Side effects of TB-500 are thinly characterised in humans. Here's what the one Phase 1 trial reported, what users describe, and the regulatory red flags.
If you go looking for a clean list of "TB-500 side effects" online, you'll mostly find marketing copy. Most product pages skip the topic. Most peptide forums repeat the same three or four anecdotes. The honest picture, drawn from the small human research base and the regulatory record, is messier and more useful than either of those.
Here's the short version. TB-500 has been formally tested in one Phase 1 trial in healthy humans. The trial called it well tolerated. Almost everything else written about TB-500 side effects comes from user reports, animal-model observations, and inference from research on the full parent protein Thymosin Beta-4. The bigger risks sit in three places people rarely look: what's actually in the vial, the regulatory status, and the long-term unknowns.
This article is offered for research purposes only. It is not medical advice. It does not present TB-500 as an approved product, protocol, or therapy for any condition.
The honest summary:
- One published Phase 1 trial in 40 healthy adults reported no serious adverse events at IV doses up to 1260 mg.
- Common user-report side effects cluster around lethargy, a brief head-rush, and injection-site reactions.
- Sourcing risk is a real side-effect category nobody talks about: vial contents vary, contamination is documented.
- TB-500 is banned in all sport under WADA, and the FDA has not approved it for any indication.
- Cancer biology, autoimmune signalling, and pregnancy all sit outside the human research base.
What does the only human safety trial actually report?
The single most useful citation on TB-500 side effects is also the only one of its kind: a Phase 1 trial of intravenous synthetic Thymosin Beta-4 in healthy adults, run by Ruff and colleagues and published in 2010 in the Annals of the New York Academy of Sciences. Forty subjects, four dose tiers, daily IV infusions for fourteen days.
The headline result from that trial: "adverse events were infrequent, and mild or moderate in intensity." No dose-limiting toxicities. No serious adverse events. The pharmacokinetic profile was clean and dose-proportional.
That sounds reassuring, and within the trial's window it is. But here is what trial-design literacy tells you to add in your head before you take it as a blanket safety endorsement:
- Forty subjects is a small sample. Rare events (one in a hundred, one in a thousand) cannot show up.
- Fourteen days is a short window. Long-term signals do not.
- Healthy adults are not the population most TB-500 users belong to. People reaching for repair peptides typically have something they want repaired.
- The synthetic full Thymosin Beta-4 in the trial is not the seven-amino-acid TB-500 fragment sold in research vials.
In our protocol design work, the framing we use with members is that this trial sets a useful floor: in the population it studied, at the doses it studied, the safety signal was clean. It does not promote TB-500 to "broadly safe in humans." That data does not exist yet.
Why is the TB-500 side-effect picture so thin?
Most peptides that reach pharmacy shelves have hundreds of human-trial subjects behind them. TB-500 has forty. That gap is not an accident. It tracks the regulatory route the molecule actually travelled.
Think of the drug-approval pipeline like a long, narrow staircase. Each step costs millions, and only molecules with a clear sponsor (a company that owns the intellectual property and wants the approval) ever climb it. TB-500 does not have one. The closest commercial sponsor, RegeneRx Biopharmaceuticals, ran trials on the full Thymosin Beta-4 molecule, not the TB-500 fragment, and most of their programmes paused or never completed Phase 3.
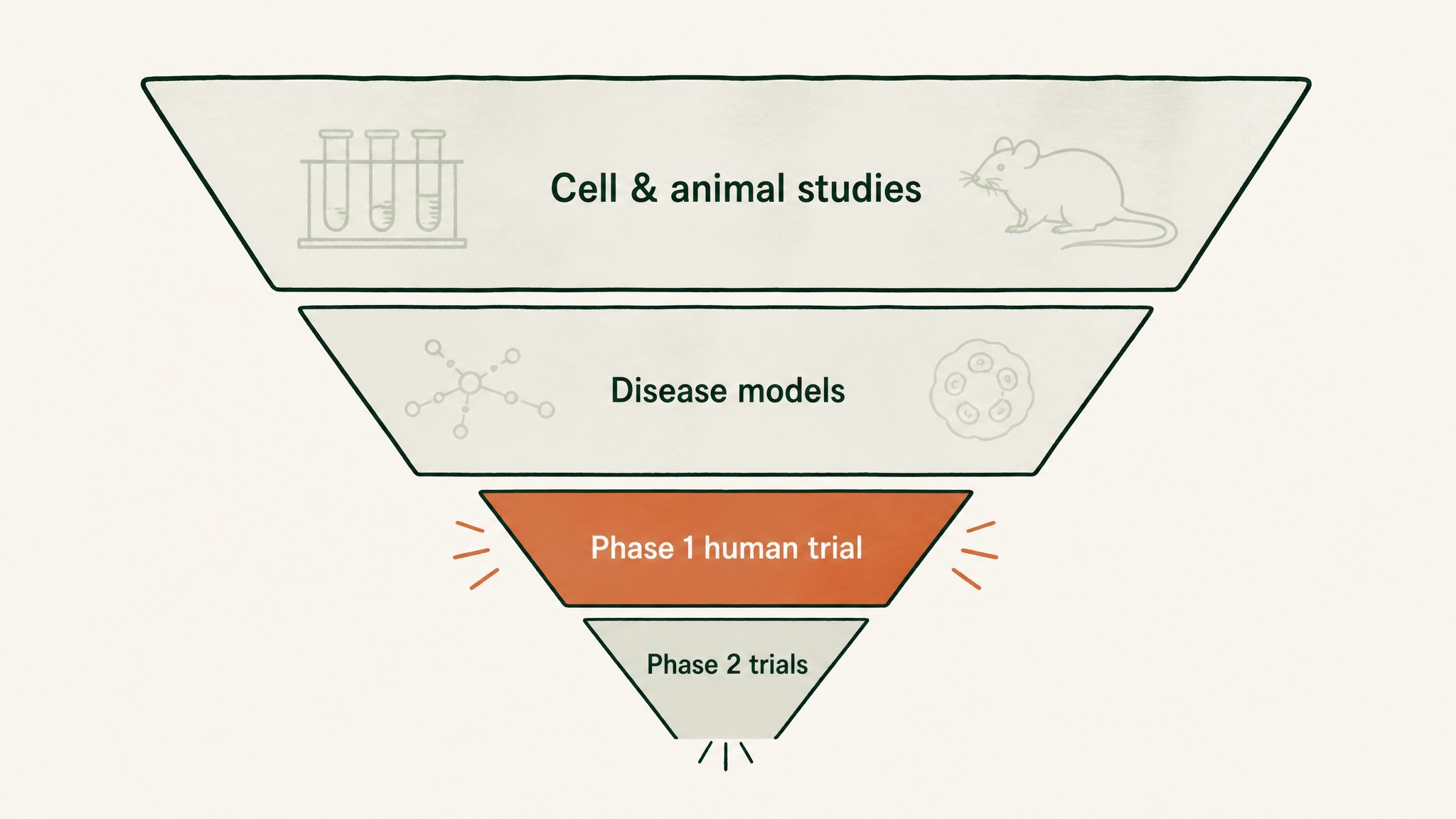
TB-500's research pyramid narrows dramatically from animal studies down to just one small human safety trial.
The result is a research base shaped like an inverted pyramid:
- A wide base of cell-culture and animal-model studies on Thymosin Beta-4
- A narrower band of disease-model preclinical work
- One small Phase 1 human safety trial
- A handful of paused Phase 2 trials in specific indications
- No long-term human safety data at all
Current research suggests the fragment shares the parent molecule's broad actin-binding mechanism, but the side-effect data does not transfer one-for-one. A safety signal seen at one dose of full Thymosin Beta-4 over fourteen days tells you very little about months of weekly subcutaneous fragment injections in a forty-year-old runner with a tendon injury. Members researching the RESTORE protocol sit in that gap, and the appropriate posture is research-cautious, not casual.
What side effects do users report most often?
Forum and clinic reports keep returning to a short, recurring list. None are common, none are well-characterised in formal studies, and all of them are worth understanding before you take any user anecdote at face value.
The four side effects users report most often:
- Lethargy or tiredness in the first 48 hours after a dose, often after the larger loading-phase injections.
- A brief head-rush or light-headedness in the minutes after subcutaneous injection.
- Injection-site reactions including redness, mild swelling, or a small bump that resolves over a day or two.
- Vivid dreams or shallow sleep on dosing nights, particularly when the injection lands close to bedtime.
The lethargy report is interesting because it has a plausible mechanism. TB-500 has been observed to recruit repair cells and quiet pro-inflammatory signalling in animal models. If that biology partially translates to humans, a temporary "your body is in maintenance mode" feeling fits the pattern. It is not formally documented in trial data, but the user-report frequency is high enough that the mechanism deserves attention.
Members experience the injection-site bump most often when they reconstitute with too little bacteriostatic water, which raises the peptide concentration per millilitre and produces more local tissue irritation. That is a sourcing-and-handling variable, not a peptide property.
Does TB-500 cause injection-site reactions?
Subcutaneous and intramuscular peptide injections of any kind can produce small local reactions. TB-500 is no exception. The reactions are typically mild, short-lived, and concentration-dependent rather than dose-dependent.
The pattern users report:
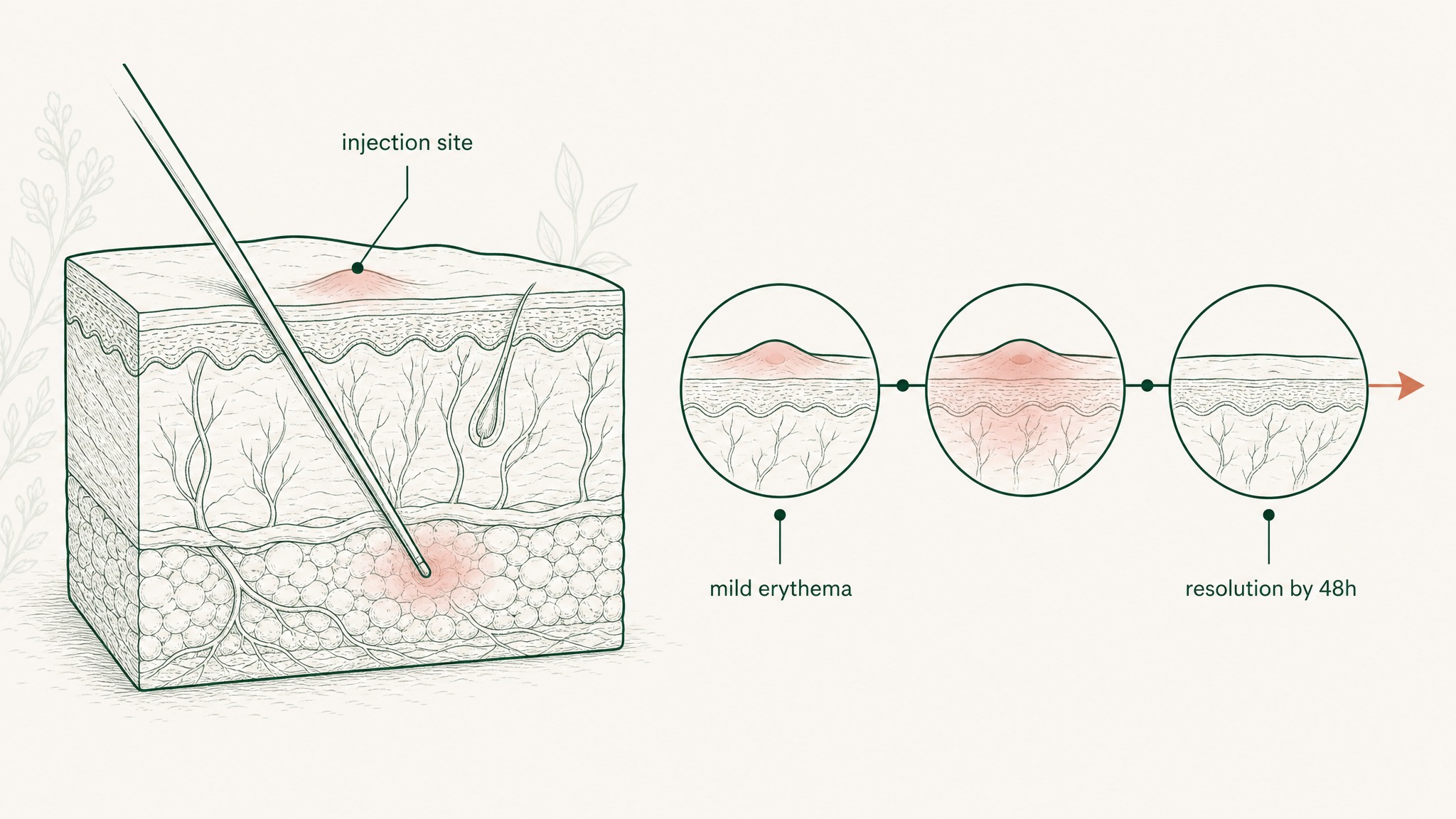
A mild bump and pink area at the injection site typically fade completely within two days.
- A small raised bump or pink area at the injection site, appearing within an hour
- Mild tenderness for 12 to 36 hours
- Full resolution by 48 hours with no marking
A few practical things drive these reactions up or down. Higher concentration per millilitre (smaller injection volume) increases local tissue stress. Cold peptide solution injected straight from the fridge stings more than peptide warmed to room temperature. Repeatedly hitting the same anatomical spot raises the local-reaction rate; rotating sites is the standard mitigation.
If reactions get larger, hotter, or spread visibly outward from the site, that pattern is no longer ordinary irritation. It is the shape of either infection from sterile-technique failure or an allergic-type response to either the peptide or the bacteriostatic preservative. That is a stop-and-reassess situation.
What about lethargy, head-rush, and the systemic feelings?
The "brief head-rush" report is the most consistent systemic effect users describe. Most often it shows up within ten minutes of a subcutaneous injection, lasts under an hour, and feels like a mild vasodilatory flush rather than a stimulant rush.
In our protocol design we regard that report as a real signal even though no trial has documented it formally. The plausible mechanism: TB-500 has been observed in animal models to promote angiogenesis, the growth of new small blood vessels, and to interact with vasoactive signalling pathways. A short systemic effect on vascular tone is mechanism-coherent, even if the trial data does not specifically prove it in humans.
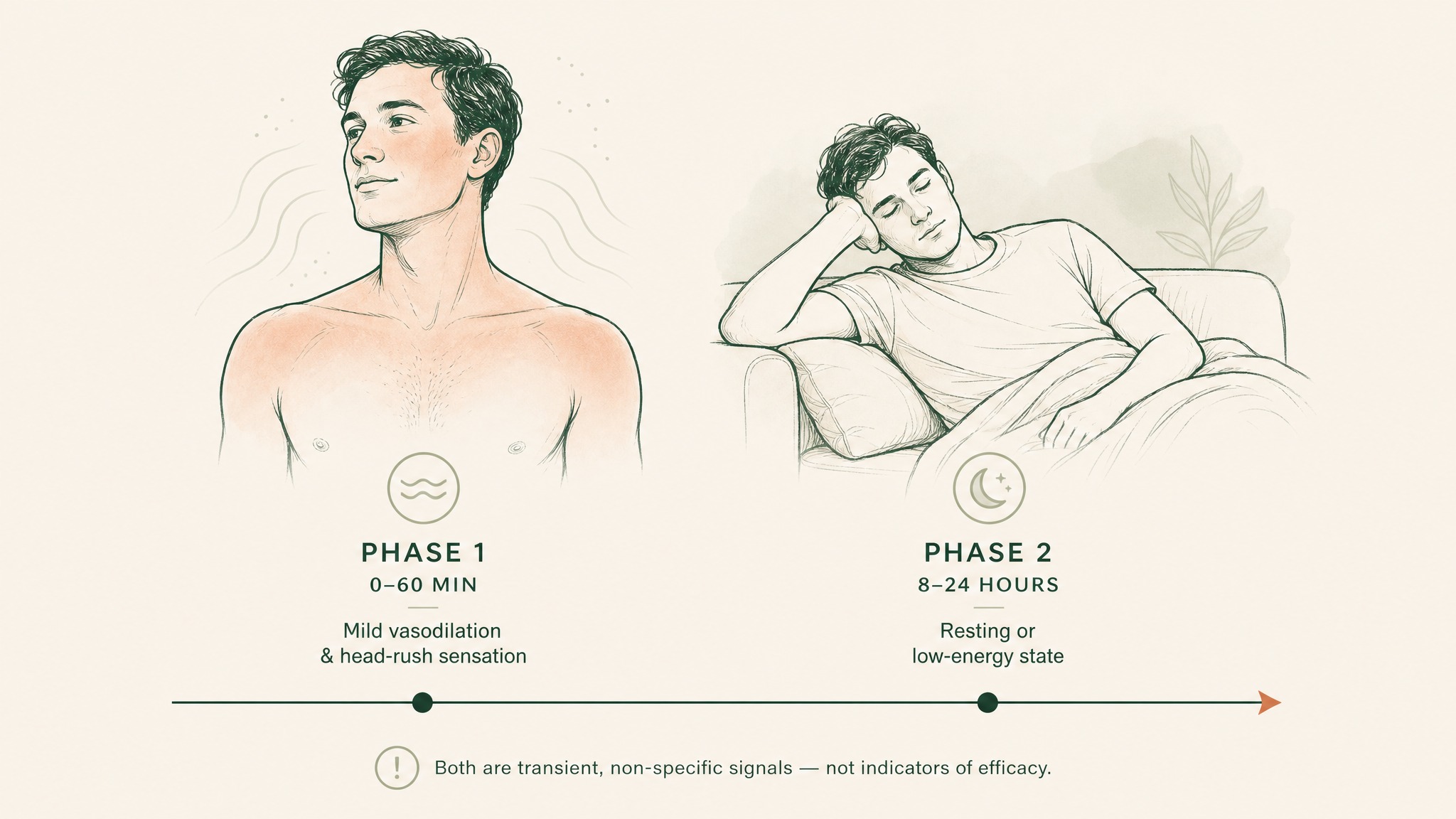
TB-500 typically causes a mild head-rush within ten minutes, followed by lethargy eight to twenty-four hours later.
The lethargy report often pairs with the head-rush, hits in the eight-to-twenty-four-hour window after a dose, and resolves on its own. Practically, that means timing injections away from days that demand sustained alertness is the cheap, sensible move. Evening dosing on a non-driving night is the most common adjustment members make when this shows up.
What you should not do is interpret lethargy as the peptide "working." Tiredness is not evidence of repair. It is, at most, a non-specific signal that some metabolic process is underway.
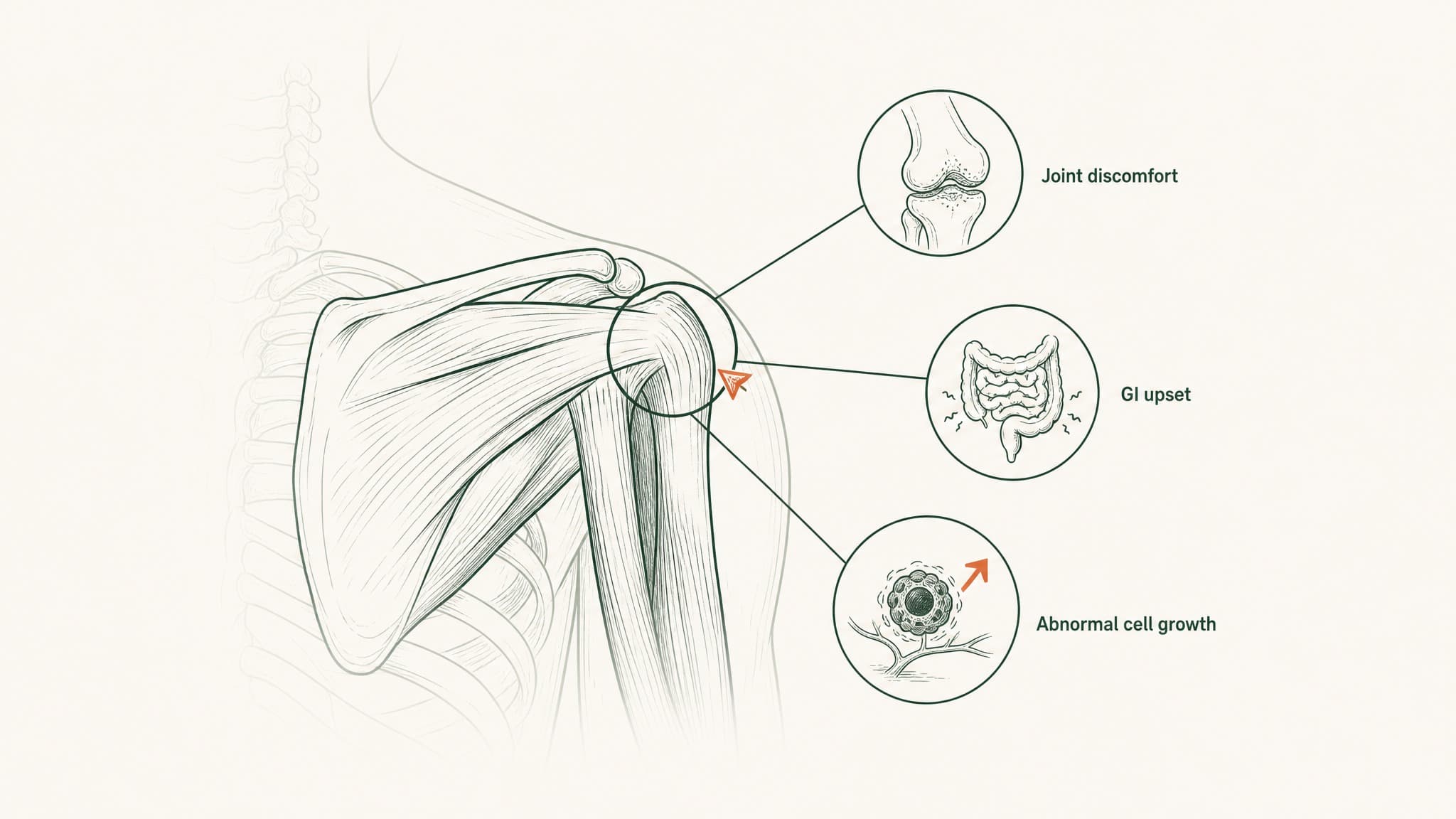
Can TB-500 fuel cancer?
This is the side-effect question that should make any honest peptide article slow down, because the biology is interesting in a way that cuts both directions and the human data simply is not there.
Thymosin Beta-4 supports angiogenesis (new blood vessel growth) and cell migration. Both are exactly the processes a tumour relies on to expand and metastasise. Preclinical work has examined Thymosin Beta-4 expression in various cancer tissues, with mixed signals: some tumour types show elevated expression that tracks with worse outcomes, others do not.

How tumors rely on new blood vessel growth to expand and spread to other parts of the body.
The honest framing has three layers:
- No human study has shown that TB-500 administration causes or accelerates cancer.
- No human study has shown it does not. The trial does not exist.
- The mechanistic plausibility is enough that researchers with active cancer, recent cancer, or strong family-history risk should regard TB-500 as outside their research window.
This is one of the places where the regulatory caution lines up with biological caution. The FDA has flagged TB-500 in its Category 2 list for compounded peptides partly because the in-vitro and animal-model signals raise enough concern to warrant more data before clinical use. Until that data lands, "we don't know" is the only honest answer, and "default to opt out if you sit in a higher-risk group" is the only conservative one.
Why is TB-500 banned in sport?
TB-500 sits on the WADA Prohibited List under Section S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). The Voluntary Anti-Doping Association mirrors that classification on its 2026 list. The ban is in-competition and out-of-competition, meaning it applies year-round to athletes covered by WADA-aligned testing.
The reason is straightforward in regulatory logic: TB-500 has been observed in animal models to support tissue repair, angiogenesis, and possibly performance-relevant recovery. That puts it squarely inside the category WADA prohibits.
For the side-effects conversation, the ban matters in two practical ways:
- Tested athletes who use TB-500 face career-ending sanctions, not health side effects, but regulatory side effects that can be just as costly.
- WADA's classification implies the underlying biology is taken seriously enough to prohibit at the international-sport level. That is not the language a regulator uses for a substance considered inert.
The pattern across regulators (FDA non-approval, WADA prohibition, FDA Category 2 compounding flag) is consistent: TB-500 is treated as biologically active enough to warrant restriction, and unknown enough to make casual human use a meaningful risk.
What's the FDA's position on TB-500?
Three things, none of them flattering for the "this is just a supplement" framing the marketing prefers:
- TB-500 has no FDA approval for any clinical indication.
- The FDA has classified Thymosin Beta-4 (the parent molecule TB-500 is derived from) in its Category 2 list for 503A compounding, which restricts pharmacy compounding under that section.
- Commercial "research peptide" channels selling TB-500 operate outside the FDA's approved-drug framework. Research suggests labelling accuracy and purity vary substantially across that channel.
That last point is the regulatory side effect almost nobody on a peptide forum flags. The Esposito et al. characterisation paper from 2012 confirmed that commercial vials labelled "TB-500" contained the N-terminally acetylated 17-23 fragment of Thymosin Beta-4. That is reassuring on identity for the products tested. It does not tell you anything about the vial you might buy in 2026 from a different supplier with different quality-control practices.
Members researching peptide protocols at the conservative end of the spectrum regard sourcing risk as the single biggest side-effect variable. A vial that contains the wrong fragment, or a contaminated fragment, has a side-effect profile that no published study can describe. For wider context on what reputable channels test for and how the regulatory map sits, the what is TB-500 guide covers the identity and sourcing layer in detail.
How does delivery route change the side-effect picture?
Most TB-500 research uses subcutaneous or intramuscular injection at the user end and intravenous infusion at the trial end. The side-effect profile shifts with the route in predictable ways.
A quick comparison of how route changes the picture:
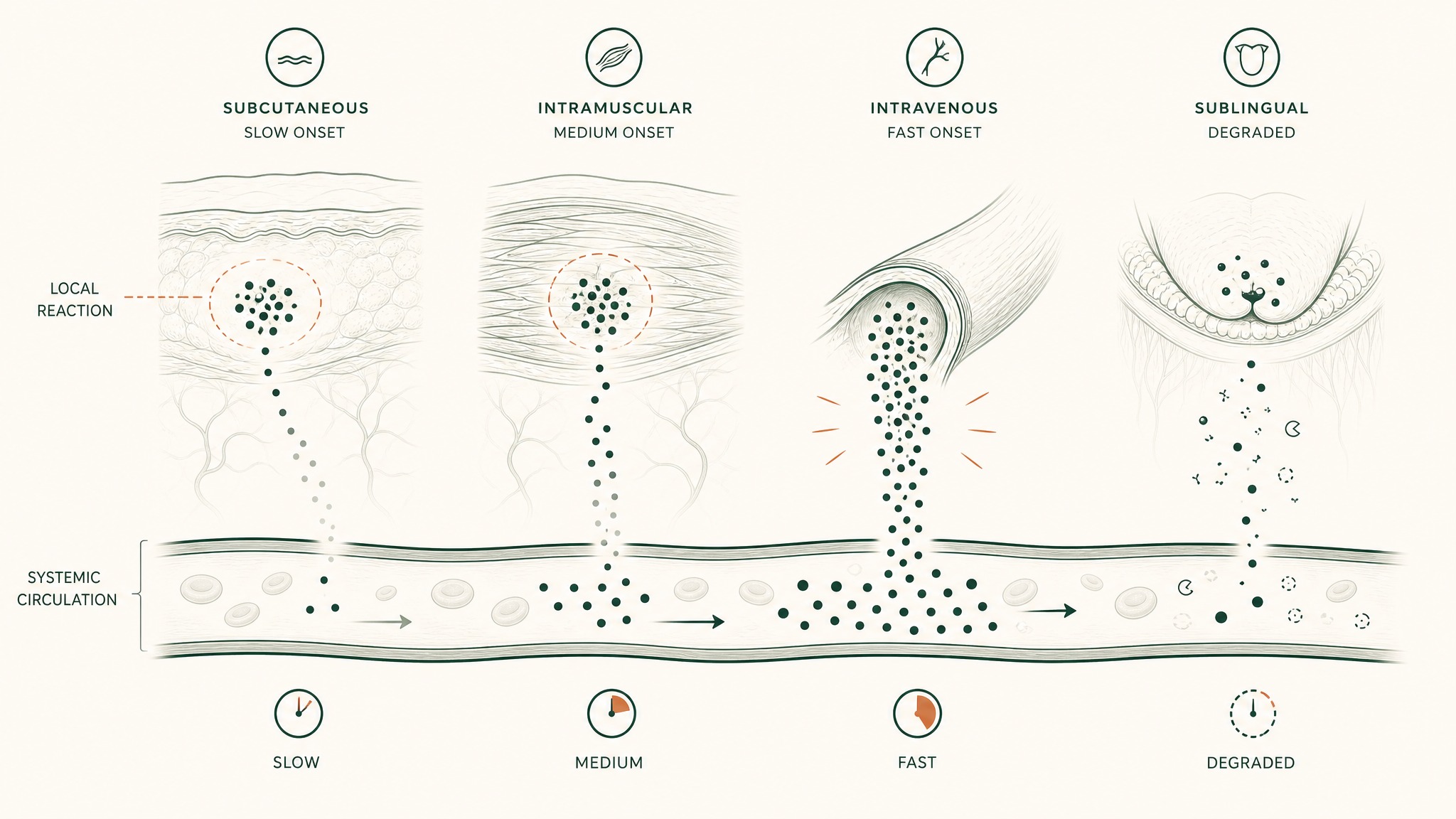
How TB-500 reaches your bloodstream differently depending on injection type or route.
- Subcutaneous (most common user route): Injection-site reactions and the head-rush sit here. Systemic onset is gradual.
- Intramuscular: Slightly faster systemic onset, similar local-reaction rate, often less surface bruising.
- Intravenous (used in the Ruff Phase 1 trial): No injection-site reactions in the user sense, but any infusion-related effects (vasodilation, flush) are amplified by the rapid systemic delivery.
- Sublingual or oral research peptides (a separate research area): Bypass injection-site reactions entirely. Bioavailability and degradation become the relevant variables instead.
VERO's research into VERISORB sublingual delivery is focused on the bioavailability question for peptides where injection is the bottleneck for member compliance. For TB-500 specifically, the published literature is injection-based; any sublingual research framing is downstream of separate absorption work.
Who should not research TB-500 at all?
A short, conservative list of "outside the research base":
- Pregnancy and breastfeeding. No human safety data. Default to opt out.
- Active cancer or recent cancer history. Mechanistic concerns, no human data to set them aside.
- Strong family-history cancer risk. Same logic, applied earlier.
- Children and adolescents. No dosing or safety base in this population.
- People on immunosuppressive therapy. TB-500 has been observed to modulate immune-related signalling; interactions are unstudied.
- People with significant cardiovascular disease. The Ruff Phase 1 trial was in healthy adults; the cardiac-population safety data is paused or absent.
- Anyone in WADA-tested sport. Regulatory side effects (sanction, career impact) outweigh any health framing.
This is the conservative-default version, not a comprehensive contraindication list. The general principle: if you sit outside the population the small published trial enrolled, the published safety data does not cover you.
How should researchers think about long-term unknowns?
The longest-running human safety follow-up on TB-500 or full Thymosin Beta-4 is measured in weeks, not years. That is the empirical ceiling on confidence in long-term safety.
Three honest unknowns to hold in mind:
- Cumulative immune-signalling effects. Repeated dosing across years has not been studied.
- Chronic angiogenesis modulation. New blood vessel growth supports repair; in the wrong tissue context it supports other things too.
- Sourcing drift. A protocol that worked safely at one supplier in 2024 is not the same product if the supplier has changed processes in 2026.
Users report stacking TB-500 with BPC-157 for joint and tendon research as if it were a routine combination. The honest read is that the combination has been observed in some animal models and reported informally by user communities. It has not been studied for combination safety in any human trial. For background on the most-studied repair-peptide comparison, the BPC-157 dose article covers the mechanism contrast.
Key Takeaways
- The one published Phase 1 human safety trial of synthetic Thymosin Beta-4 reported only mild or moderate adverse events in 40 healthy adults, with no dose-limiting toxicities. The trial used the full parent molecule, not the TB-500 fragment specifically.
- User-report side effects cluster around lethargy, a brief head-rush, mild injection-site reactions, and occasional sleep disturbance.
- Long-term human safety data on TB-500 does not exist. Trials run weeks, not years.
- Cancer biology, autoimmune conditions, pregnancy, and paediatric populations sit outside the research base. Conservative researchers opt out.
- TB-500 is banned at all times under the WADA Prohibited List Section S2, and is not FDA-approved for any indication.
- FDA Category 2 classification under 503A reflects the regulator's assessment that more data is needed before clinical compounding is permitted.
- Sourcing risk is a real side-effect category. Vial contents, purity, and labelling accuracy vary by channel.
- Delivery route shifts the side-effect picture. Subcutaneous injections produce most user-reported local reactions. Sublingual delivery routes are a separate research area entirely.
- Members researching the RESTORE protocol should read this article as background context, not protocol guidance. Speak to a qualified clinician before adding any peptide research to your practice.
References
- Ruff D, Crockford D, Girardi G, Zhang Y. (2010). Phase 1 safety and pharmacokinetic profile of intravenous thymosin beta-4 in healthy volunteers. Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536472/. Retrieved 2026-06-19.
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. (2012). Thymosin beta-4 as a multifunctional regenerative peptide: review of basic properties and clinical applications. Expert Opinion on Biological Therapy. https://pubmed.ncbi.nlm.nih.gov/22074294/. Retrieved 2026-06-19.
- Crockford D, Turjman N, Allan C, Angel J. (2010). Thymosin beta-4: structure, function, and biological properties supporting research applications. Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536467/. Retrieved 2026-06-19.
- Esposito S et al. (2012). Synthesis and characterisation of the N-terminal acetylated 17-23 fragment of thymosin beta-4 identified in commercial TB-500. Drug Testing and Analysis. https://analyticalsciencejournals.onlinelibrary.wiley.com/doi/abs/10.1002/dta.1402. Retrieved 2026-06-19.
- Philp D, Kleinman HK. (2010). Animal studies of thymosin beta-4 in tissue repair and regeneration (review). Annals of the New York Academy of Sciences. https://pubmed.ncbi.nlm.nih.gov/20536453/. Retrieved 2026-06-19.
- Goldstein AL, Hannappel E, Kleinman HK. (2005). Thymosin beta-4: actin-sequestering peptide with tissue-repair signalling. Trends in Molecular Medicine. https://pubmed.ncbi.nlm.nih.gov/16099219/. Retrieved 2026-06-19.
- World Anti-Doping Agency. The Prohibited List (Section S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics). https://www.wada-ama.org/en/prohibited-list. Retrieved 2026-06-19.
- Voluntary Anti-Doping Association. VADA Prohibited List version 1-1-2026 (Section S2 classification of TB-500). https://vada-testing.org/wp-content/uploads/2025/12/VADA-Prohibited-List-2026-.pdf. Retrieved 2026-06-19.
- Banned Substances Control Group. TB-500: status, risks, and bans in sport and military settings. https://www.bscg.org/blogs/single/tb-500-status-risks-and-bans-in-sport-and-military. Retrieved 2026-06-19.
- U.S. National Library of Medicine. ClinicalTrials.gov NCT00311766 (Phase 2 registry record of Thymosin Beta 4 in dermal repair research). https://clinicaltrials.gov/study/NCT00311766. Retrieved 2026-06-19.
For research purposes only. Curious how VERO formulates tissue-repair peptide research? Explore the RESTORE protocol →
RESTORE™
BPC-157Engineered around 500mcg BPC-157. Accelerates deep tissue and joint recovery
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.