.gov/10839713/. Retrieved 2026-05-18.
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration. Biomed Res Int. 2015;2015:648108. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/. Retrieved 2026-05-18.
- Papakonstantinou E, Roth M, Karakiulakis G. Hyaluronic acid: a key molecule in skin aging. Dermatoendocrinology. 2012;4(3):253-258. https://pmc.ncbi.nlm.nih.gov/articles/PMC3583886/. Retrieved 2026-05-18.
- Asserin J, et al. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network. J Cosmet Dermatol. 2015;14(4):291-301. https://pubmed.ncbi.nlm.nih.gov/26362110/. Retrieved 2026-05-18.
This content is published for research and educational purposes only. It is not intended to diagnose, treat, cure, or prevent any disease, and it does not constitute medical advice. Readers should consult a qualified healthcare professional before making any decisions about their own health. Statements on this page have not been evaluated by the FDA. VERO's peptide products are supplied for research purposes only.
RADIANCE™
Coming SoonEngineered around 5mg GHK-Cu. Increases dermal thickness and systemic collagen synthesis
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.