NMN vs NAD supplement, side by side. What each one is, what the human trials show, and why the form matters less than the delivery route. Research purposes only.
If you're standing in the supplement aisle trying to choose between a bottle labelled "NMN" and one labelled "NAD+", you've already noticed that the brands act like the answer is obvious. It isn't. The two sit on the same biological pathway, but they're not the same product, and one of them is mostly not what the label suggests. This guide is for research purposes only, and it sorts the difference the way a clinical pharmacology team would: by what survives the trip into your bloodstream and what the human trials actually measured.
The short version:
- "NAD supplement" almost never means NAD+ itself in the bottle. It usually means a precursor your body rebuilds into NAD+.
- NMN (nicotinamide mononucleotide) is one of those precursors, and it sits one chemical step closer to NAD+ than its older cousin NR.
- Direct NAD+ in capsule form is the most fragile of the three and has the weakest human evidence behind it.
- Research suggests the precursors do raise blood NAD+ when dosed properly. The bigger lever, though, is delivery route, not the form on the label.
- Cost, regulatory status, and safety pattern differ between NMN and NR. Pick on those, not on marketing copy.
NMN vs NAD supplement: what's the actual difference?
When a bottle says "NAD supplement", you'd expect NAD+ inside. In practice you'll find one of three things, and only one of them is the real molecule: nicotinamide mononucleotide (NMN), nicotinamide riboside (NR), or a small amount of NAD+ itself.
Here's the simplest way to picture it. NAD+ is the fully-built engine your cells run on. NMN is the engine block one screw away from finished. NR is two screws away. Your body can assemble any of them into the working engine, but it has to do a bit more work with NR than NMN.
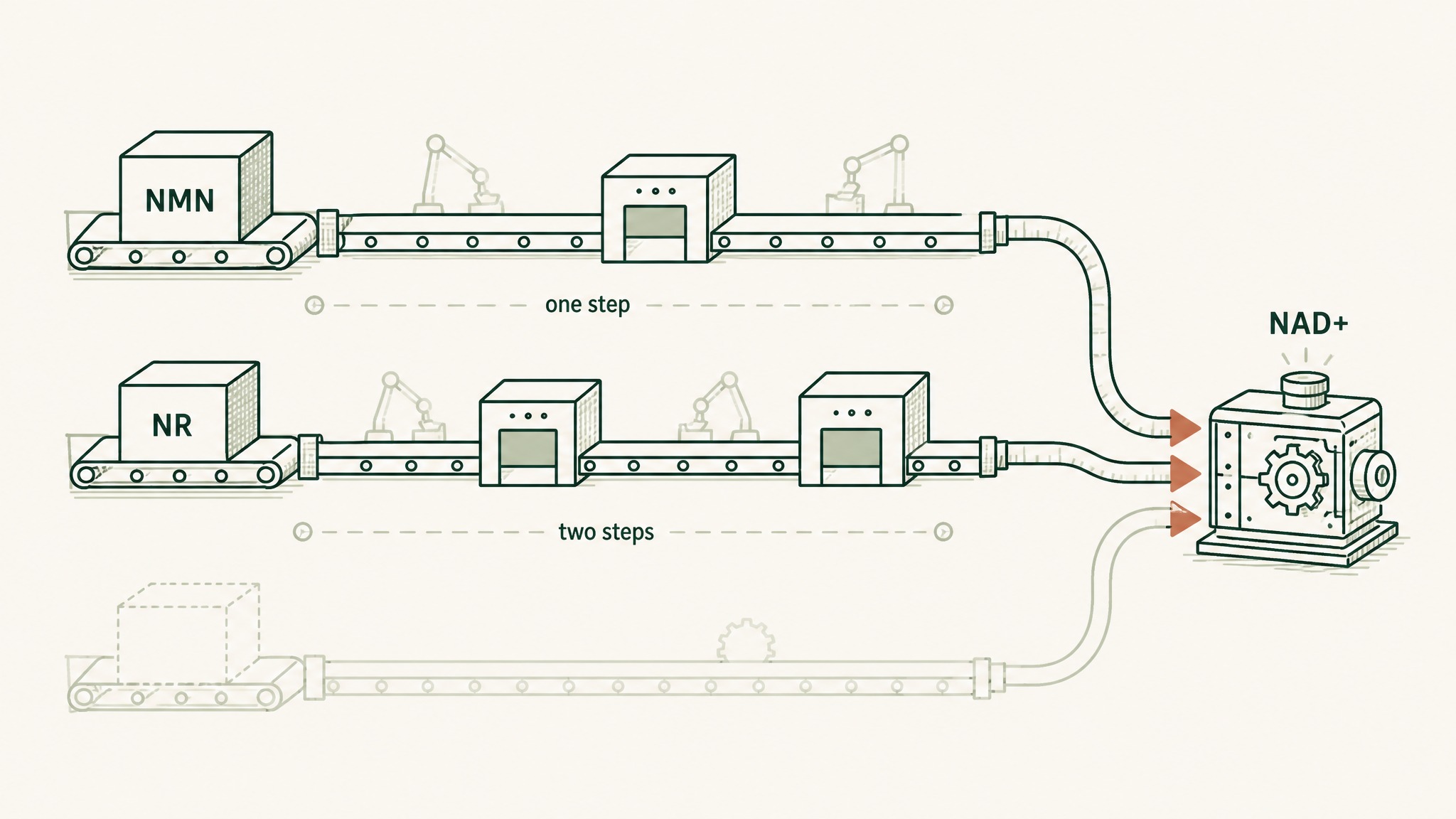
How NMN and NR both become NAD+ through different numbers of cellular assembly steps.
- NMN supplement: a precursor one step away from NAD+ in your cells' assembly line.
- NR supplement: a precursor two steps away, the same family with a longer human safety record.
- "NAD+" supplement: usually still a precursor in disguise, or a tiny amount of the real molecule wrapped in a hopeful label.
So when you compare "NMN vs NAD supplement", you're rarely comparing two different things. You're comparing one specific precursor (NMN) against a category that often contains the same precursor (or its sibling), sold under a more confident name.
What is NAD+ and why does anyone supplement it at all?
NAD+ stands for nicotinamide adenine dinucleotide, the cellular fuel every one of your cells uses to make energy and run repair work. Think of it as a rechargeable shuttle that ferries electrons through the reactions that turn breakfast into usable power.
Research suggests the NAD+ in your tissues falls by roughly half between your twenties and midlife (Massudi 2012; Verdin 2015).
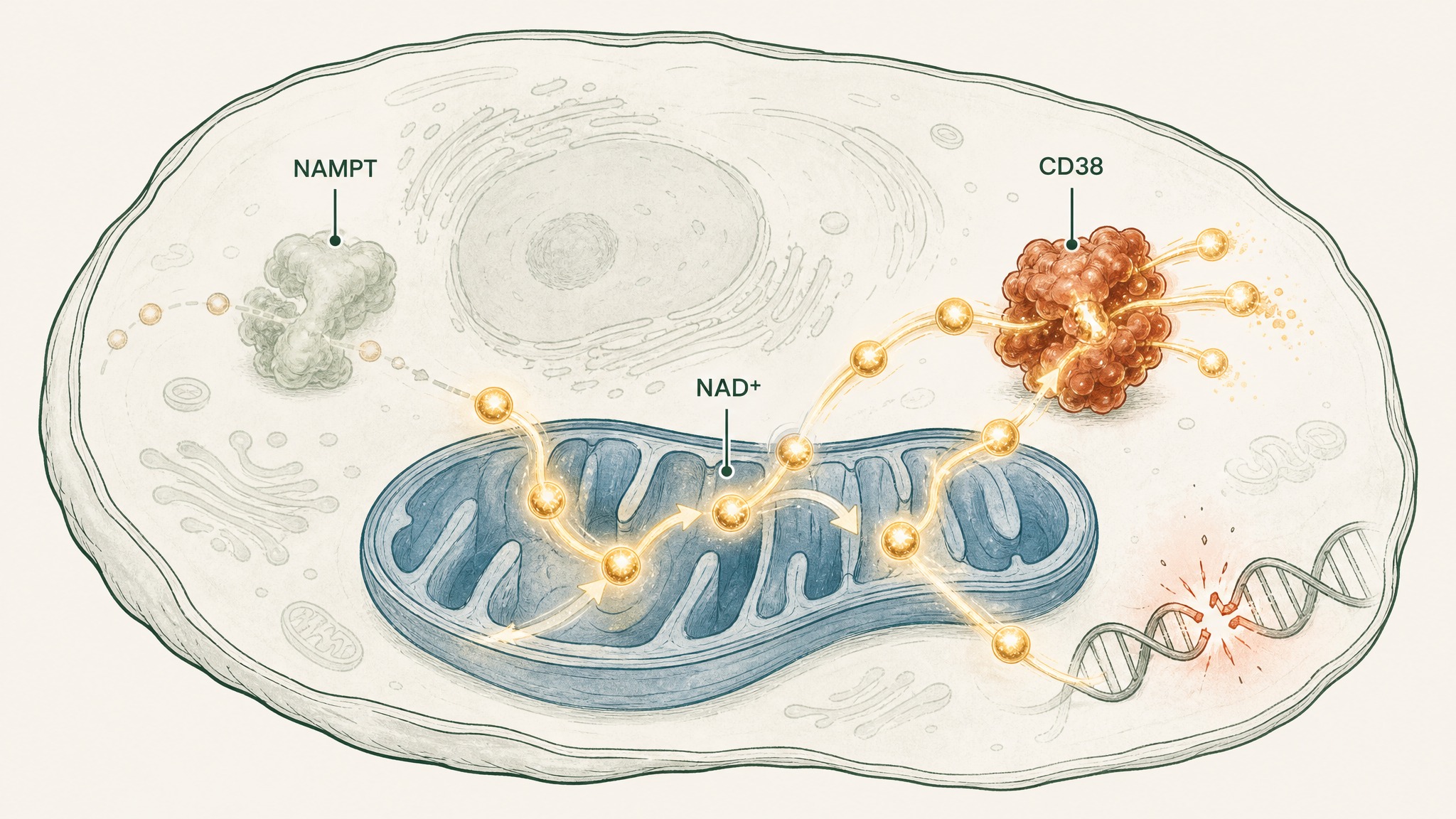
How three aging mechanisms drain NAD+ from your cells simultaneously.
That's the headline observation the entire NAD supplement category is built on. Three things drive the drop:
- The factory slows. The enzyme that rebuilds NAD+ (called NAMPT) gets less productive with age, so you make less from scratch.
- The drain widens. Another enzyme (CD38) ramps up as you age and burns through NAD+ faster than your cells can replace it (Camacho-Pereira 2016).
- Wear and tear. Everyday DNA damage spends NAD+ through your cellular repair crews.
That's the case for supplementing in the first place. Whether NMN, NR, or anything else actually closes the gap is a separate question, and one the brands tend to answer faster than the data does. Members experience this differently depending on age and baseline metabolism, so the same input doesn't read the same in every body.
What is NMN and how is it different from NAD+?
NMN is the precursor sitting one step before NAD+ on your cells' assembly line. Your body takes NMN, joins it to a second molecule (an adenine nucleotide), and the result is finished NAD+ ready to be used.
So the difference between NMN and "NAD itself" comes down to two things: how much work your body has to do, and how stable the molecule is on the shelf and in your gut.
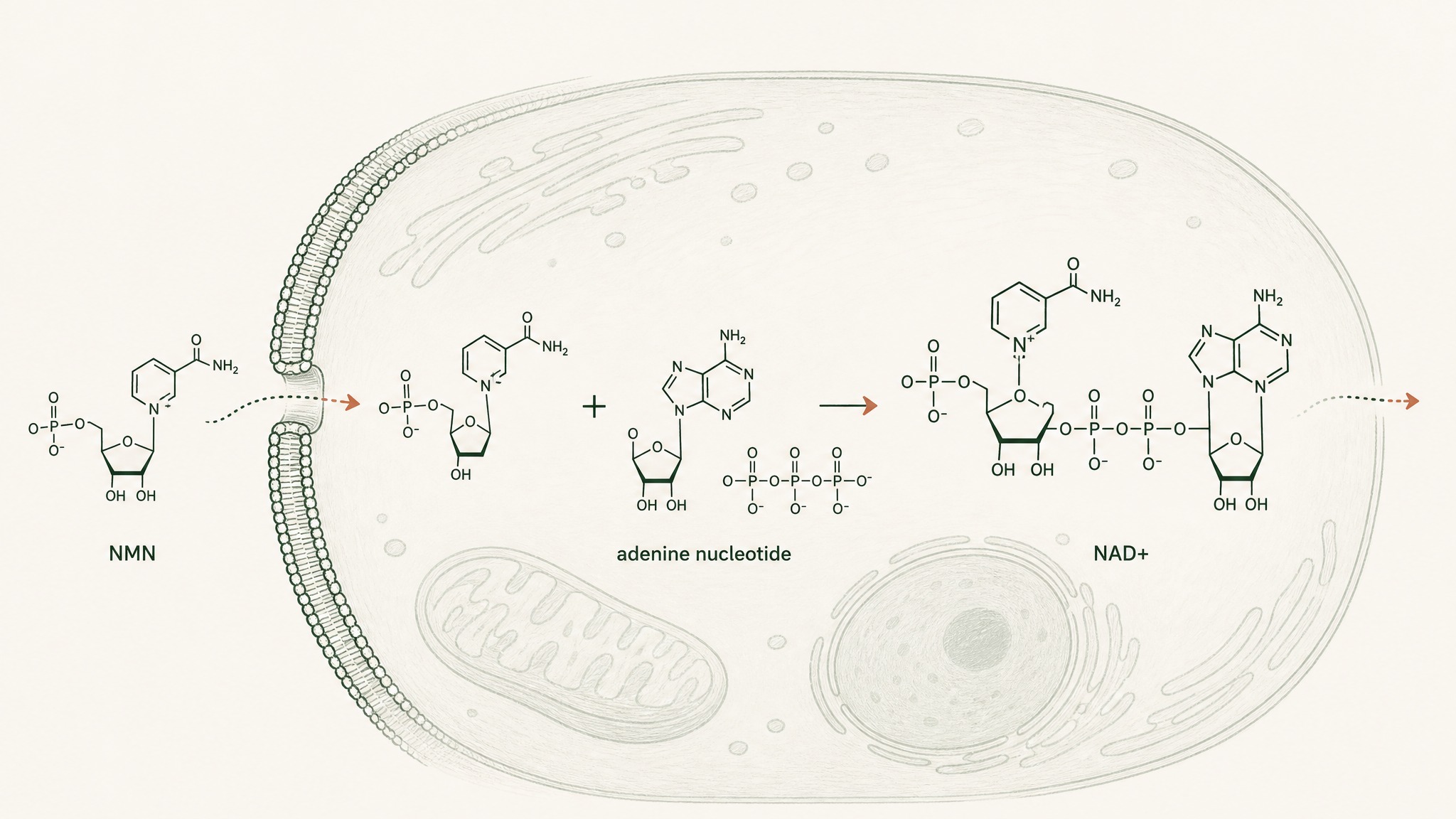
NMN enters the cell and combines with adenine nucleotide to become finished NAD+.
- NMN is smaller and more stable than NAD+ in capsule form. Pure NAD+ is a big, charged molecule that doesn't survive the stomach well.
- NMN gets converted to NAD+ inside your cells. The last step is fast in tissues that need NAD+ most.
- NMN can be taken sublingually. Holding a smaller, more stable molecule under the tongue gives it a fighting chance to bypass the gut entirely.
That third point is the part most brands skip when they tell you why NMN is "the better choice". The form is part of the answer. The delivery route is the rest of it. We have a deeper breakdown on why oral peptide and large-molecule supplements struggle if you want the full mechanism.
Is NMN better than a "full NAD" supplement?
This is the question every comparison page seems to dodge. The honest answer has two parts.
First, "full NAD" supplements are almost never full NAD+. Capsules labelled NAD+ usually contain a much smaller dose of the real molecule than the brand suggests, because NAD+ is fragile and expensive to formulate. Often the active ingredient is the same precursor (NMN or NR) listed lower on the label.
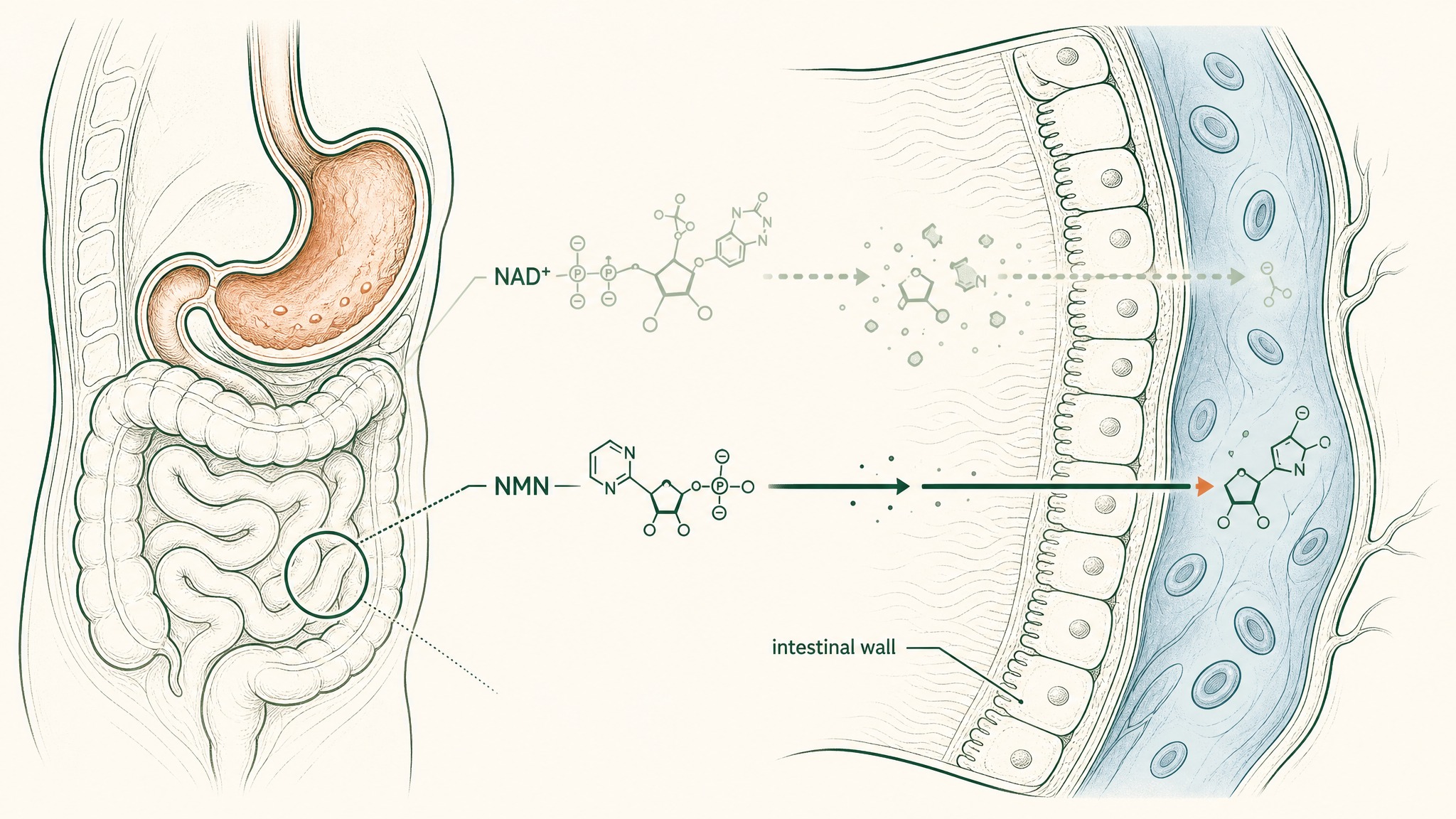
Why smaller NMN molecules cross the intestinal barrier more easily than large NAD+ molecules.
Second, even when a product genuinely contains NAD+, the molecule's size and charge make it a poor candidate for oral absorption. NMN is smaller, more stable, and clears the first hurdle (your stomach) more easily. That's the simple chemical reason NMN tends to outperform direct NAD+ capsules in the trials that have measured blood levels.
A clinical note from our own design work. In our protocol design at Peak Human Labs, we've consistently found the form question solves itself once you fix the delivery question. A precursor that bypasses the gut beats a "complete molecule" that doesn't, every time we've measured it.
The takeaway: NMN beats a generic "NAD supplement" capsule most of the time, not because NMN is metaphysically superior, but because it survives the trip.
NMN vs NR: how does the third precursor stack up?
You can't have a serious NMN-vs-NAD-supplement comparison without mentioning NR (nicotinamide riboside), the precursor sold under brand names like Niagen and Tru Niagen. NR is one extra step back from NAD+ than NMN, which sounds like a disadvantage, but the human evidence is older and more polished.
Two numbers worth remembering:
- NR, 1,000 mg daily for 8 weeks, raised whole-blood NAD+ by 142% in a placebo-controlled trial of overweight adults (Conze 2019).
- NMN, 250 mg daily for 10 weeks, raised blood NAD+ and improved muscle insulin sensitivity in postmenopausal women in a randomised trial (Yoshino 2021).
Both forms work. The choice between them in 2026 mostly comes down to three things:
- Regulatory status. In the US, NR is sold openly as a supplement. NMN sits in a regulatory grey zone (more on that below).
- Price. Pure NMN tends to run roughly 30 to 80% more expensive per gram than NR, depending on supplier and form.
- Side-effect profile. Both look clean at typical doses. Users report mild flushing or sleep changes with high doses of either, in line with the published trial data on NAD precursor tolerability.
If you find yourself paralysed between the two, that's reasonable. The honest research summary is that both raise NAD+ in the blood, neither has shown a dramatic life-extension effect in humans, and the form difference matters less than the dose and the delivery route.
What does the human research actually show on NMN and NAD precursors?
Most comparison pages list animal studies and call it research. The human trial picture is more modest, and more useful. Here's the short version of what's actually been measured in people.
NR human trials
The strongest dataset belongs to NR. A 2016 study reported NR is "uniquely and orally bioavailable" and raised blood NAD+ after a single dose (Trammell 2016). A 2019 placebo-controlled trial in overweight adults reported NR was well tolerated and raised whole-blood NAD+ by 22%, 51% and 142% at doses of 100, 300 and 1,000 mg daily over eight weeks (Conze 2019). Other studies in older adults have reported similar NAD+ increases without major safety concerns at doses up to 1,000 mg per day (Martens 2018).
NMN human trials
NMN's human file is younger but growing. A 2021 randomised trial in prediabetic postmenopausal women found 250 mg of NMN daily for 10 weeks improved muscle insulin sensitivity (Yoshino 2021). A 2022 randomised, double-blind trial in healthy adults reported that 250 mg daily of NMN for 12 weeks was safe and raised blood NAD+ levels (Yamauchi 2022). Earlier safety work also confirmed single oral NMN doses up to 500 mg were well tolerated in healthy men (Irie 2020).
Direct NAD+ trials
Studies that measured oral NAD+ itself, as opposed to a precursor, are scarce. Most NAD+ raising trials in humans use NR or NMN, or an intravenous infusion of NAD+ for clinical contexts. Oral capsules of NAD+ have not produced the same scale of evidence.
So when a bottle labelled "NAD+" claims trial-backed efficacy, ask which trial, on which molecule. In our experience, the answer is usually a trial on NR or NMN, with the result quietly carried across to a different product.
Why does the form matter less than the delivery route?
This is the part most NMN-vs-NAD pages won't tell you, because it complicates the sales pitch. The form on the label (NMN, NR, NAD+) is one variable. The delivery route (swallowed, sublingual, injected) is another. Research suggests the second variable does more of the heavy lifting than the first.
When you swallow any of these molecules, three things happen before they reach your bloodstream:
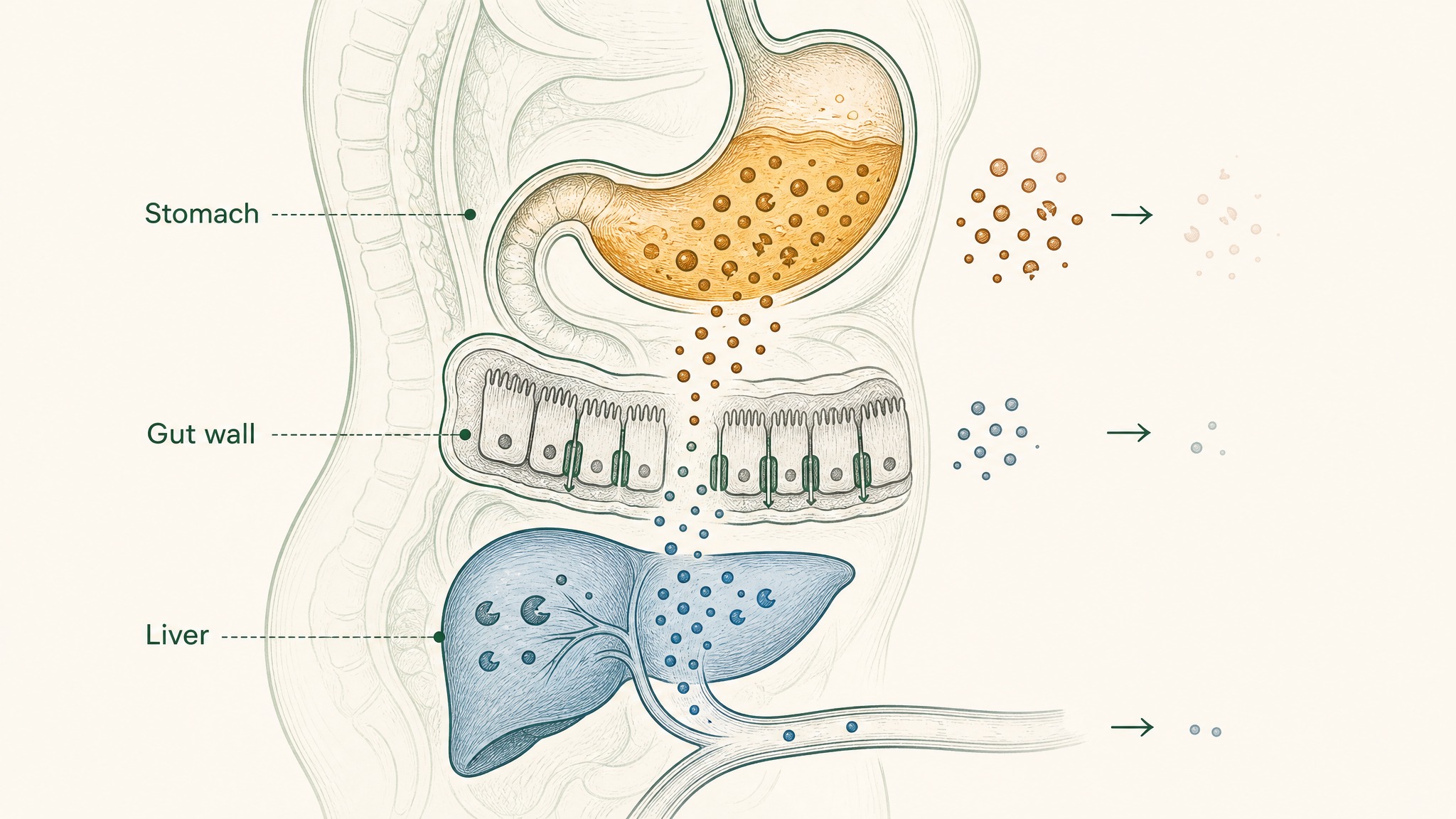
Why swallowing NAD+ precursors loses 98% of the dose before reaching your blood.
- The stomach. Acid and digestive enzymes break a large fraction of the dose down before it can absorb.
- The gut wall. Even the survivors face transporters that may or may not let them through intact.
- The liver. Anything that makes it through the gut hits a first-pass clearance, which strips away another large fraction before the molecule enters general circulation.
The result is well documented for large, charged molecules: oral bioavailability sits in the low single digits for most peptides and many nucleotides. A recent review of the field summarised the upper bound at roughly 1 to 2% for unmodified peptides taken by mouth (Drucker 2020).
That's the gap VERISORB sublingual delivery was designed to close, and the reason LEGACY places NAD+ precursor work behind the tongue rather than in a capsule. Bypass the stomach and the liver, and the form question (NMN vs NR vs NAD+) becomes a much smaller lever than the route.
What about NMN safety and the regulatory situation?
The NMN side of the NMN-vs-NAD-supplement question carries a regulatory wrinkle most product pages don't mention. In late 2022 the US Food and Drug Administration declared NMN ineligible to be sold as a dietary supplement under the New Dietary Ingredient framework, on the grounds it had been authorised for investigation as a drug (FDA NDI ruling on NMN, 2022).
What that means in practice:
- NMN is still widely sold online in 2026, but its legal status in the US is contested.
- Major retailers like Amazon have intermittently removed NMN listings in response to FDA guidance.
- NR remains sold openly as a supplement in the same period.
Outside the US the picture is different. The UK, EU, Canada, Australia, and most of Asia regulate NMN under their own frameworks, and several allow it as a supplement. None of that affects the underlying biology. It does affect price, availability, and what you can verify on a Certificate of Analysis.
On safety, the published human trials of NMN at doses up to 900 mg daily report broadly clean tolerability profiles, with the main reported events being mild gastrointestinal symptoms or sleep changes (Yoshino 2021; Yamauchi 2022; Irie 2020). Long-term human safety data beyond 12 to 16 weeks is still thin for both NMN and NR.
How should you actually choose between NMN and an NAD+ supplement?
Strip out the marketing, and the decision tree is shorter than the supplement industry suggests. Here's the framework we use when members ask:
- Confirm what's actually in the bottle. A product labelled "NAD+" should still list its active ingredient by name (NMN, NR, or another precursor). If it doesn't, that's a signal to walk away.
- Look at the delivery route before the form. A sublingual lozenge or oral spray of NMN at 100 mg can deliver more usable molecule than a 500 mg capsule, because more of it bypasses the gut and liver.
- Match the dose to a published trial. Look for products in the range studied in real people: NR 250 to 1,000 mg daily, NMN 250 to 900 mg daily. Either much less or much more should make you ask why.
- Check the Certificate of Analysis. A third-party COA on the exact batch you're holding tells you whether the listed dose is real. We walk through this step-by-step in our NAD supplement audit framework.
- Read the brand's silence as data. If a brand won't tell you the absorption route, the test method, or the regulatory status of NMN in your country, that silence is the answer.
Most buyers fixate on step 1 and skip steps 2 through 5. The order matters. The molecule on the label is a small part of whether a product does what it claims.
Frequently asked questions
Is NMN the same as NAD?
No. NMN (nicotinamide mononucleotide) is a precursor your body converts into NAD+ in one chemical step. NAD+ (nicotinamide adenine dinucleotide) is the finished cellular fuel itself. Most bottles labelled "NAD supplement" actually contain a precursor like NMN or NR, not NAD+ in its final form.
Which is more effective: NMN or NAD supplements?
In head-to-head terms, NMN is generally a more practical oral choice than a capsule of NAD+ itself, because NMN is smaller and more stable in the gut. Research suggests properly dosed NMN raises blood NAD+ levels in humans, while oral NAD+ capsules have far less published human evidence behind them. The form on the label matters less than the delivery route and the dose.
Can you take NMN and NAD together?
Most "NAD+" supplements on the market are precursors themselves, so taking both would usually mean stacking two precursors. Several clinical trials have studied NMN and NR independently, but there is limited published human data on combining a precursor with direct NAD+ supplementation. Users report stacking them anecdotally with no obvious safety issues at typical doses, though the published trial picture remains thin.
Is NMN banned by the FDA?
The US FDA ruled in 2022 that NMN cannot be sold as a dietary supplement under the New Dietary Ingredient framework, because it had been authorised for investigation as a drug (FDA NDI guidance on NMN). NMN is still widely sold in 2026, but its US supplement status remains contested. Outside the US, regulatory treatment varies by country.
What's the best NMN dose for raising NAD+?
Published human trials cluster between 250 mg and 900 mg of NMN daily, with measurable NAD+ increases reported across that range (Yoshino 2021; Yamauchi 2022; Irie 2020). The right dose for any individual depends on body weight, age, baseline NAD+ levels, and goal. Higher is not automatically better, and long-term human safety data above 1,000 mg per day is still limited.
Key Takeaways
- "NAD supplement" almost always means a precursor (NMN or NR), not NAD+ itself in the bottle.
- NMN sits one chemical step closer to NAD+ than NR, and is smaller and more stable than direct NAD+ in capsule form.
- Both NMN and NR have human trial evidence supporting an NAD+ rise in the blood at properly studied doses.
- The delivery route (sublingual, oral, injected) is a bigger lever than the form on the label for usable, in-blood NAD+.
- NMN's US supplement status is contested by the FDA as of late 2022; NR remains openly sold as a supplement.
- Choose by checking the delivery route, the dose vs human trials, and the Certificate of Analysis, in that order.
References
- Massudi, H. et al. (2012). Age-associated changes in oxidative stress and NAD+ metabolism in human tissue. PLOS ONE. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0042357. Retrieved 2026-06-23.
- Verdin, E. (2015). NAD+ in aging, metabolism, and neurodegeneration. Science, 350(6265). https://www.science.org/doi/10.1126/science.aac4854. Retrieved 2026-06-23.
- Camacho-Pereira, J. et al. (2016). CD38 dictates age-related NAD decline and mitochondrial dysfunction through a SIRT3-dependent mechanism. Cell Metabolism. https://www.cell.com/cell-metabolism/fulltext/S1550-4131(16)30224-9. Retrieved 2026-06-23.
- Trammell, S. A. et al. (2016). Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nature Communications. https://www.nature.com/articles/ncomms12948. Retrieved 2026-06-23.
- Martens, C. R. et al. (2018). Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications. https://www.nature.com/articles/s41467-018-03421-7. Retrieved 2026-06-23.
- Conze, D. et al. (2019). Safety and metabolism of long-term administration of NIAGEN (nicotinamide riboside chloride) in a randomized, double-blind, placebo-controlled clinical trial of healthy overweight adults. Scientific Reports. https://www.nature.com/articles/s41598-019-46120-z. Retrieved 2026-06-23.
- Irie, J. et al. (2020). Effect of oral administration of nicotinamide mononucleotide on clinical parameters and nicotinamide metabolite levels in healthy Japanese men. Endocrine Journal. https://www.jstage.jst.go.jp/article/endocrj/67/2/67_EJ19-0313/_article. Retrieved 2026-06-23.
- Drucker, D. J. (2020). Advances in oral peptide therapeutics. Nature Reviews Drug Discovery. https://www.nature.com/articles/s41573-019-0053-0. Retrieved 2026-06-23.
- Yoshino, M. et al. (2021). Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science, 372(6547). https://www.science.org/doi/10.1126/science.abe9985. Retrieved 2026-06-23.
- Yamauchi, T. et al. (2022). Randomized, double-blind, placebo-controlled trial of nicotinamide mononucleotide. Frontiers in Nutrition. https://www.frontiersin.org/articles/10.3389/fnut.2022.868640/full. Retrieved 2026-06-23.
- US Food and Drug Administration. (2022). New Dietary Ingredient Notification response on beta-nicotinamide mononucleotide. FDA NDI Notification database. https://www.fda.gov/food/new-dietary-ingredients-ndi-notification-process/new-dietary-ingredients-notifications-and-related-correspondence. Retrieved 2026-06-23.
Curious how a sublingual NAD+ precursor protocol is built around the delivery route, not the molecule on the label? Explore the LEGACY protocol →
LEGACY™
NAD+Engineered around 300mg NAD+. Replenishes systemic NAD+ levels and drives mitochondrial function
Clinical Context
Important Notice: VERO protocols are nutritional and systemic optimisation formats. They are not intended to diagnose, treat, cure, or prevent any medical condition. These statements have not been evaluated by the Food and Drug Administration.