
How peptides fit into skin care, which compounds have real research, why topical serums hit a biological ceiling, and what actually changes your dermis.
Peptides are on roughly a third of skin care products sold today. The marketing around them, "collagen-boosting," "firming," "regenerating", sounds compelling. Cutting through it comes down to matching the right protocol to what the biology can actually deliver. But the category is genuinely complex, and understanding which compounds do what (and where the biology stops cooperating) makes the difference between a skin care routine that works and one that just costs a lot.
This guide covers the full ecosystem: what skin aging is, how peptides address it, which ones have the strongest evidence, and when you need a different approach entirely. This content is produced for research purposes only.
Key Takeaways
- Skin aging is driven by three converging changes: slowing fibroblast signalling, declining collagen and elastin production, and hyaluronic acid depletion from the dermis. Peptides address the signalling side of this.
- Signal peptides trigger production, carrier peptides deliver the minerals synthesis requires, and enzyme inhibitors slow collagen breakdown. Stacking more than one type targets different stages of the same cycle.
- GHK-Cu has the deepest research base in the category: five decades of published evidence, documented plasma decline with age, and collagen outcomes outperforming vitamin C cream and retinoic acid in placebo-controlled testing (PMID 4349963; PMC4508379).
- The stratum corneum's lipid barrier limits topical delivery regardless of peptide concentration. Molecular size (the 500 Dalton rule) is necessary but not sufficient, a peptide's hydrophilicity determines whether it crosses a fat-based barrier (PMID 10839713).
- Don't layer peptide serums directly with L-ascorbic acid vitamin C. Use a stable vitamin C derivative alongside peptides, or separate them to different times of day.
- Topical peptide products are genuinely useful for surface and barrier outcomes. For structural dermal change, fibroblast signalling and collagen synthesis, a systemic route bypasses the barrier the published research didn't have to navigate.
- Structural results accumulate over 8–12 weeks. The off-period reveals whether changes were structural (they last) or surface-level (they fade within weeks), that distinction guides what a second cycle should target.
Ready to build a skin protocol that reaches the dermis? Explore RADIANCE →
This content is published for research and educational purposes only. It is not intended to diagnose, treat, cure, or prevent any disease, and it does not constitute medical advice. Consult a qualified healthcare professional before making any decisions about your own health. Statements on this page have not been evaluated by the FDA. VERO's peptide products are supplied for research purposes only.
What Happens to Your Skin as It Ages
Think of your skin as a three-layer system. The surface you can see and touch, the epidermis, handles barrier function and surface appearance. Below it, the dermis is where the structural work happens: collagen fibres packed densely together, elastin woven between them, and fibroblasts (your skin's maintenance crew) spread throughout building and repairing the whole scaffold.
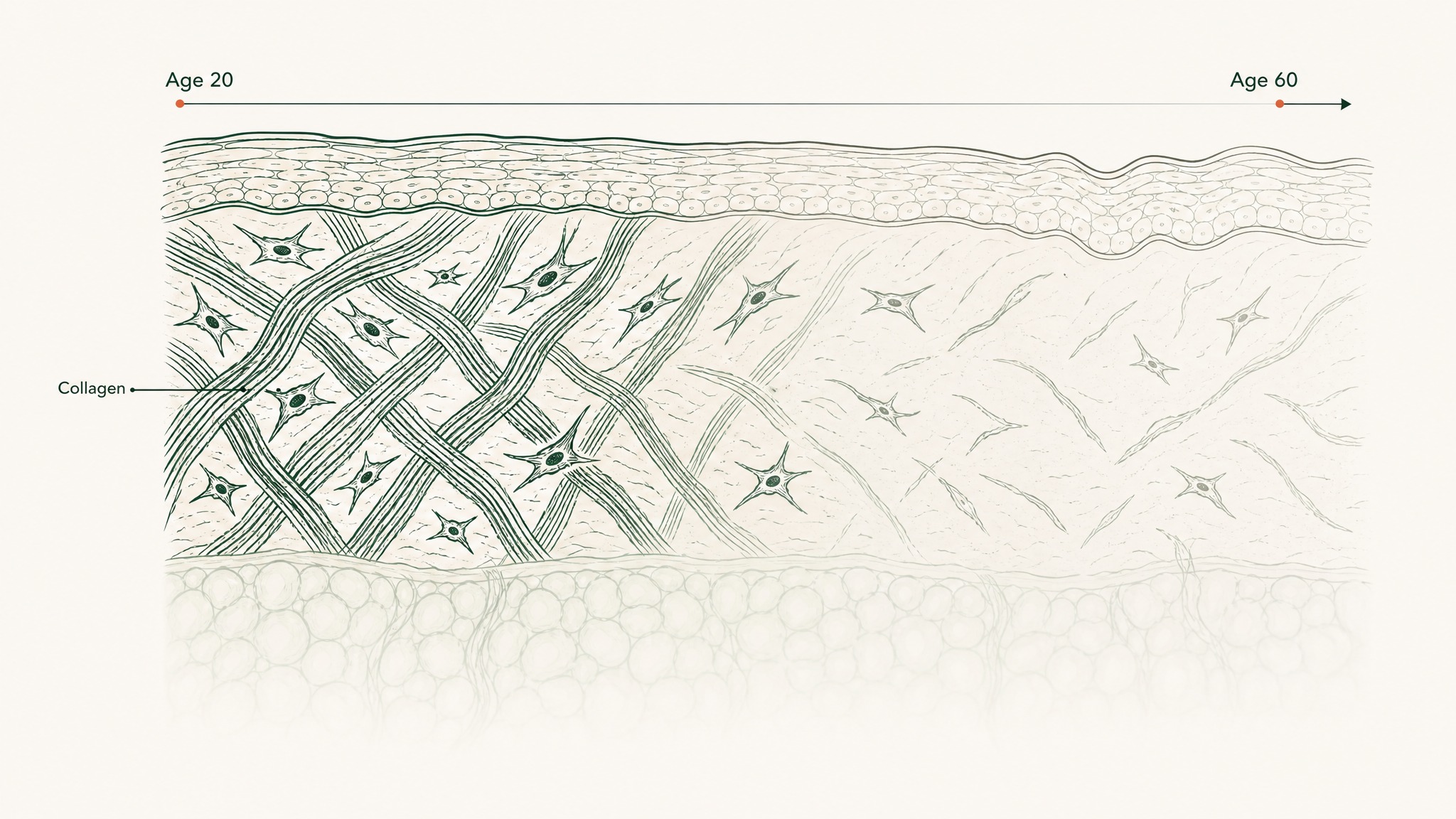
Here's where aging enters: by your thirties, your body produces roughly 1% less collagen per year. By your mid-forties, the fibres you still have are cross-linking poorly and breaking down faster than they're being replaced. The visible effects, skin that looks thinner, less resilient, slower to recover, track that biology directly.
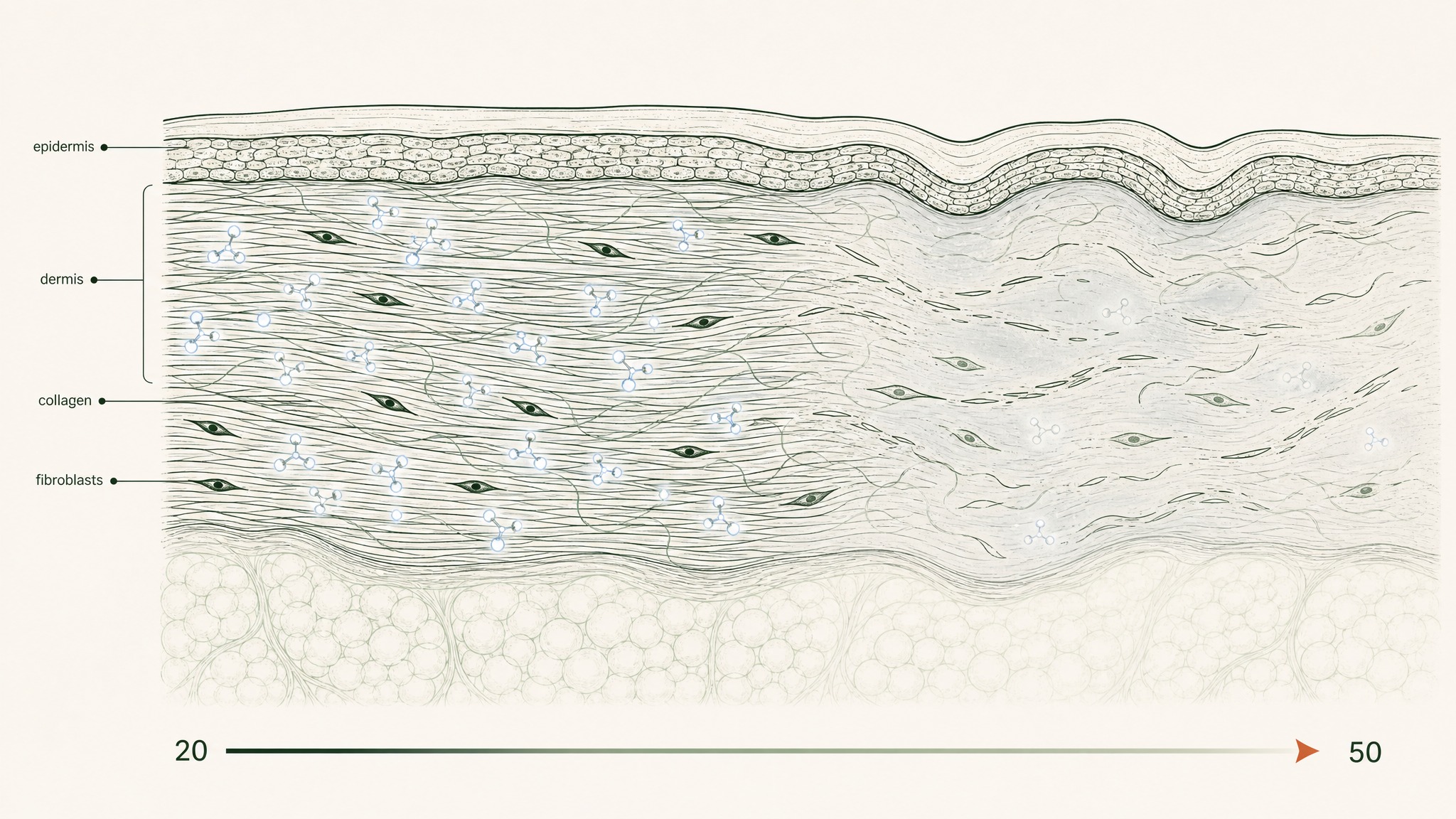
How collagen thins and fibroblasts slow down as skin ages from your twenties to your fifties.
Two other changes compound the problem:
- Hyaluronic acid depletes, this molecule fills the space between collagen and elastin fibres, binding water at up to a thousand times its own weight. Research suggests dermis HA levels drop measurably with age, reducing the volumetric cushion that gives younger skin its plumpness (Papakonstantinou et al., Dermatoendocrinology 2012, PMC3583886)
- Fibroblast signalling slows, the cells are still there, but they receive fewer production cues. They produce less and respond more sluggishly to repair signals
Peptides address the signalling side of this equation. They don't rebuild your dermis directly, they tell your fibroblasts to do it.
How Peptides Work: The Short Version
Peptides are short chains of amino acids, the same building blocks that make up collagen itself. When your body breaks down old collagen during normal tissue turnover, the fragments released act as signals: your fibroblasts detect them and ramp up new production. That feedback loop is how your skin naturally maintains itself.
What researchers worked out is that you can trigger those same fibroblast receptors artificially. Synthetic peptides mimic the signal without requiring the breakdown to occur first, which matters as you age, because your natural feedback system runs slower and the production response weakens.
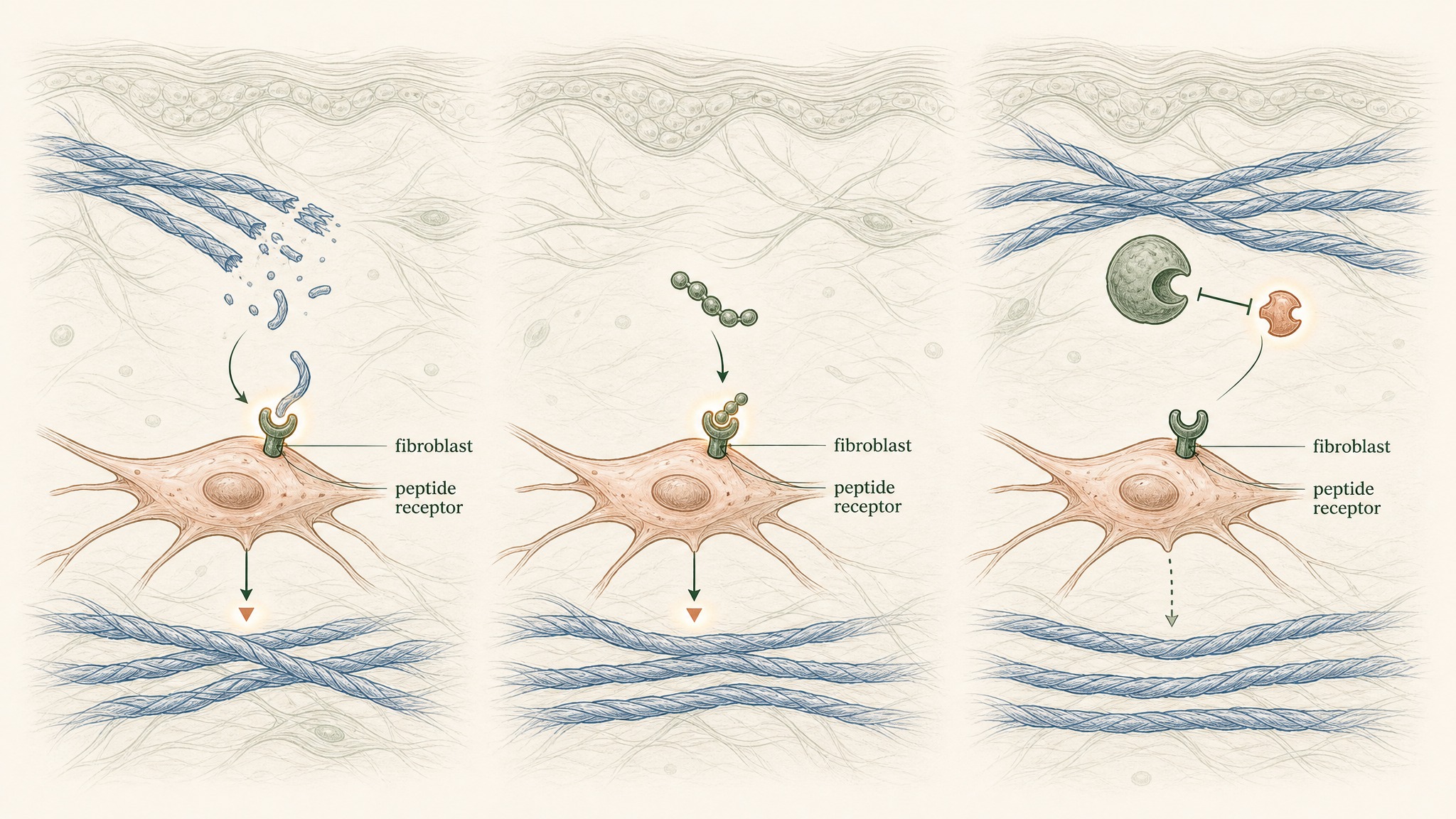
How signal peptides trigger the same collagen-building response as natural breakdown fragments.
There are three functional types in skin care products, each targeting a different stage of the collagen cycle:
- Signal peptides: bind directly to fibroblast receptors and trigger collagen, elastin, and matrix-protein synthesis, the core production side
- Carrier peptides: deliver trace minerals (primarily copper) that enzymes in the dermis need to complete protein synthesis and collagen cross-linking
- Enzyme-inhibitor peptides: slow the enzymes that break old collagen down, shifting the net balance toward more total collagen without touching the production machinery
Understanding these categories matters because products containing them are doing very different things. A signal peptide and an enzyme inhibitor used together target different parts of the same cycle, which is why stacking is common in serious formulations.
The Peptides With Real Evidence Behind Them
Not everything listed as a "peptide" on a label carries equal evidence. Here's where the research actually sits for the compounds you'll encounter most often.
GHK-Cu (Copper Peptide)
GHK-Cu levels drop 40% by age 60, tracking with thinner collagen in your skin.
GHK-Cu sits in a different tier from every other compound in this category. It's a molecule your body already makes, first isolated from human serum and published in Nature New Biology in 1973 (Pickart & Thaler, PMID 4349963). By the time you're 60, your body makes roughly 60% less of it than it did in your twenties, and that decline tracks closely with slowed wound healing and reduced skin collagen density (Pickart & Margolina, Int J Mol Sci 2018, PMC6073405).
In placebo-controlled topical testing, GHK-Cu application produced measurable collagen increases in 70% of participants, outperforming both vitamin C cream and retinoic acid in the same conditions (Pickart et al., Biomed Res Int 2015, PMC4508379). Research suggests GHK-Cu modulates gene expression by at least 50% in roughly a third of all human genes, covering tissue repair, antioxidant defence, and anti-inflammatory signalling (PMC6073405). That's an unusually broad reach for a single small molecule.
Palmitoyl Tripeptides (Matrixyl)
The palmitoyl tripeptide family, palmitoyl tripeptide-1, palmitoyl pentapeptide-4, sold under the trade name Matrixyl, is the most commercially widespread signal peptide group. These compounds mimic collagen-fragment signals, triggering fibroblast synthesis without requiring actual collagen breakdown to occur first. They have meaningful in-vitro collagen upregulation data and a well-understood mechanism.
The palmitoyl (fatty acid) tail attached to the peptide chain improves lipid compatibility, which, as you'll see below, matters a lot for whether anything actually crosses the skin barrier.
Argireline
Argireline (acetyl hexapeptide-3) works differently from everything above. Rather than targeting collagen synthesis, it interferes with the neuromuscular signalling that causes facial muscles to contract, think of it as a much milder version of the mechanism behind botulinum toxin. The mechanism is real and peer-reviewed.
Whether consumer product concentrations produce clinically meaningful expression-line results is a question worth holding with appropriate scepticism.
Enzyme Inhibitors
Leuphasyl and related enzyme-inhibitor peptides slow the matrix metalloproteinases, the enzymes your skin uses to break down old collagen during normal turnover. They tend to play a supporting role in a broader stack rather than carrying results as a standalone ingredient.
How Your Skin's Age Changes What Matters
Peptides aren't equally valuable for the same goals at 32 and at 52. The biology shifts across decades, and what's worth prioritising shifts with it.
In your thirties, collagen production has just begun its slow decline and fibroblast signalling is still relatively active. Signal peptides here are largely a maintenance play, sustaining the system's responsiveness before the steeper drop. Members experience the most efficient return in their thirties because the cellular machinery they're signalling is still capable of a strong response.
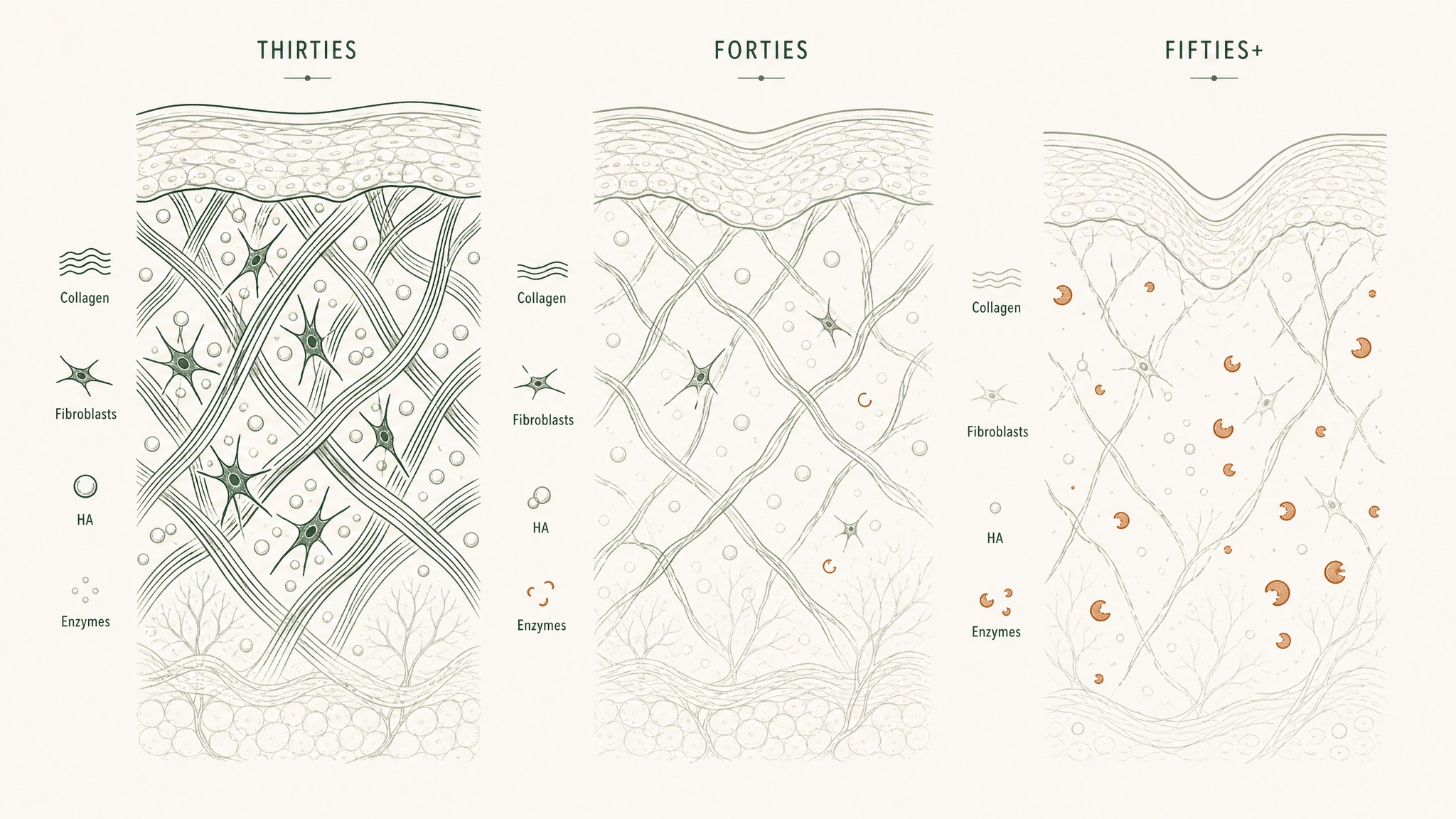
How collagen, fibroblast activity, and enzyme breakdown shift across your thirties, forties, and fifties.
By your forties, signalling slows more noticeably and hyaluronic acid depletion becomes structurally significant. This is where combining a signal peptide (GHK-Cu or palmitoyl tripeptide) with HA makes more sense, because restoring the volumetric environment between fibres supports the structural work the peptide signals are trying to drive.
From your fifties onward, enzyme inhibition becomes more relevant alongside production signalling. When degradation is outrunning synthesis, slowing the breakdown side complements the production signals and shifts the net balance more meaningfully than signal peptides alone.
The Delivery Problem Most Skin Care Brands Don't Explain
Here's the critical gap between the marketing and the biology, and it's one the industry rarely discusses clearly.
Your skin's outermost layer, the stratum corneum, is built like a sealed brick wall from dead skin cells and lipids. It evolved to keep molecules out. The pharmaceutical reference point for whether a compound can cross it is the 500 Dalton rule: molecules above 500 Daltons in molecular weight generally can't cross intact skin in clinically meaningful amounts (Bos & Meinardi, Exp Dermatol 2000, PMID 10839713).
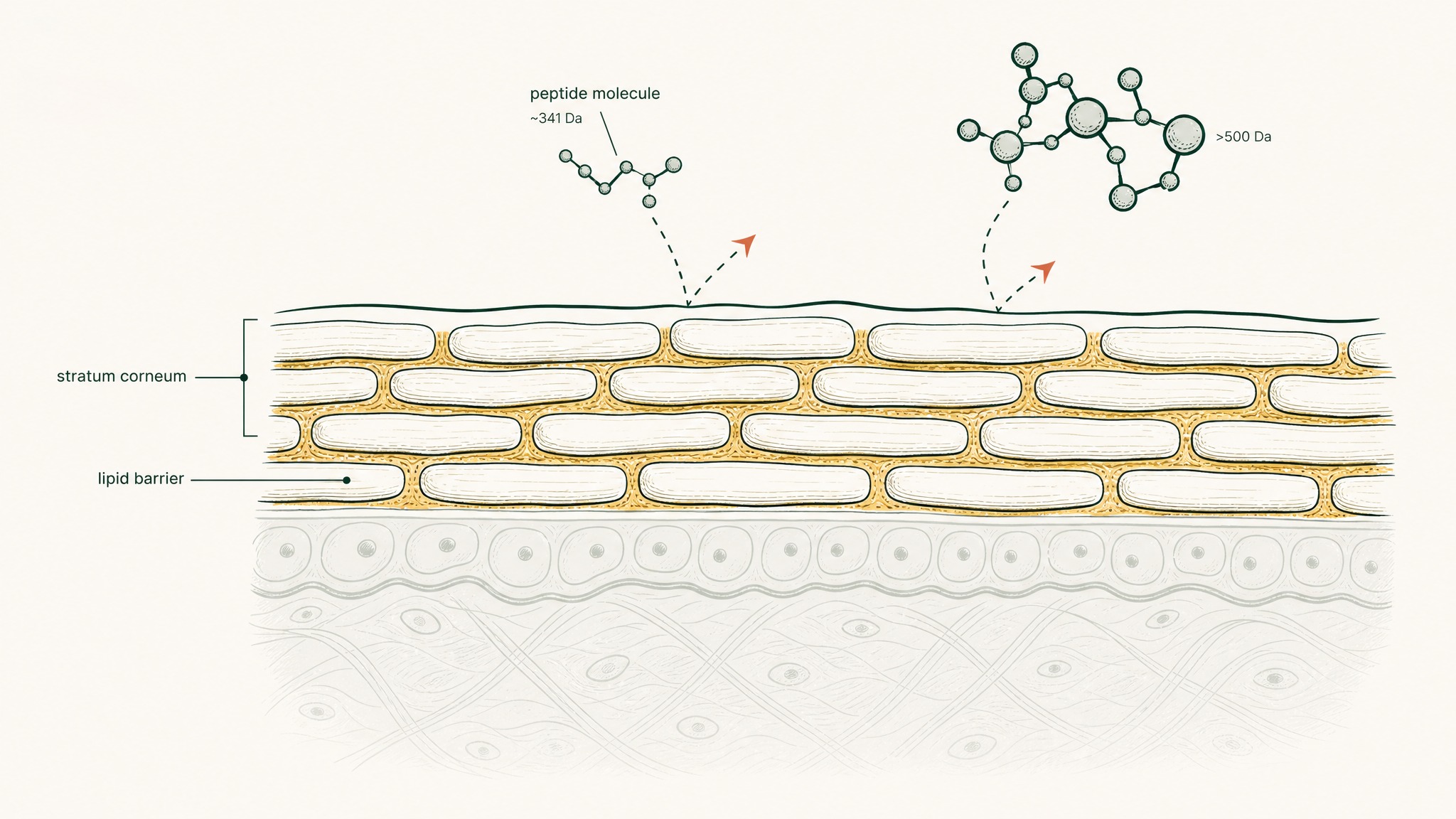
Why small peptides struggle to cross skin's lipid barrier, even when they're light enough to theoretically pass through.
GHK-Cu weighs around 341 Daltons, small enough to pass that test in theory. But there's a second gate: polarity. GHK-Cu is hydrophilic, water-loving, and the stratum corneum is built of lipids.
Water-soluble molecules partition poorly into a fat-based barrier regardless of their size. Most of what you apply to the surface hits that lipid wall and doesn't cross.
Users report noticing this distinction in practice: topical peptide serums produce real surface-level effects, improved hydration, texture, barrier support. What they don't consistently reproduce is the structural dermal change documented in clinical research, which was largely conducted with systemic delivery or specially engineered penetration systems, not standard serum jars.
This isn't a reason to avoid topical peptide products. It's a reason to be precise about what you're asking them to do.
Pairing Peptides With Other Skin Care Actives
Peptides are compatible with most actives in a routine, but a few interactions are worth knowing before you build your stack.
Retinol and peptides work together without conflict. Retinol drives skin cell turnover at the epidermal level; peptides drive fibroblast signalling deeper in the dermis. They're targeting different mechanisms, so layering is fine, apply the peptide serum first, then retinol, then moisturiser.
Vitamin C (L-ascorbic acid) is the main watch-out. L-ascorbic acid is a reducing agent that can degrade peptides in the same formula or applied immediately before or after. The research does support vitamin C as a non-negotiable cofactor in collagen synthesis, it's required at two specific steps in the biochemical pathway where procollagen becomes mature collagen (Pullar et al., Nutrients 2017, PMC5579659).
The fix isn't avoiding vitamin C, it's using a stable derivative (ascorbyl glucoside, sodium ascorbyl phosphate, or 3-O-ethyl ascorbic acid) alongside your peptide serum, or keeping L-ascorbic acid in the morning and peptides in the evening.
A practical layering order for evening use:
- Cleanser
- Toner or essence (if used)
- Peptide serum, applied to slightly damp skin
- Retinol (if part of your routine, it doesn't conflict with peptides)
- Moisturiser or barrier cream
Niacinamide, ceramides, and most barrier-support ingredients sit comfortably at any position in this order.
What Results Actually Look Like, and When
Structural dermal changes don't happen in a week, and knowing the realistic timeline stops you from abandoning a protocol before it's had time to work.
Your fibroblasts begin responding to peptide signals within days, but the structural proteins they produce, new collagen fibres, rebuilt proteoglycan matrix, accumulate over weeks to months. Here's the window the biology actually supports:
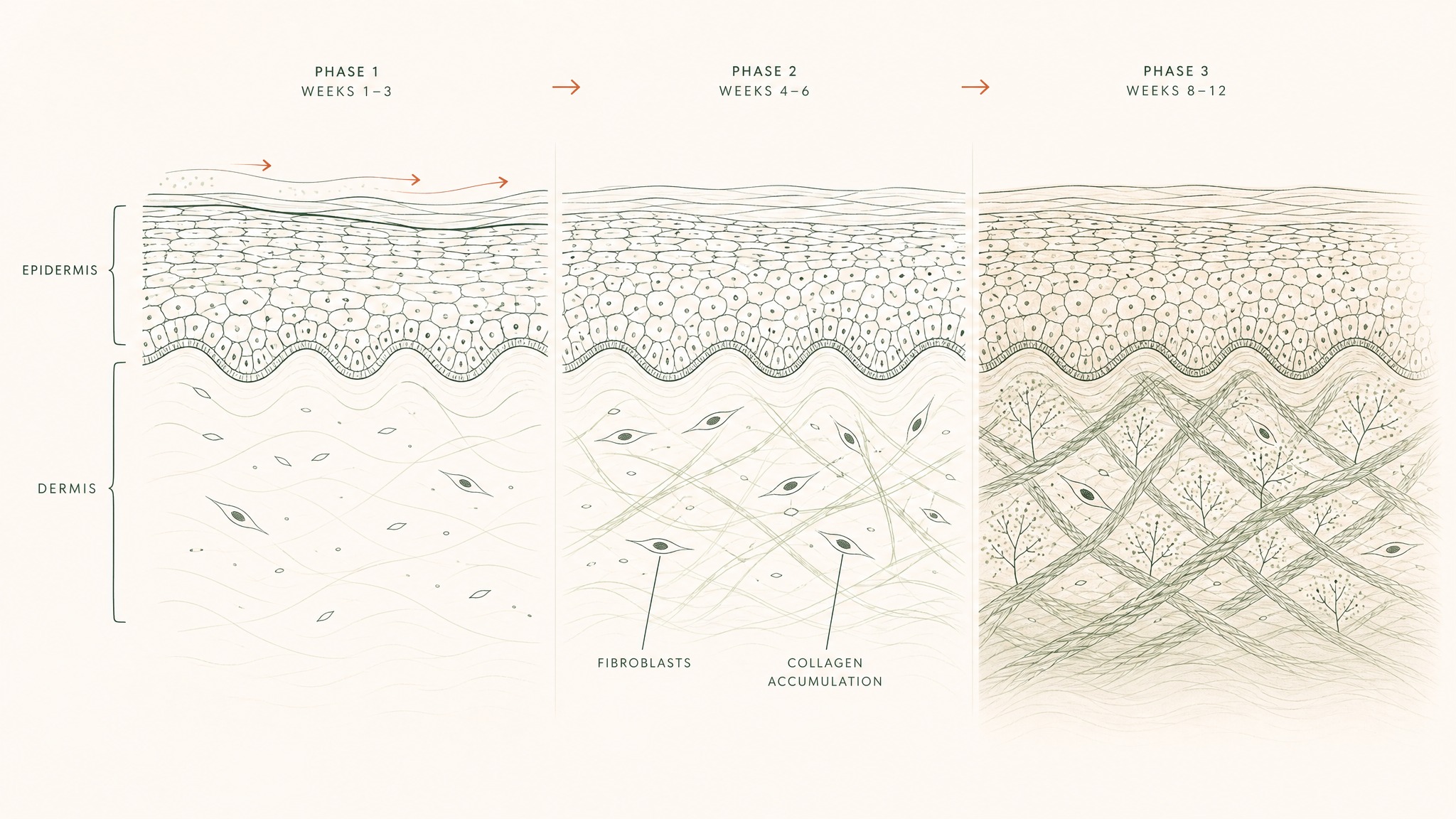
How skin structure rebuilds over twelve weeks as collagen fibers accumulate in the dermis.
- Weeks 1–3: Surface changes are common and genuine, improved hydration, smoother texture, reduced dullness. These reflect the epidermal and barrier-level effects of the hyaluronic acid and surface-active peptide components. No visible skin lifting or firmness change in this window is normal.
- Weeks 4–6: Early firmness changes may become apparent, particularly for those comparing against a baseline photograph. Research suggests collagen synthesis rates are actively responding to ongoing peptide signalling in this phase.
- Weeks 8–12: The primary window for structural dermal change. Members experience the most consistent and documentable results here. The GHK-Cu evidence base reflects protocols of at least 10–12 weeks for skin and connective-tissue endpoints.
The off-period after a defined cycle is as informative as the active phase itself. Changes that persist after stopping suggest actual structural modification. Changes that fade within two to four weeks point toward surface-level response, and that distinction tells you exactly what a second cycle should prioritise.
Going Beyond Topical: When the Surface Isn't the Target
For surface hydration, barrier support, and texture improvement, a well-formulated topical peptide serum is a rational tool. The ceiling is real but it's not nothing.
The GHK-Cu clinical research wasn't measuring surface outcomes. It was measuring what happens when the compound reaches fibroblasts in the dermis, a fundamentally different target.
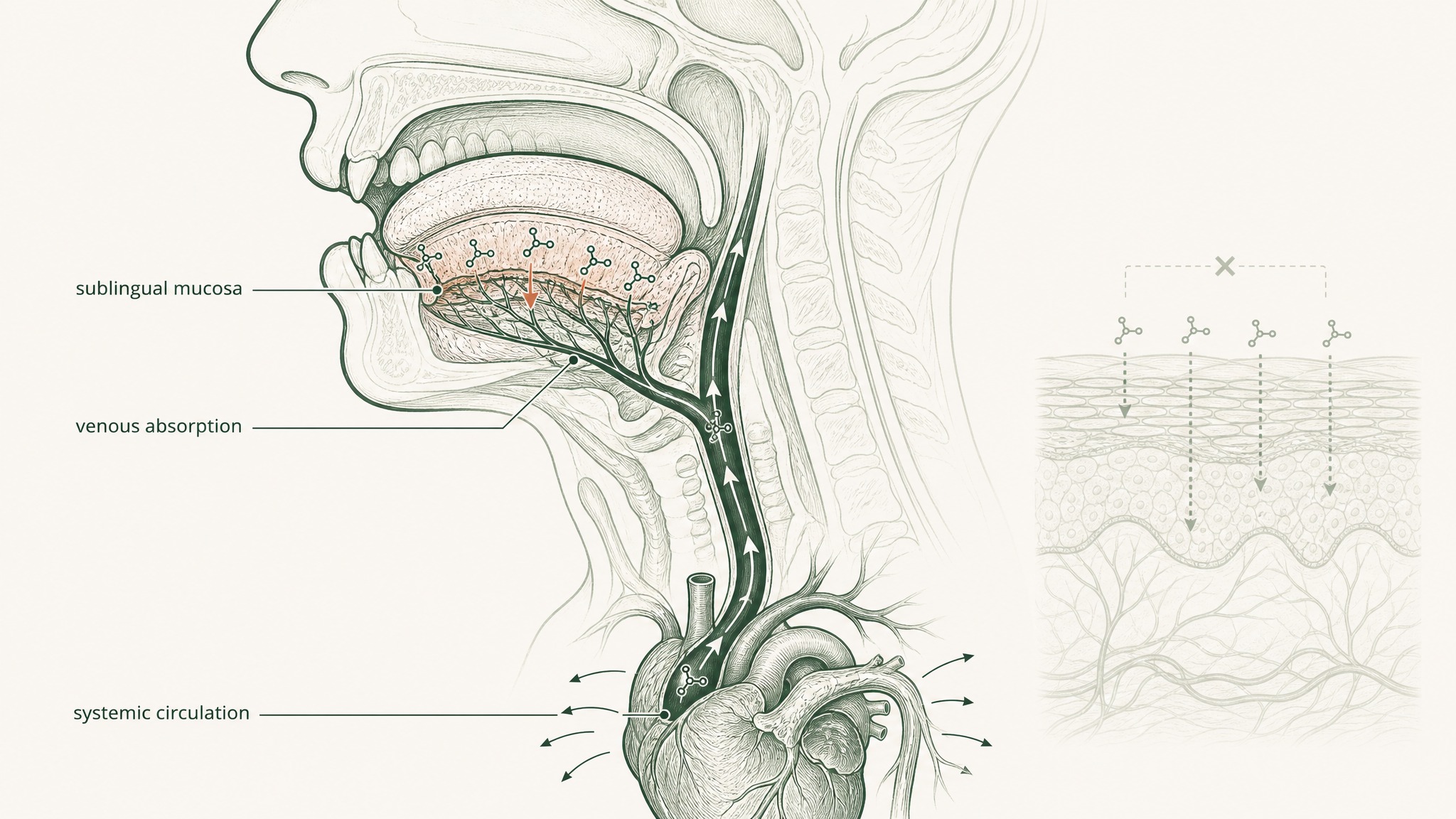
GHK-Cu absorbed under the tongue enters the bloodstream directly, skipping the skin barrier entirely.
When the goal is structural dermal change, the fibroblast signalling, collagen synthesis, and ECM (extracellular matrix, the fibrous scaffold inside your dermis) outcomes the clinical literature documents, the delivery route becomes the primary variable.
Sublingual delivery places the compound under your tongue, where mucosal membranes absorb it directly into venous circulation, bypassing both gut degradation and the stratum corneum barrier entirely. For a hydrophilic peptide like GHK-Cu, that bypass matters more than almost any formulation decision in a topical serum.
VERO's RADIANCE Complex delivers GHK-Cu via the VERISORB sublingual delivery system, a mucoadhesive formulation designed to extend mucosal contact time and assist permeation for hydrophilic compounds. The goal is the systemic compound exposure the published GHK-Cu research was actually measuring, without requiring an injectable. For a full breakdown of the delivery mechanism, the VERISORB guide covers it here.
Frequently Asked Questions
What is the best peptide for skin care?
Research suggests GHK-Cu (copper peptide) has the deepest evidence base, with five decades of published research and placebo-controlled trials showing collagen increases that outperformed vitamin C cream and retinoic acid. Palmitoyl tripeptides (Matrixyl) are the most commercially widespread signal peptide with strong in-vitro data. The right choice depends on whether the goal is collagen production (signal peptides like GHK-Cu or Matrixyl), expression lines (Argireline), or slowing breakdown (enzyme inhibitors).
Do peptide serums actually work on skin?
Users report genuine surface-level results from topical peptide serums: improved hydration, smoother texture, and stronger barrier function. The biological ceiling is delivery. The stratum corneum's lipid barrier blocks most hydrophilic peptides from reaching the dermis in meaningful concentrations, which is why topical serums rarely reproduce the structural collagen changes documented in clinical research using systemic or specially engineered delivery routes.
How long do peptides take to work on skin?
Surface changes (hydration, texture) often appear within 1 to 3 weeks. Early firmness changes may become visible at weeks 4 to 6. Structural dermal change accumulates over 8 to 12 weeks, which matches the protocol length used in most GHK-Cu skin and connective-tissue research. Changes that persist after stopping a cycle suggest structural modification, while changes that fade within two to four weeks point to surface-level response.
Can you use peptides and retinol together?
Yes, peptides and retinol target different mechanisms and do not conflict. Retinol drives epidermal cell turnover at the surface, while peptides signal fibroblasts deeper in the dermis. The standard layering order for evening use is peptide serum first on slightly damp skin, then retinol, then moisturiser.
Can you use peptides with vitamin C?
L-ascorbic acid is a reducing agent that can degrade peptides applied at the same time. Research supports vitamin C as a required cofactor for collagen synthesis, so the fix is not avoiding it. Use a stable derivative (ascorbyl glucoside, sodium ascorbyl phosphate, or 3-O-ethyl ascorbic acid) alongside peptides, or separate them by keeping L-ascorbic acid for the morning and peptides for the evening.
Are peptides safe for sensitive skin?
Topical peptides are generally well tolerated and rarely associated with irritation, since they work by signalling fibroblasts rather than disrupting the barrier. Users with sensitive skin often tolerate peptides better than retinoids or acids. Anyone with active dermatologic conditions or known ingredient sensitivities should consult a qualified healthcare professional before starting a new routine.
When should you start using peptides on your skin?
Research suggests the early thirties is a rational starting point, because that is when natural collagen production begins declining by roughly 1% per year and fibroblast signalling is still highly responsive. Members experience the most efficient return in their thirties when the cellular machinery being signalled is still capable of a strong response. Starting later remains worthwhile, but the protocol emphasis shifts toward combining signal peptides with hyaluronic acid in the forties and adding enzyme inhibition from the fifties onward.
References
- Pickart L, Thaler MM. Tripeptide in human serum which prolongs survival of normal liver cells and stimulates growth in neoplastic liver. Nature New Biology. 1973;243(122):85–87. https://pubmed.ncbi.nlm.nih.gov/4349963/. Retrieved 2026-05-16.
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. Int J Mol Sci. 2018;19(7):1987. https://pmc.ncbi.nlm.nih.gov/articles/PMC6073405/. Retrieved 2026-05-16.
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration. Biomed Res Int. 2015;2015:648108. https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/. Retrieved 2026-05-16.
- Papakonstantinou E, Roth M, Karakiulakis G. Hyaluronic acid: a key molecule in skin aging. Dermatoendocrinology. 2012;4(3):253–258. https://pmc.ncbi.nlm.nih.gov/articles/PMC3583886/. Retrieved 2026-05-16.
- Pullar JM, Carr AC, Vissers MCM. The roles of vitamin C in skin health. Nutrients. 2017;9(8):866. https://pmc.ncbi.nlm.nih.gov/articles/PMC5579659/. Retrieved 2026-05-16.
- Bos JD, Meinardi MM. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp Dermatol. 2000;9(3):165–169. https://pubmed.ncbi.nlm.nih.gov/10839713/. Retrieved 2026-05-16.
RADIANCE™
Coming SoonEngineered around 5mg GHK-Cu. Increases dermal thickness and systemic collagen synthesis
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.